Adhesión)al)tratamiento)en)la) - ACCU-ASTURIAS · PDF filea Department of Medicine I,...
38
Adhesión al tratamiento en la enfermedad inflamatoria intes2nal Dr. Ignacio MarínJiménez Unidad enfermedad inflamatoria intes/nal Hospital Universitario Gregorio Marañón Madrid
Transcript of Adhesión)al)tratamiento)en)la) - ACCU-ASTURIAS · PDF filea Department of Medicine I,...

§ Adhesión al tratamiento en la enfermedad inflamatoria intes2nal
Dr. Ignacio Marín-‐Jiménez
Unidad enfermedad inflamatoria intes/nal Hospital Universitario Gregorio Marañón
Madrid

Esquema de adhesión en EII
• Definiciones
• Importancia
• Causas
• ¿Cómo detectarla?
• Estrategias de mejora

Esquema de adhesión en EII
• Definiciones
• Importancia
• Causas
• ¿Cómo detectarla?
• Estrategias de mejora
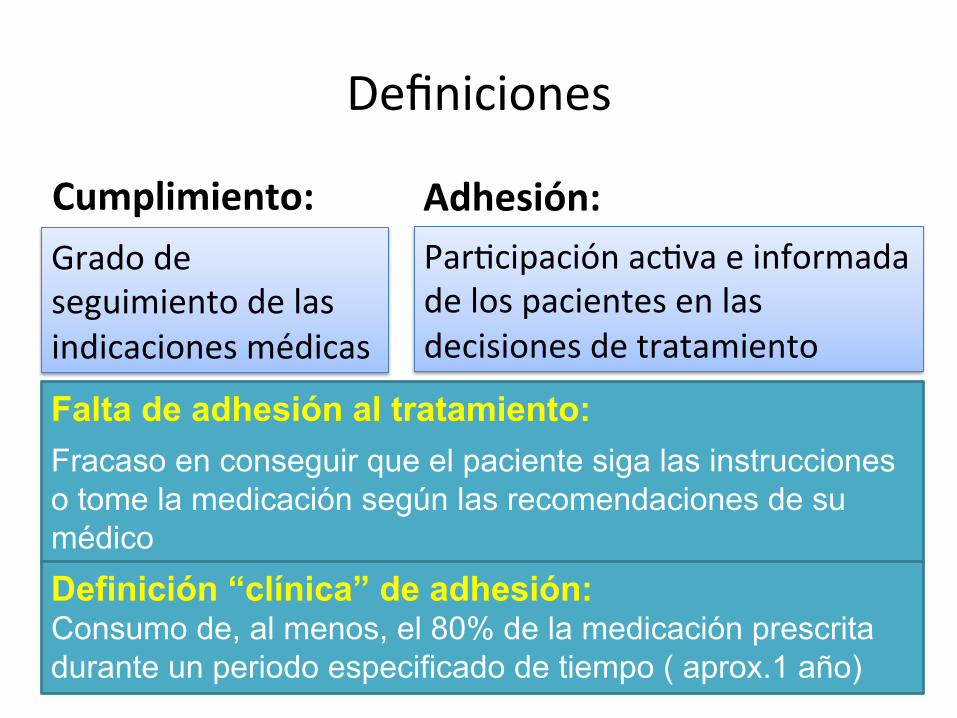
Definiciones
Falta de adhesión al tratamiento:
Fracaso en conseguir que el paciente siga las instrucciones o tome la medicación según las recomendaciones de su médico Definición “clínica” de adhesión: Consumo de, al menos, el 80% de la medicación prescrita durante un periodo especificado de tiempo ( aprox.1 año)
Cumplimiento: Adhesión: Grado de seguimiento de las indicaciones médicas
Par@cipación ac@va e informada de los pacientes en las decisiones de tratamiento

¿Qué implica la adhesión?
ü Que el paciente y el médico colaboran para conseguir un objetivo común
ü Que las decisiones médicas han de tener en
cuenta • quién es el paciente • qué necesita el paciente
Tipos de falta de adhesión
• No intencionada: involuntaria, pasiva (65-80%)
• Intencionada: voluntaria, activa (20-35%)

Patrones de pacientes según ac@tud
Horne R. et al. Inflamm Bowel Dis 2009 Robinson A, Aliment Pharmacol Ther 2008
p Teacher´s pet
(“pelota”)
p Distractible
(distraído)
p Gambler
(apostador)
p Rebel (rebelde)

Adhesión según tipo de actitud
Moshkovska T et al, Aliment Pharm Ther 2009 Horne R. et al. Inflamm Bowel Dis 2009

