Coagulopatía Vascular Disemjhkhjhinada
8
585 Disseminated Intravascular Coagulation in T rauma Patients Satoshi Gando, M.D., Ph.D. 1 ABSTRACT Disseminated intravascular coagulation (DIC) is characterized by the in vivo ac- tivation of the coagulation system, which results in the intravascular deposition of fibrin and consumption bleeding. DIC is a serious hemostatic complication of trauma. It can be clearly distinguished from physiological hemostatic response to trauma by using sensitive coagulofibrinolytic molecular markers. Physiological hemostasis to injuries is similar in all kinds of trauma without exception. There is an increase in circulating proinflammatory cytokines in DIC patients after trauma. Elevated cytokines induce tissue factor–mediated activation of coagulation, suppression of the anticoagulant pathway , and plasminogen ac- tivator inhibitor-1 (PAI-1)–mediated inhibition of fibrinolysis followed by disseminated fibrin deposit ion in the micro vascul ature. In addition to the occlusive microv ascular thrombosis and h ypoxia, sustained systemic inflammatory response characterized by neu- trophil activation and endothelial damage plays a pivotal role in the development of mul- tiple organ dysfunction syndrome (MODS) in posttrauma DIC patients. DIC associated with sustained systemic inflammatory response syndrome (SIRS) af ter trauma leads to the develop ment of MODS , which is the mai n determina nt of patients ’ outcom e after trauma. KEYWORDS: Disseminated intravascular coagulation (DIC), trauma, multiple organ dysfunction syndrome (MODS), systemic inflammatory response syndrome (SIRS), inflammation Objectives: Upon completion of this article, the reader should be able to (1) recognize the differences between physiological and pathological hemostatic responses to trauma and ( 2) appreciate the close relationship between DIC, SIRS and MODS in trauma pa- tients. Accreditation: Tufts University School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. TUSM takes full responsibility for the content, quality, and scientific integrity of this continuing education activity. Credit: Tufts University School of Medicine designates this education activity for a maximum of 1.0 hours credit toward the AMA Physicians Recognition A ward in category one. Each physician should claim only those hours that he/she actually spent in the edu- cational activity. Seminars in Thrombosis and Hemostasis , volume 27, number 6, 2001. Address for corr esponden ce and r eprint r equests: Satosh i Gando , M.D. , N15, W7, Kita-ku, Sapporo 060 Japan. E-mail: [email protected]. 1 Divis ion of Acute and Critic al Care Medici ne, Department of Anesthesiology and C ritical Care Medicine, Hokkaido University Graduate School of Med icine, Sapporo, Japan. Copyright © 2001 by Thieme Medical Publ ish ers, Inc ., 333 Seventh Ave nue, New Y ork, NY 10001, USA. T el: +1( 212) 584-4662. 0094 -61 76, p;20 01, 27, 06,585,592 , ftx,en;sth00762x. D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t . C o p y r i g h t e d m a t e r i a l .
Transcript of Coagulopatía Vascular Disemjhkhjhinada

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 1/8
585
Disseminated Intravascular Coagulationin Trauma PatientsSatoshi Gando, M.D., Ph.D.1
ABSTRACT
Disseminated intravascular coagulation (DIC) is characterized by the in vivo ac-tivation of the coagulation system, which results in the intravascular deposition of fibrinand consumption bleeding. DIC is a serious hemostatic complication of trauma. It can be
clearly distinguished from physiological hemostatic response to trauma by using sensitivecoagulofibrinolytic molecular markers. Physiological hemostasis to injuries is similar inall kinds of trauma without exception.There is an increase in circulating proinflammatory cytokines in DIC patients after trauma. Elevated cytokines induce tissue factor–mediatedactivation of coagulation, suppression of the anticoagulant pathway, and plasminogen ac-tivator inhibitor-1 (PAI-1)–mediated inhibition of fibrinolysis followed by disseminatedfibrin deposition in the microvasculature. In addition to the occlusive microvascularthrombosis and hypoxia, sustained systemic inflammatory response characterized by neu-trophil activation and endothelial damage plays a pivotal role in the development of mul-tiple organ dysfunction syndrome (MODS) in posttrauma DIC patients. DIC associated
with sustained systemic inflammatory response syndrome (SIRS) after trauma leads tothe development of MODS, which is the main determinant of patients’ outcome after
trauma.
