Clases pregrado piel 1
70
Parte 1 LA PIEL
-
Upload
nayelinieto -
Category
Career
-
view
319 -
download
4
Transcript of Clases pregrado piel 1

Parte 1
LA PIEL

GENERALIDADES

QUE ES LA PIEL?
• Cubierta exterior que reviste todo el cuerpo.
• Órgano complejo anatómico y funcional ligado a la fisiología y patología de todo el organismo.
• Debemos conocerlo en su estado natural para poder comprender su estado patológico
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

LA PIEL EN NÚMEROS
• Extensión varía de acuerdo al peso y talla. • 70 kg. y 1.70 m = 1.85 m2
• Volumen de 4000 mL • Espesor promedio: 2.2 mm • Peso de 4.2 Kg, 6 % peso corporal • Contenido de sangre: 1.8 L, 30 % del
total • Es el órgano mas extenso y de mayor
peso y volumen
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

COMPLEJIDAD DE LA PIEL
En un cm2 de piel hay: • 5 folículos pilosos • 15 glándulas sebáceas • 100 glándulas sudoríparas • 4 metros de nervios • 1 metro de vasos sanguíneos • 5000 terminales sensitivas • 6 millones de células
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

VARIACIONES DE LA PIEL
• Color: Cantidad de pigmento melánico, red vascular (Oxihemoglobina y hemoglobina reducida), carotenos y la dispersión
• Grosor, aspecto y textura • Sexo y edad
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

ESTRATOS EPICUTANEOS
Microatmósfera que rodea la piel del individuo y lo pone en contacto con el medio exterior y son:
1.-Manto gaseoso : Capa de aire mas caliente con mas contenido de C0 2 y vapor de agua resultante de la evaporación del agua.
2.-Manto ácido : Emulsión de la secresión sudoral y sebácea. pH 5.5. (C0 2 y aminoácidos). Ventanas alcalinas
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

COMPONENTES QUIMICOS DE LA PIEL
• Agua • Electrolitos: Cl, Na, K, Mg. y Ca. • Otros minerales: Azufre (radical sulfidrilo), P,
Pb, Mg, Fe, Cu y otros en menor proporción. • Proteínas • Lípidos • Hidratos de Carbono • Enzimas y vitaminas: Citocromoxidasa
(queratinización)
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

FISIOLOGÍA DE LA PIEL
• Estética• Protección:
• Barrera por su cohesion, elasticidad e integridad • Propiedades eléctricas: Carga (-) • Manto acido: Germicida y fungicida
• Sensorial • Termoregulación • Metabolismo en general:
• Absorción y eliminación de sustancias (urea, creatinina) • Función Queratógena • Función Sebácea • Función Melanogénica
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

1. ANATOMÍA.
EPIDERMISDERMISHIPODERMISFANERAS O ANEXOS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

SUPERFICIE DE LA PIEL
• La piel presenta entrantes y salientes, depresiones y orificios
• Las salientes pueden ser • Transitorias: Conos pilosos formados por el músculo
erector del pelo (frío, aspecto de piel de gallina) • Permanentes como los rafes, rollos o “llantas”,
dermatoglifos (huellas dactilares) y pliegues losángicos que siguen la dirección de las líneas de torsión
• Pliegues articulares, musculares • Los orificios corresponden a la desembocadura de las
glándulas sudoríparas (2.5 millones)
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

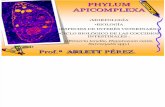
A. EPIDERMIS
E. córneo E. lúcido E. granuloso E. espinoso E. germinativo o basal
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Capa proliferante.Célula basaloideMitosisMelanocitos.
Estrato basal o germinativo.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Estrato espinoso
Estrato granuloso
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Capa más superficial.
Son células muertas, aplanadas, sin núcleo y queratinizadas.
En las áreas sometidas a presiones y roces ( palmoplantares ) es más grueso, mientras que en el resto de la piel es más delgado y flexible.
Estrato córneo.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

OTRAS CÉLULAS
Melanocitos
Células dendríticas
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Células de Merkel
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
• Neuroendocrinas
• Mecanoreceptor

Tejido conjuntivo densoVasos sanguíneos.Vasos linfáticos.MúsculosTerminaciones nerviosasAnexos cutáneos: Folículos pilososGlándulas
D. PAPILAR:Huellas digitales
D. RETICULAR:Redes de colágeno
B. DERMIS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Tejido conectivo y células adiposas: ADIPOCITOS.
También: TEJIDO CELULAR SUBCUTÁNEO O PANÍCULO ADIPOSO.
C. HIPODERMIS:
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

D. ANEXOS CUTÁNEOS
• Complejo Pilosebáceo • Folículo piloso • El pelo • Músculo erector del pelo
• Glándula sebácea • Glándulas sudoríparas : Ecrinas y
apocrinas • Uñas
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

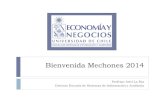
PELO
PELO: (Médula y cutícula)RAIZ (Bulbo)TALLO
MÚSCULO ERECTOR
GLÁNDULA SEBÁCEA
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