Esquema de adhesión en EII
• Definiciones
• Importancia
• Causas
• ¿Cómo detectarla?
• Estrategias de mejora
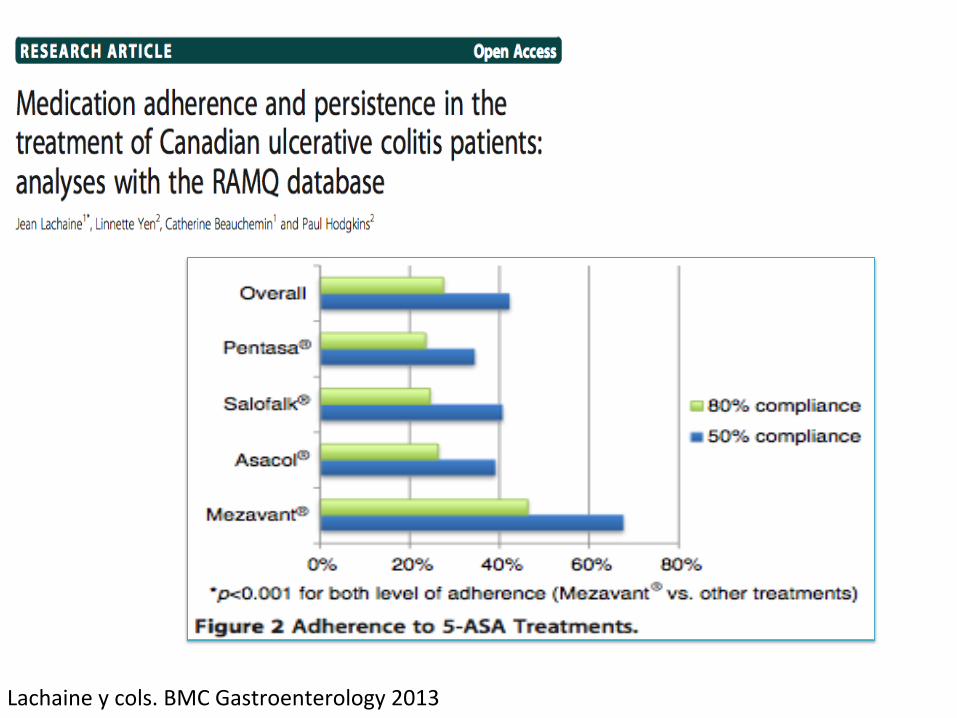
Lachaine y cols. BMC Gastroenterology 2013

Lachaine y cols. BMC Gastroenterology 2013

Pero en otros estudios la adherencia es muy buena… sospechosamente buena…
Schreiber y cols. J Crohns Colitis 2013
National differences in ulcerative colitisexperience and management among patientsfrom five European countries and Canada:An online surveyStefan Schreiber a,⁎,1, Julián Panés b,1, Edouard Louis c,1, Derek Holley d,Mandy Buch d, Kristine Paridaens e
a Department of Medicine I, University Hospital Schleswig-Holstein, Christian Albrechts University, Schittenhelmstr. 12,24105 Kiel, Germanyb Department of Gastroenterology, Hospital Clínic of Barcelona, Villarroel 170, 08036 Barcelona, Spainc Department of Gastroenterology, University Hospital of Liège (CHU), Liège University, 4000 Liège, Belgiumd GfK Healthcare Division, Ludgate House, 245 Blackfriars Road, London, SE1 9UL, United Kingdome Shire AG, Business Park Terre-Bonne, Route de Crassier 7, 1296 Eysins, Switzerland
Received 23 February 2012; received in revised form 24 May 2012; accepted 25 July 2012
KEYWORDSUlcerative colitis;Inflammatory boweldisease;Large intestine;Abdominal pain
Abstract
Background and aims: Patients' and physicians' perceptions of ulcerative colitis and itsmanagement are important for developing and guiding appropriate therapies. This studyexplored national differences in patients' and physicians' experiences, expectations, and beliefsabout ulcerative colitis.Methods: Structured, cross-sectional, online surveys evaluating various indices were completedby 775 adult patients with ulcerative colitis and 475 physicians actively managing ulcerativecolitis patients from France, Germany, Ireland, Spain, the United Kingdom, and Canada.Results: Patients' classification of their symptom severity differed across countries (mild, 16%–45%; moderate, 46%–58%; severe, 4%–36%). Expectations of disease control also varied, with 26%(Ireland) to 65% (Spain) describing that remission realistically involves “living withoutsymptoms.” Within each country, more patients (45%–69%) than physicians (28%–45%)considered ulcerative colitis symptoms to affect patients' quality of life. Mean number ofpatient-reported flares during the past year ranged from 2.5 in Ireland to 8.0 in France.Self-reported adherence with oral 5-aminosalicylic acid (during remission) was highest in Spain(91% vs 50%–73% across other countries). Spanish patients were more likely to self-adjust their
⁎ Corresponding author. Tel.: +49 431 597 2350; fax: +49 431 597 1302.E-mail addresses: [email protected] (S. Schreiber), [email protected] (J. Panés), [email protected] (E. Louis),
[email protected] (D. Holley), [email protected] (M. Buch), [email protected] (K. Paridaens).1 On behalf of the international patient/healthcare provider survey study working group.
1873-9946/$ - see front matter © 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.crohns.2012.07.027
Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Journal of Crohn's and Colitis (2013) 7, 497–509