KEYWORDS: Disseminated intravascular coagulation (DIC), trauma, multiple organ
dysfunction syndrome (MODS), systemic inflammatory response syndrome (SIRS),
inflammation
Objectives: Upon completion of this article, the reader should be able to (1) recognize the differences between physiological and
pathological hemostatic responses to trauma and (2) appreciate the close relationship between DIC, SIRS and MODS in trauma pa-
tients.
Accreditation: Tufts University School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to
provide continuing medical education for physicians. TUSM takes full responsibility for the content, quality, and scientific integrity of
this continuing education activity.
Credit: Tufts University School of Medicine designates this education activity for a maximum of 1.0 hours credit toward the AMAPhysicians Recognition Award in category one. Each physician should claim only those hours that he/she actually spent in the edu-
cational activity.
Seminars in Thrombosis and Hemostasis , volume 27, number 6,2001. Address for correspondence and reprint requests: Satoshi Gando, M.D., N15, W7, Kita-ku, Sapporo 060 Japan. E-mail: [email protected]. 1Division of Acute and Critical Care Medicine, Department of Anesthesiology and Critical Care Medicine, Hokkaido University Graduate School of Medicine, Sapporo, Japan. Copyright © 2001 by ThiemeMedical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662. 0094-6176,p;2001,27,06,585,592,
ftx,en;sth00762x.
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 2/8
The trauma patient’s survival depends on theability to control hemorrhage and support vital organsby preventing MODS after DIC. DIC is a serious he-mostatic problem in critically ill patients and is oftenseen in trauma patients. It is characterized by an activa-tion of the coagulation cascade and, thereby, accelerated
consumption of numerous coagulation factors andplatelets. The consumption and subsequent exhaustionof coagulation proteins and platelets induce severebleeding complications in trauma patients. Suppressionof the physiological anticoagulant pathway and im-paired fibrinolysis as well as activation of coagulationcan be seen in DIC after trauma. The extensive activa-tion of blood coagulation with impaired fibrinolysis re-sults in the generation and deposition of fibrin, leadingto microvascular thrombi in various organs and con-tributing to the development of MODS.1 Recent obser-
vations suggest that, in addition to ischemic organ fail-
ure because of disseminated fibrin deposition, DICcauses inflammatory organ failure through the interac-tion between coagulation and the inflammatory path-
way.2 In trauma patients, DIC has an important role inthe pathogenesis of MODS. Accordingly, DIC strongly influences trauma patients’ morbidity and mortality through serious hemorrhage and organ dysfunction.
To understand the pathophysiology of DIC ininjured patients, we have to know the physiological he-mostasis after trauma. In this article, the physiological
hemostatic responses to trauma are discussed and thenthe coagulofibrinolytic changes in posttrauma DIC arementioned. After the overview of these hemostatic re-sponses to trauma, the mechanisms of organ dysfunc-tion in DIC are shown. Finally, the relationship amongDIC, MODS, and SIRS3 in trauma patients will be
discussed.
PHYSIOLOGICAL HEMOSTATIC
RESPONSES TO TRAUMA
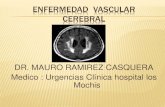
As presented in Figure 1, platelet counts of non-DICpatients were reduced significantly on day 1 as com-pared with those on day 0 and then gradually increasedalmost to the initial values. However, platelet counts of DIC patients showed continuously low levels duringthe study period. The lowest values of prothrombintime and fibrinogen levels were observed on the day of
trauma.The prothrombin time returned to normal, andthe levels of fibrinogen reached the highest values onday 4, as an acute phase-reactant protein. Fibrin/fibrin-ogen degradation product (FDP) levels were minimally elevated during the study period in patients withoutDIC; this was different from what was seen in the DICpatients. Careful observation of the changes in FDPlevels indicates a depression of fibrinolysis and its reac-tivation (see later). Except for platelet counts and FDPlevels, the differences in the levels of global parameters
586 SEMINARS IN THROMBOSIS AND HEMOSTASIS/VOLUME 27, NUMBER 6 2001
Figure 1 Global measurements of coagulation and fibrinolytic activity in trauma patients with (stippled bars) and without (open
bars) DIC. *Denotes p values from 0.05 to 0.0001.