TERMORREGULACIÓN ABSORCIÓN PROTECCIÓN Microorganismos Traumatismos Agentes extraños Radiación UV.
EXCRECCIÓN
SENSORIAL
SECRECIÓN: Sudor Sebo Queratina Cera
METABÓLICA: Vit D
2. FISIOLOGÍA:
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

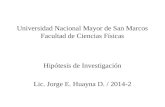
3.PATOLOGÍA DE LA PIEL

Definiciones de los términos macroscópicos
Mácula. Coloración <5mm, lisa
Placa: >5mm.
Pápula, lesión elevada cupuliforme <5mm
Nódulo: lesión elevada >5mm.
Vesícula: Rellena de líquido <5mm.
Bulla: líquido >5mm.
Pústula = Lleno de pus
Roncha = lesión elevada, pruriginosa, transitoria, con eritema
Escama = Placa cornea seca (queratinización anormal)
Excoriación = Rotura de dermis, puntiformes.Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

DE LA COLORACIÓN MACULA ERITEMATOSA ANGIOMA MACULA PURPÚREA TELANGIECTASIA MÁCULA HIPERCRÓMICA MACULA HIPOCRÓMICA
LESIONES ELEMENTALES PRIMARIAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Mácula pigmentaria hipercrómica
Mácula pigmentaria hipocrómica
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

SÓLIDASPÁPULAPLACARONCHA O HABÓNNÓDULOTUMOR
LESIONES ELEMENTALES PRIMARIAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

MÁCULAS ERITEMATOSAS
Mancha rojiza de origen vascular.
Si aparecen simultáneamente hablamos de exantema.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

MÁCULAS PURPÚREAS
TELANGIECTASIAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

LESIONES AMPOLLOSAS VESÍCULA AMPOLLA PÚSTULA QUISTE
LESIONES ELEMENTALES PRIMARIAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

1.Mácula. 2. Roncha.3. Nódulo. 4.Tumor
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

VESÍCULAS
AMPOLLAS
PÚSTULAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

EROSIÓN EXCORIACIÓN FISURA O RÁGADE ÚLCERA
LESIONES ELEMENTALES SECUNDARIAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

ESCAMA COSTRA ESCARA ATROFIA
ESCLEROSIS CICATRIZ LIQUENIFICACIÓN
LESIONES POR MODIFICACIÓN DE LESIONES PRIMITIVAS
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Términos microscópicos
Hiperqueratosis = Engrosamiento corneoParaqueratosis = NúcleosOrtoqueratosis = Sin núcleos
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Hipergranulosis = Hiperplasia granular
Fricción
Acantosis = Hiperplasia espinosa.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Espongiosis = Edema intercelular.Hinchazón hidrópica (balloning)= Edema intracelular, virus.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Papilomatosis = Elevación irregular en
superficie.
Disqueratosis = Queratinización anormal.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Acantolisis = Pérdida de uniones intercelulares
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Exocitosis = Células inflamatorias intraepidérmicas.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Erosión = Pérdida incompleta de la epidermis.Ulceración = Pérdida completa de piel
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Vacuolización = Vacuolas, generalmente capa
basal.
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Lentiginoso = Proliferación melanocítica
lineal
Patología estructural y funcional de Robbins, 8ª ed, 2010Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

INFECCIONES CUTÁNEAS

INFECCIONES BACTERIANAS -- PIODERMA
Infección cutánea bacteriana• Superficial• Profunda IMPÉTIGO
• Contagioso o no buloso Estreptococos A• Buloso S. aureus (Sx piel escaldada).
Contagioso• Niños• Vesiculopústulas frágiles• Glomerulonefritis
ocasional• Vesículas en capa
granular• Neutrófilos• Espongiosis• Cocos ocasionales Barnhill’s Dermatopathology, 4ª ed, 2008
Lever’s Histopathology of the skin 9ª ed, 2005

Buloso
• Niños < 5 años (neonatos)• Vesiculopústulas confluentes• Generalizado Indistinguible de Ritter• Poca inflamación y es dérmica
Sx piel escaldada (Ritter)• Menores de 5 años• Eritema, fiebre, bullas con líquido seroso • Denudación• Mortal en 4% niños, pero en 50% de adultos• No se demuestra estafilococo en las heridas• Ampolla subcornea• Prácticamente no hay inflamación.
Ectima = Impétigo contagioso ulcerado
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

ERISIPELA
• Celulitis superficial por Estreptococos grupo A• Área roja circunscrita, bien demarcada, indurada• Raro Fascicitis necrosante, cardiopatía y GMN• Dermis con edema e infiltrado por neutrófilos• Cocos en dermis y linfáticos.
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

FASCIITIS NECROSANTE
• Estreptococos A beta hemolíticos, Estafilococo, Hemofilus y otros.
• Celulitis profunda• Traumatismo• Necrosis e inflamación aguda y crónica• Edema y neutrófilos en tejido subcutáneo, fascia y
músculo
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