Schreiber y cols. J Crohns Colitis 2013
cultural factors, combined with differing treatment prac-tices and health service organization. Learning to recognizethese factors and address them during therapy may improvetreatment outcomes and the standard of healthcare avail-able to patients with UC in specific countries.
Supplementary data to this article can be found online athttp://dx.doi.org/10.1016/j.crohns.2012.07.027.
Conflict of interest
Stefan Schreiber has received consultancy and speaker feesfrom Shire that were not related to this article; has receivedlecture fees from the Falk Foundation; and has consulted forvarious companies developing novel biologic agents. JuliánPanés has received consultancy fees from Abbott, Bristol‐Myers Squibb, Cellerix, Genentech, MSD, Novartis, PalauPharma, Pfizer, and Roche; has received speaker fees fromAbbott, Ferring, MSD, Shire, and Tillotts Pharma; and hasreceived unrestricted research grants from Abbott and MSD.Edouard Louis has received consultancy fees from ScheringPlough, Abbott, MSD, Ferring, Shire, Millennium, and UCB; hasreceived research or educational grants from MSD, ScheringPlough, Astra Zeneca, Abbott; and has received lecture fees
from Abbott, Astra Zeneca, Ferring, MSD, Schering Plough,Falk, Menarini, Chiesi, and Nycomed. Derek Holley and MandyBuch are employees of GfK Healthcare Division, which wascontracted by Shire to conduct this research. KristineParidaens is an employee of Shire.
Acknowledgments
All authors were involved in the conception and design of the study,the analysis and interpretation of data, and the drafting of themanuscript or revising it critically for important intellectualcontent. DH and MB were responsible for data acquisition. Allauthors approved the final submitted version. The authors wish toacknowledge Nicholas Pym, an employee of Apollo Market Intelli-gence Ltd. and a consultant to Shire, for administrative oversight forthe surveys. The market research, which was conducted by GfKHealthcare Division (London, United Kingdom), was funded by theSponsor, Shire Development LLC. Under the direction of theauthors, Andrew Brittain, an employee of GeoMed, and WilsonJoe, an employee of MedErgy, provided writing and editorialassistance for this publication (including formatting, proofreading,copy editing, and fact checking), which was funded by ShireDevelopment LLC. Representatives from Shire Development LLCand Shire Pharmaceutical Development Ltd also reviewed themanuscript for scientific accuracy. Although the Sponsor was