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 3/8
were minor, but one can obviously distinguish DIC pa-tients from non-DIC patients.
The immediate function of the hemostaticmechanisms after trauma is the termination of bleedingfrom the intravascular space by vascular contraction andplatelet plug formation. The next step is the provision of
a fibrin framework at the injured site by activation of thrombin and impairment of fibrinolysis. A furtherfunction is the removal of the fibrin by secondary fibri-nolysis when repair of injured blood vessels or the tissueis sufficiently advanced. Global measurements of coag-ulation and fibrinolysis mentioned earlier hardly detectthese changes. However, using sensitive assay methods,
we can assess thrombin and plasmin activation (fibrino-peptide A [FPA] and fibrinopeptide B
15–42[FPB
15–42]),
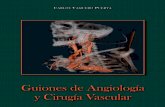
fibrin formation and its degradation (D-dimer), and in-hibition of fibrinolysis by PAI-1.4,5 Figure 2 (left)shows the immediate increase in thrombin activity after
trauma followed by plasmin activity to protect intravas-cular thrombi caused by extra fibrin formation. As a re-sult of the secondary fibrinolysis by plasmin, a steep in-crease in D-dimer levels is noted. To prevent rebleedingby excessive fibrinolysis, PAI-1 increases a few hoursafter the trauma, which brings about a decrease of bothFPB
15–42and D-dimer levels. Several days after trauma,
PAI-1 increase comes to an end, indicating repair of in- jured blood vessels and wound healing.Then we can de-tect removal of unused fibrin by reactivating plasminand reelevation of D-dimer. These scenarios have beenconstructed in several of our studies on hemostaticchanges after trauma.
These hemostatic responses, detected by usingsensitive molecular markers, have long been incorrectly
called hypercoagulability, fibrinolytic shutdown, andits reactivation.6–9 The coagulofibrinolytic changes ob-served in trauma patients without DIC are not a diseaseprocess but a physiological process for hemostasis and
wound healing. The poorly defined term “hypercoagu-lability ” or “fibrinolytic shutdown” should not be used
for the normal physiological hemostatic response totrauma. The use of those terms should be restricted toabnormal hemostatic changes such as DIC.
For the past two decades, the hypothesis thathead injury strongly activates the coagulation cascadeand that the subsequent coagulopathy predicts the out-come of these patients has been widely accepted.10–12
We recently demonstrated that, after systematic eluci-dation of the time course of coagulation and fibrinolysisfollowing isolated head injury, changes in the coag-ulofibrinolytic and antifibrinolytic systems in patients
with head injuries are not different from those in
trauma patients without head injury.4,13
These resultssuggest that the physiological homeostatic response toinjury is similar in all kinds of trauma patients, withoutexceptions.
PATHOLOGICAL HEMOSTATIC
RESPONSES TO TRAUMA
An abnormal pathological hemostatic response totrauma is called DIC. Although identification of nor-mal systemic activation of coagulation and fibrinolysis ispossible using sensitive molecular markers, hemostaticactivity is basically confined to the area of the injury.Occasionally, control mechanisms fail to restrict the he-mostatic processes to the area of tissue damage, and
DIC IN TRAUMA PATIENTS/GANDO 587
Figure 2 Schematic variation of thrombin activity (FPA), plasmin activity (FPB15–42
), fibrin formation and secondary fibrinolysis (D-
dimer), and inhibition of fibrinolysis (PAI-1) after trauma. Patients without DIC (left) and with DIC (right). A vertical axis shows in-
creases from normal values (times). A, FPA; B, FPB15–42; C, D-dimer; D, PAI-1.
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 4/8
they become disseminated throughout the systemic cir-culation, which causes DIC. The DIC diagnosis can beperformed accurately on the basis of the DIC DiagnosisStandard published in 1988 by the Japanese Ministry of Health and Welfare (Table 1). The basic disorder, theclinical condition, and the results of examination forglobal coagulation and fibrinolytic tests are quantifiedon a score basis (maximum = 13; minimum = 0). If thenumber is 7, DIC can be assumed.