TUBERCULOSIS
• M. tuberculosis• Rutas:
• Inoculación• Diseminación• Extensión de un ganglio
• Neutrófilos Macrófagos Granulomas caseificantes
• Células de Langhans
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Variantes
Primaria• Raro• Trauma• Chancro tuberculoso
Lúpus vulgar• Nódulos profundos con el tiempo atróficos.• Granulomas pequeños no caseificantes confluentes• Escasos bacilos• Hiperplasia seudoepiteliomatosa

Verrucosa cutánea• Placa verrucosa purulenta en manos, rodillas y
nalgas• Acantosis e hiperqueratosis, abscesos y
granulomas
Miliar cutánea• Inmunocomprometidos• Pápulas o pústulas eritematosas
Escrofuloderma• Trayecto a partir de ganglio rodeado de
granulomas
Goma tuberculoso• Nódulo necrótico ulcerado

Micobacterias no tuberculosas
• Inmunosupresión• Supurativa o granulomatosa• Macrófagos espumosos con micobacterias

LEPRA
• M. leprae• Piel y nervios periféricos• Inhalación• Lepromatosa (respuesta ausente)• Indeterminada • Tuberculoide (alta respuesta)• Acumulo de macrófagos
perineurales, perimisiales, perivasculares
• Dx sólo al demostrar bacilos
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Lepromatosa
• Tipo infiltrativo nodular• Tipo difuso• Histioide
• Infiltrado mixto, predominan macrófagos• Zona de Grenz• Células de Virchow Macrófagos con bacilos
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Tuberculoide
• Granulomas perineurales
• Pocos bacilos
• Eritema nodoso leproso En LL abscesos de
PMN
• Fenómeno de Lucio LLD Endarteritis
obliterante
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

Botriomicosis
• Inmunocompetentes
• Bacterias piógenas
• Inflamación aguda alrededor de
nidos
de bacterias
• Fenómeno de Hoeppli-Splendore
Actinomicosis
• Inmunocompetentes
• A. israelii
• Filamentoso
• Absceso rodeado de
granulación
• Vivos los filamentos
periféricos
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

HERPES
• Edema de queratinocitos• Vesículas con neutrófilos• Acantolisis• Células de Tzank• Células acantolíticas• Inclusiones tipo Cowdry• En VZV el daño es mas severo, vasculitis, vesículas grandes,
hemorragia, microtrombos
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

VERRUGA VIRAL
• Papilomavirus (6 y 8, oncogénicos: 16,18,31,33).
• Niños y adolescentes (cualquier edad).
• Autolimitadas, regresión espontánea
• Tipos:
• Vulgar
• Plana
• Palmar y plantar
• Condiloma
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005Barnhill’s Dermatopathology, 4ª ed, 2008
Lever’s Histopathology of the skin 9ª ed, 2005

Hallazgos patológicos:
1. Acantosis papilomatosa
2. Coilocitosis
3. Hipergranulosis
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

CMV
• Úlceras
• Vasculitis
• Células endoteliales
• Inclusiones nucleares y citoplasmicas
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

MOLUSCO
• Niños y jóvenes con inmunosupresión• Acantolisis y cuerpos de inclusión Henderson -Patterson
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

HIV
• Infecciones oportunistas
• Apoptosis basal
• Edema en los queratinocitos superficiales
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

SÍFILIS
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
Primaria
Chancro erosión, infiltrado plasmacitario.Endarteritis obliterante

Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
Tinciones de plata = Warthin-Starry

Secundaria
Varios patronesHiperplasia psoriasiforme con dermatitis vacuolar de interfase
Infiltrado plasmacitario.Endarteritis obliterante
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005

LEISHMANIASIS
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
• Promastigotes o amastigotes de Leishmania• Localizada, dufusa, crónica cutánea,
Diseminación post Kala-Azar, mucocutánea, visceral
• Histiocitos llenos de parásitos y plasmáticas• Cuerpos de Leishman-Donovan
Microorganismos de 4 mcm, densos con halo claro y cinetoplasto.
• Giemsa, PAS y Gomori.

ESCABIOSIS
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
• S. Scabiei hominis• Túneles o madrigeras Patognomónicos• Túneles negro-rojizos, delgados, mm, al final
hay una vesícula.• Demostrar el ácaro o sus productos.

LARVA MIGRANS CUTÁNEA
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
• Larvas de nemátodos• Contacto con tierra contaminada• Ancylostoma brazilienzis, A. caninum, A.
tubaeformis, Uncinaria stenocephala, Gnathostomum spingerum
• Traycto serpingoso -> Inflamación• Madriguera 1-2 cm adelante.

MORDEDURA DE ARTRÓPODOS
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
• Infiltrado inflamatorio perivascular superficial y profundo en forma de cuña con linfocitos y eosinófilos.
• Espongiosis• En fase crónica puede ser tan intenso o atípico que
semeja linfoma pero es policlonal.

OTROS
Barnhill’s Dermatopathology, 4ª ed, 2008Lever’s Histopathology of the skin 9ª ed, 2005
• CISTICERCOSIS• TUNGIASIS• MIASIS• ESQUISTOSOMIASIS