Table 3 Attitudes of patients from different countries towards 5-ASA treatment.
Characteristic Canada(n=64)
France(n=54)
Germany(n=74)
Ireland(n=26)
Spain(n=141)
UK(n=84)
Adherence to 5-ASA, %a
Always took most or all of my medication that my doctorwanted me to
64b 50b 53b 73 91b 52b
Tried taking fewer tablets than prescribed(but did not stop)
30c,d 24c 15d 8 9c 23c
Tried not taking medication at all for a period of time 6e,f 26e,f 32e,f 19 0e 25e,f
Satisfaction with 5-ASA, %a
Very satisfied/happy 58g 20g 28g 15 18g 44g
Somewhat satisfied/happy 41h 69h 49h 58 40h 46h
Not very satisfied/happy 2i.j 9i 15i,j 12 38i 8i
Not at all satisfied/happy 0k 2 8k 15 4 1k
UK, United Kingdom; 5-ASA, 5-aminosalicylic acid.aAll respondents who were currently taking daily oral 5-ASA medication for UC; percentages may not total 100% due to rounding.Values without footnotes were not significantly different from other values.Adherence to 5-ASA.“Always took most or all of my medication that my doctor wanted me to.”bCanada, France, Germany, and UK Pb0.05 vs Spain.“Tried taking fewer tablets than prescribed (but did not stop)”.cCanada, France, and UK Pb0.05 vs Spain.dCanada Pb0.05 vs Germany.“Tried not taking medication at all for a period of time”.eCanada, France, Germany, and UK Pb0.05 vs Spain.fCanada Pb0.05 vs France, Germany, and UK.Satisfaction with 5-ASA, %.“Very satisfied/happy”.gCanada and UK Pb0.05 vs France, Germany, and Spain.“Somewhat satisfied/happy”.hCanada, Germany, Spain, and UK Pb0.05 vs France.“Not very satisfied/happy”.iCanada, France, Germany, and UK Pb0.05 vs Spain.jCanada Pb0.05 vs Germany.“Not at all satisfied/happy”.kCanada and UK Pb0.05 vs Germany.
507National differences in ulcerative colitis perceptions
Nuestros pacientes se toman el tratamiento con mesalazina mejor que nadie… pero son los más
descontentos con dicho tratamiento… …???
Pero en otros trabajos la adherencia es muy buena… sospechosamente buena…
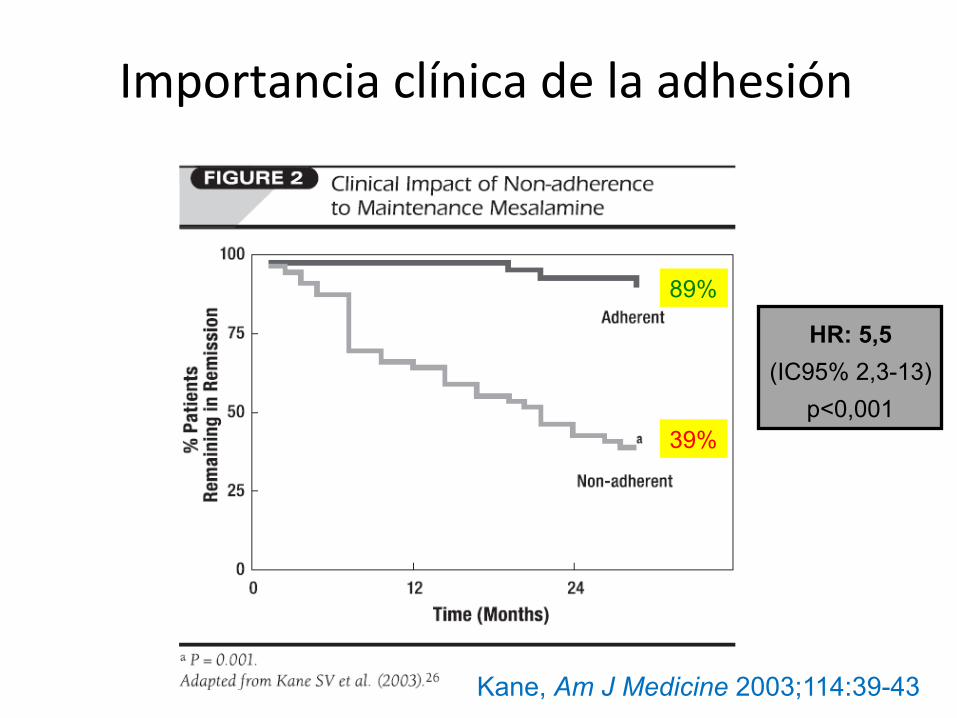
Importancia clínica de la adhesión
Kane, Am J Medicine 2003;114:39-43
89%
39%
HR: 5,5 (IC95% 2,3-13)
p<0,001
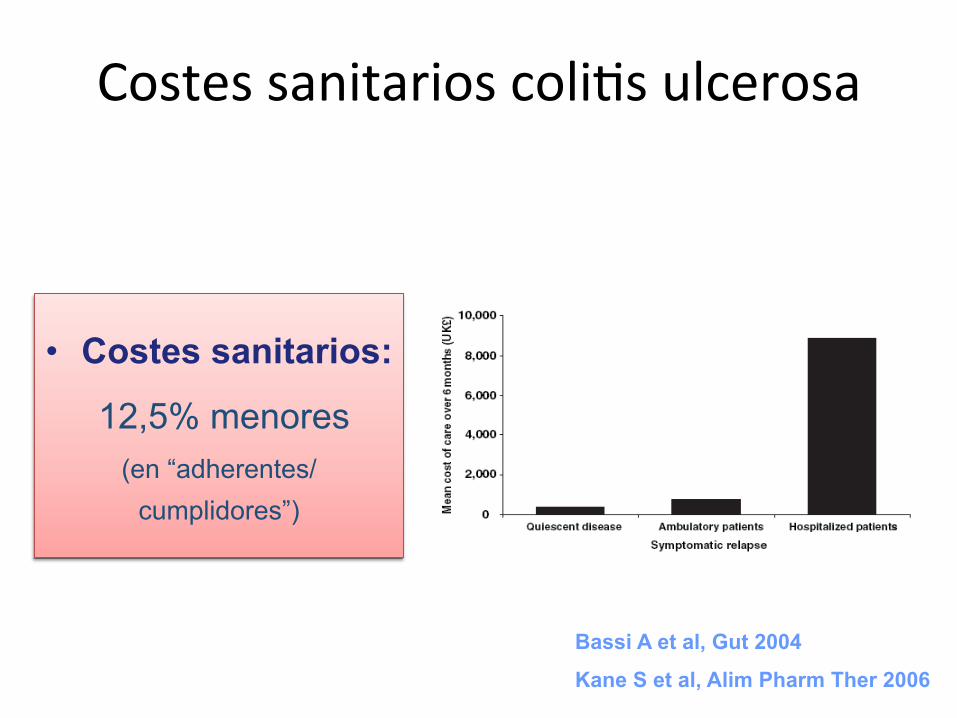
Costes sanitarios coli@s ulcerosa
• Costes sanitarios:
12,5% menores (en “adherentes/
cumplidores”)
Bassi A et al, Gut 2004
Kane S et al, Alim Pharm Ther 2006
Costes en EII
“Sabemos que puede ser caro tomar medicamentos, pero puede ser aún más caro no tomarlos”
Suhananda Kane