Tissue Factor–Mediated Activation
of Coagulation and PAI-1–Mediated
Inhibition of Fibrinolysis
The intrinsic pathway of coagulation does not appear toplay an important role for the activation of coagulationin DIC.14 The consensus is that the function of the con-
tact system is to generate bradykinin, a potent inducer
of local edema and systemic hypotension.1,14 Severallines of evidence point to the pivotal role of the tissuefactor–dependent pathway in the initiation of thrombingeneration. This concept is true for DIC patients aftertrauma. Continuously higher tissue factor levels wereobserved in DIC patients compared with non-DIC pa-
tients on the day of trauma and on days 1 through 4after admission.15 The results suggest extensive activa-tion of the extrinsic coagulation pathway in posttraumaDIC. Massive activation of thrombin and plasmin,measured by FPA and FPB
15–42, respectively, were
noted after tissue factor production.4 The levels of these activation products showed significantly higher
values than those seen for non-DIC patients. As a con-sequence, cross-linked fibrin degradation products,D-dimer also increased to markedly higher levels thanthose seen in non-DIC patients. Both PAI-1 activity and its antigen levels in non-DIC patients decreased to
normal concentrations on day 5 after trauma. On thecontrary, PAI-1 levels in the DIC patients, especially values in nonsurvivors, continued to be markedly higherup to day 5 after trauma.5 The high PAI-1 activity sug-gests that elevated D-dimer levels are not balanced withthe massive fibrin formation observed in DIC patientsafter trauma. The PAI-1–mediated inhibition of fibri-nolysis results in inadequate fibrin removal from the
vasculature.
Suppression of Physiological
Anticoagulant Pathways
An impaired function of the natural regulating path- ways of coagulation activation contributes to fibrin for-mation. Tissue factor pathway inhibitor (TFPI),proteinC, and antithrombin—three major physiological anti-coagulants—are greatly affected in posttrauma DIC.Recently, we systematically elucidated the relationshipbetween tissue factor and TFPI in posttrauma patients.
We found that an activated tissue factor–dependentpathway is not sufficiently prevented by the normal
TFPI levels in patients with DIC.15
The serial changes of the protein C system aftertrauma were further investigated.16 When trauma pa-tients were complicated with DIC, the protein C activ-ity and the antigen levels showed significantly lower
values than those for the non-DIC patients. When clas-sified into subgroups of survivors and nonsurvivors, theprotein C activity and antigen levels decreased signifi-cantly in the nonsurvivors compared with those in thesurvivors. Antithrombin, the last endogenous physio-logical anticoagulant, was also significantly reduced inposttrauma patients.17 The reduction of the protein Csystem and antithrombin may be caused by consump-tion, degradation, impaired synthesis, and downregula-tion of thrombomodulin.1 Markedly elevated levels of
soluble thrombomodulin and elastase released from ac-
588 SEMINARS IN THROMBOSIS AND HEMOSTASIS/VOLUME 27, NUMBER 6 2001
Table 1 Criteria for the Diagnosis of DIC by theJapanese Ministry of Health and Welfare
Score
Etiology of DIC
Yes 1
No 0
Clinical symptoms
Bleeding symptom
Yes 1
No 0
Organ dysfunction
Yes 1
No 0
Laboratory tests
FDP (g/mL)
40 3
20, < 40 2
10, < 20 1
< 10 0
Platelet Counts (104 /mL)
5 3
8, > 5 2
12, >8 1
> 12 0
Fibrinogen (mg/dL)
100 2
150, > 100 1
> 150 0
Prothrombin time (value of patient/normal value)
1.67 2
1.25, < 1.67 1< 1.25 0
Diagnosis
7 points DIC
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 5/8
tivated neutrophils until the fifth day of trauma in DICpatients partly confirms the hypothesis.18
These studies clearly demonstrate tissue factor–mediated activation of coagulation, depression of anti-coagulant system, and impaired fibrinolysis in DICpatients after trauma. Based on these results, we can
construct Figure 2 (right), reflecting the pathologicalhemostatic response to trauma. This can be obviously distinguished from the physiological hemostaticchanges also presented in Figure 2 (left).
CLOSE RELATIONSHIP BETWEEN
DIC AND MODS
In the 1990s, our understanding of the underlyingmechanisms in organ dysfunction after trauma in-creased dramatically.3,19–21 Multiple alterations in thehemostatic, inflammatory, and immunologic functions
have been demonstrated in clinical and experimentalsituations after trauma. In particular, it is now apparentthat acute respiratory distress syndrome (ARDS) andMODS have their genesis in the development of DICfollowing trauma.22
DIC patients showing higher thrombin activity exhibited by FPA have had poor outcomes.4 Inhibitionof fibrinolysis using the differences of tissue plasmino-gen activator activity and its antigen levels in DIC pa-tients has been indirectly implied.4 Gando et al5 de-scribed 58 trauma patients, 22 with DIC. The DICpatients had a higher mortality rate, 59% versus 14%.
Tumor necrosis factor- (TNF-), interleukin-1(IL-1), and PAI-1 increases were most consistently as-sociated with fatal outcome, whereas DIC was a predic-tor of ARDS and MODS.5 Neutrophil elastase releasedfrom activated neutrophils causes damage to vascularendothelial cells, and this endothelial cell injury wasdemonstrated to be deeply involved with ARDS andMODS in patients with DIC after trauma.18 The acti- vation of the tissue factor–dependent coagulation path- way and impaired fibrinolysis, as well as neutrophil acti- vation, plays an important role in the pathogenesis of posttraumatic ARDS.23,24 The ARDS patients had ahigher incidence of DIC (74 to 100%) and showedpoorer outcomes.23,24 These studies clearly suggest thata frequent complication of DIC in trauma gives rise tothe development of ARDS and MODS.
PATHOLOGICAL MECHANISMS OF DIC
IN THE DEVELOPMENT OF MODS
Extensive thrombin generation, serious defects in coag-ulation inhibitors, and impaired fibrinolysis, observed inDIC, result in ongoing massive fibrin deposition in the
vasculature. Several lines of evidence indicate that hy-poxic occlusive thrombosis caused by disseminated fi-
brin formation gives rise to MODS and mortality in
DIC patients.1 It is not certain, however, to what extentintravascular fibrin deposition alone contributes toMODS and mortality. Taylor et al25 demonstrated thateffective inhibition of the hemostatic response by DIC
with active site–inhibited factor Xa did not protect theanimals from organ failure and death. The results sug-
gest that fibrin formation per se does not influence theoutcome in DIC animals.
Recent experimental evidence has suggestedthat, in addition to their role in hemostasis, proteases of the clotting and fibrinolytic cascades transduce intracel-lular signals and modulate immunoinflammatory re-sponses through both protease and protease-activatedreceptors.2 Cross-talk between coagulation and inflam-mation amplifies mutual cascades, contributing to thepathogenesis of tissue injury and organ dysfunction.26,27
In particular, the thrombin/protease activated receptor-1(PAR-1) system plays an important role in inflamma-
tory endothelial damage by inducing proinflammatory cytokines and adhesion molecule expression after acti- vation of neutrophils and endothelium.2 These studiessuggest that amplification and perpetuation of inflam-matory response through interactions between inflam-matory and coagulation pathways, as well as to theocclusive microvascular thrombosis and hypoxia, arecritical to the development of MODS in DIC patientsafter trauma.
CLINICAL EVIDENCE OF THE CROSS-TALK
BETWEEN DIC AND INFLAMMATION
The derangement of coagulation and fibrinolysis inDIC is mediated by several proinflammatory cytokinesand neutrophil activation associated with endothelialinjury, which is greatly involved in the development of MODS in posttrauma DIC patients.5,18 A report by Nast-Kolb et al28 reinforces these results. They demon-strated low antithrombin levels, elevated neutrophilelastase, and proinflammatory cytokines (IL-6 andIL-8) in trauma patients who died from MODS. Thedata show that the degree of coagulation and inflamma-tory responses corresponds with posttraumatic MODS.