Esquema de adhesión en CU
• Definiciones
• Importancia
• Causas
• ¿Cómo detectarla?
• Estrategias de mejora

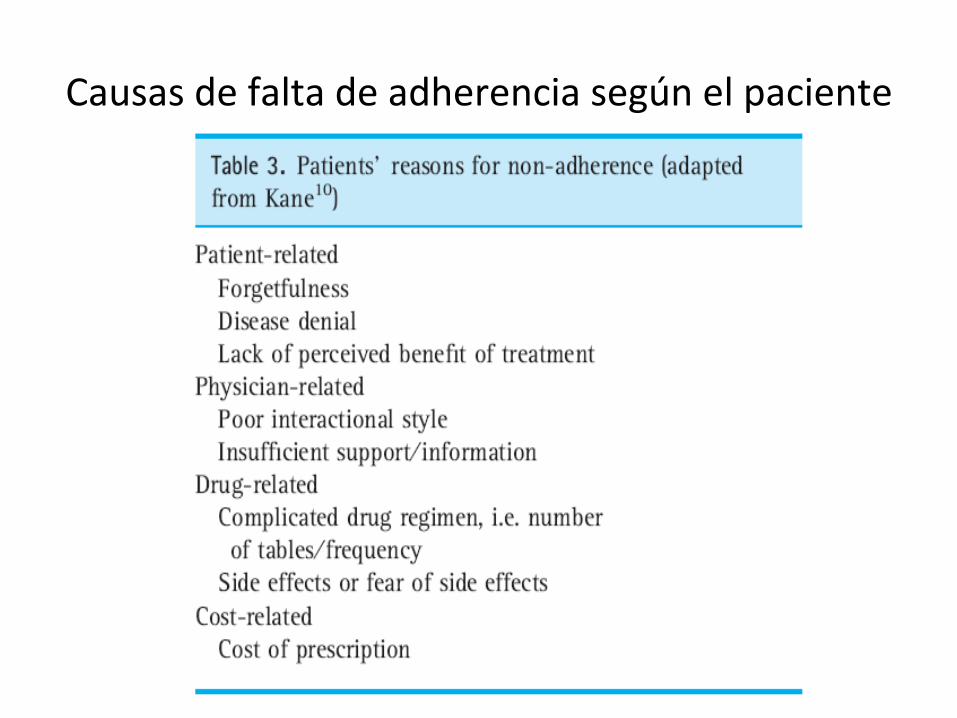
Causas de falta de adherencia según el paciente
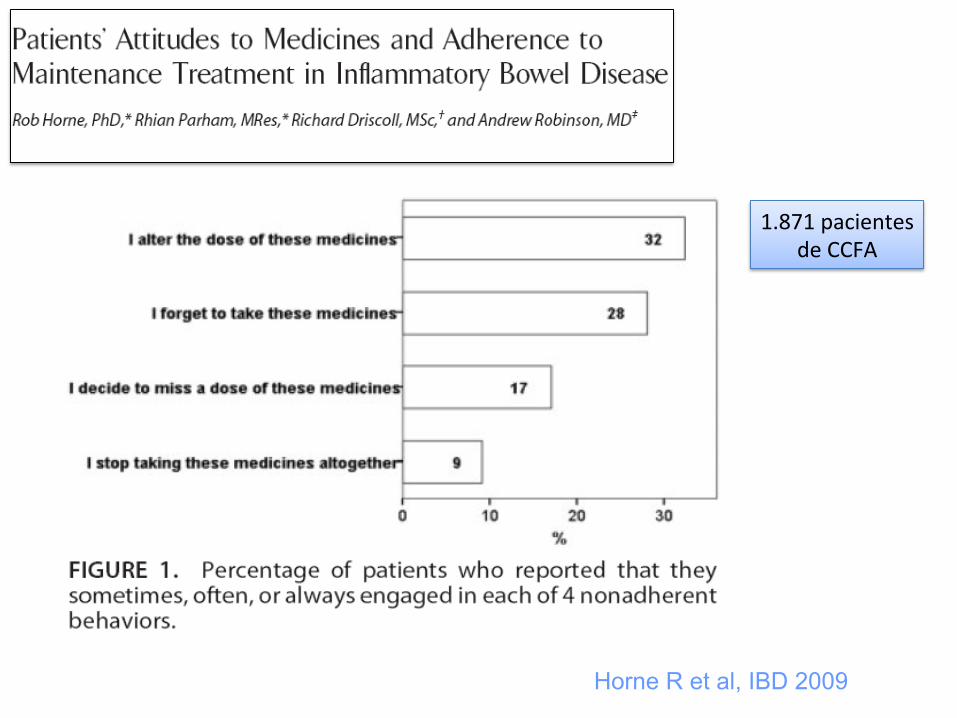
Horne R et al, IBD 2009
1.871 pacientes de CCFA

Adhesión y @po de tratamiento
Horne R et al, IBD 2009

Nahon et al, IBD 2011

• Psychological distress,
• Patient’s beliefs about medications
• Doctor–patient discordance
• Demographic, clinical, and treatment variables were
not consistently associated with non-adherence
(tendencia en complejidad tratamiento)
Jackson CA et al. Am J Gastro 2010
Esquema de adhesión en CU
• Definiciones
• Importancia
• Causas
• ¿Cómo detectarla?
• Estrategias de mejora
Dificultad de medida de la adhesión
Efecto Hawthorne
• Fábricas Chicago • 1924-‐32 • Efectos de los cambios de luz sobre el rendimiento laboral de los trabajadores

Métodos de diagnós@co de falta de adhesión
• Métodos:
– Subjetivos: • Encuestas a pacientes (MARS-4, MARS-8) • Encuestas a familiares
– Objetivos: • Contaje de pastillas • Retirada de medicamentos de Farmacia (IANUS) • Medication Possession Ratio (MPR) • Monitorización electrónica • Métodos analíticos (salicilatos, 6-TGN, niveles ADA…)
• Mejor combinar varias medidas (objetivas y subjetivas)
• No hay un patrón-oro

Métodos de diagnós?co de
falta de adhesión: escala de Morisky
modificada para pacientes
con EII

Hommel KA et al, IBD 2009

Esquema de adhesión en CU
• Definiciones
• Importancia
• Causas
• ¿Cómo detectarla?
• Estrategias de mejora
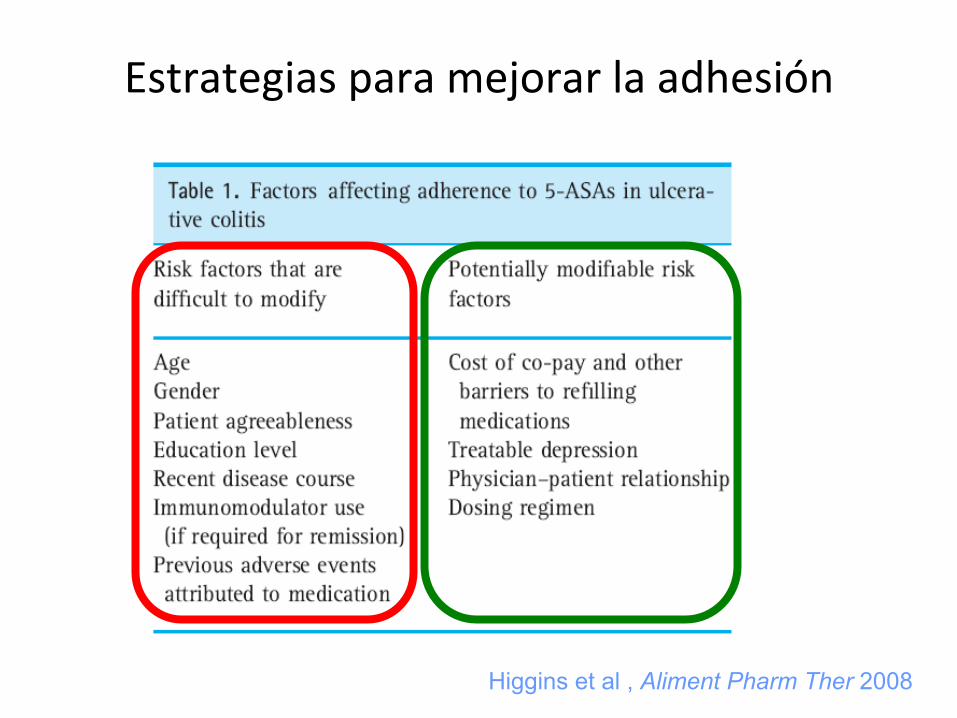
Estrategias para mejorar la adhesión
Higgins et al , Aliment Pharm Ther 2008
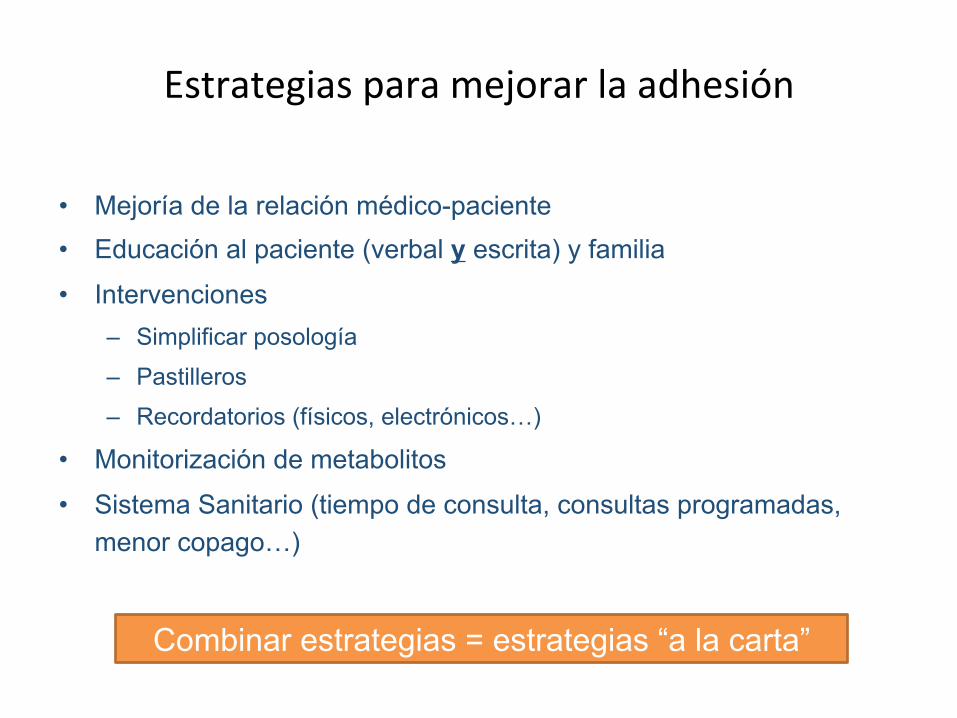
Estrategias para mejorar la adhesión
• Mejoría de la relación médico-paciente • Educación al paciente (verbal y escrita) y familia
• Intervenciones – Simplificar posología
– Pastilleros
– Recordatorios (físicos, electrónicos…)
• Monitorización de metabolitos
• Sistema Sanitario (tiempo de consulta, consultas programadas, menor copago…)
Combinar estrategias = estrategias “a la carta”
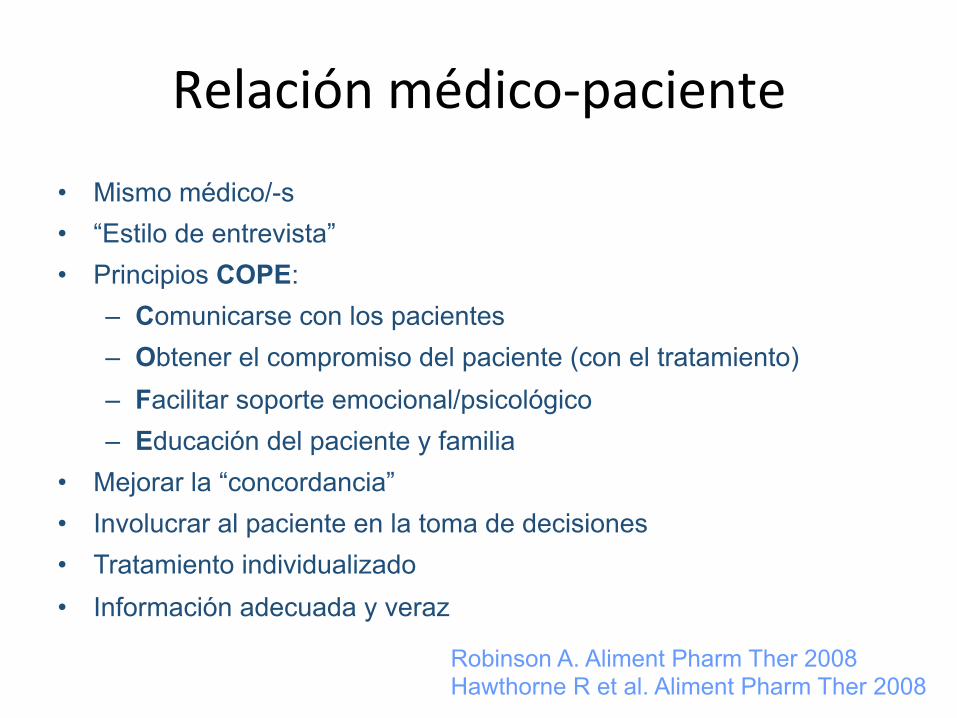
Relación médico-‐paciente
• Mismo médico/-s • “Estilo de entrevista” • Principios COPE:
– Comunicarse con los pacientes – Obtener el compromiso del paciente (con el tratamiento) – Facilitar soporte emocional/psicológico – Educación del paciente y familia
• Mejorar la “concordancia” • Involucrar al paciente en la toma de decisiones • Tratamiento individualizado • Información adecuada y veraz
Robinson A. Aliment Pharm Ther 2008 Hawthorne R et al. Aliment Pharm Ther 2008
Tratamiento ideal según el paciente
• Alta eficacia (97%)
• Ausencia de efectos secundarios (74%)
• Oral (46%)
• Pocas pastillas (23%)
• Dosis poco frecuente (23%)
• Barato (23%)
Loftus el al, IBD 2006

Claxton et al. Clin Ther 2001.
Importancia de la dosificación

Moshkovska et al. IBD 2011(e-pub)
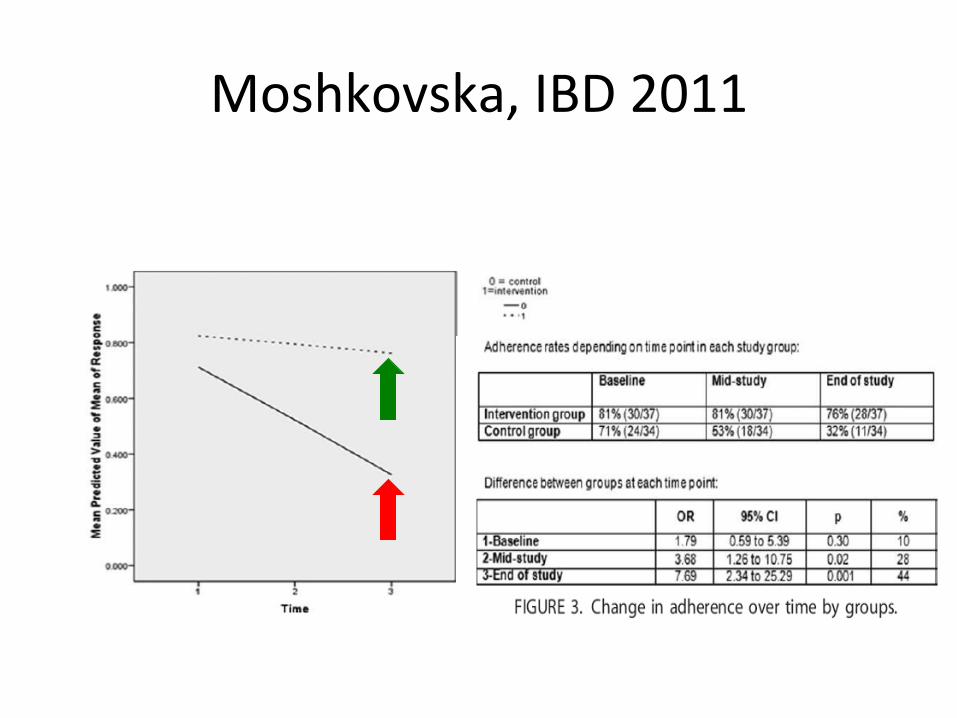
Moshkovska, IBD 2011

Conclusiones (1)
• La falta de adhesión al tratamiento en la EII es frecuente, por lo que debe ser investigada
• La falta de adhesión en la EII tiene consecuencias clínicas y económicas
• La adhesión terapéutica es un proceso complejo y multifactorial

Conclusiones (2)
• La relación médico-paciente y los factores psicológicos del paciente (percepciones, creencias, psicopatologías) son los principales factores que afectan a la adhesión
• Las estrategias combinadas y personalizadas parecen ser el mejor mecanismo para mejorar la adhesión