That DIC and inflammation synergistically contributeto the development of MODS and poor outcome intrauma patients was confirmed by two other investiga-tions.29,30 The inflammatory response has been found tobe amplified and perpetuated through a thrombin/receptor interaction in a positive feedback manner.
There is a possibility that activation of the coagulationpathway can participate in sustaining and amplifying aninflammatory response in addition to producing hy-poxia through the production of microvascular throm-bosis by fibrin. Thus, sustained SIRS originating fromDIC is the main determinant for ARDS, MODS, andpoor outcome in patients with DIC after trauma.29
After this study, the accuracy of DIC and sustained
DIC IN TRAUMA PATIENTS/GANDO 589
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 6/8
590 SEMINARS IN THROMBOSIS AND HEMOSTASIS/VOLUME 27, NUMBER 6 2001
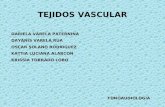
Figure 3 Schematic representation of mechanisms in the pathogenesis of MODS after trauma.
Figure 4 Relationship among DIC, sustained SIRS, and MODS after trauma. 1st insult, trauma; 2nd insult, DIC; 3rd insult, sepsis.
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 7/8
SIRS in predicting MODS after trauma was deter-mined by application of clinical decision analysis. Like-lihood ratios of DIC and SIRS for >3 days for predict-ing posttrauma MODS were 11.6 and 6.25,respectively.30 Platelet counts could be used as a simplelaboratory test for predicting MODS. These studies
clearly demonstrate the important link among, DIC,SIRS, and MODS after trauma. Figure 3 shows theschematic representation of mechanisms in the patho-genesis of MODS after trauma.
CONCLUSION
Figure 4 shows our scenario on the relationship amongDIC, sustained SIRS, and MODS after trauma.
Trauma is the first insult, followed by initial SIRS. Se- vere insult per se causes primary MODS and death.Mild to moderate SIRS comes to an end within a few
days after trauma, which is thought to be a physiologicalresponse to the insult, but severe SIRS persists for>3 days after the onset of trauma. The DIC associated
with massive thrombin generation, excessive systemicmediator release (e.g., proinflammatory cytokines andneutrophil elastase), and endothelial injury alters theSIRS reaction. Finally, the persistent alterations ulti-mately lead to sustained SIRS, producing secondary MODS and death. Sometimes a complicating sepsisabout a week later acts as a third insult and modifiessustained SIRS after trauma.
REFERENCES
1. Levi M,de Jonge E, van der Poll T, ten Cate H. Disseminatedintravascular coagulation.Thromb Haemost 1999;82:695–705
2. Cicala C, Cirino G. Linkage between inflammation and co-agulation: An update on the molecular basis of the crosstalk.Life Sci 1998;62:1817–1824
3. Members of American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Commit-tee. American College of Chest Physicians/Society of CriticalCare Medicine Consensus Conference: Definitions for sepsisand organ failure and guidelines for the use of innovativetherapies in sepsis.Crit Care Med 1992;20:864–874
4. Gando S, Tedo I, Kubota M. Posttrauma coagulation and fi-
brinolysis. Crit Care Med 1992;20:594–6005. Gando S, Nakanishi Y, Tedo I. Cytokines and plasminogen
activator inhibitor-1 in posttrauma disseminated intravascu-lar coagulation: Relationship to multiple organ dysfunctionsyndrome. Crit Care Med 1995;23:1835–1842
6. Seyfer AE, Seaber AV, Dombrose FA, Urbaniak JR. Coagula-tion changes in elective surgery and trauma. Ann Surg 1981;193:210–213
7. Kluft C, Verheijen JH, Jie AFH, et al. The postoperative fi-brinolytic shutdown: A rapidly reverting acute phase patternfor the fast-acting inhibitor of tissue-type plasminogen acti-
vator after trauma. Scand J Clin Lab Invest 1985;45:605–6108. Kapsch DN,Metzler M, Harrington M, et al. Fibrinolytic re-
sponse to trauma. Surgery 1984;95:473–478
9. Risberg B, Medegård A, Heideman M, et al. Early activationof humoral proteolytic systems in patients with multipletrauma.Crit Care Med 1986;14:917–925
10. Goodnight SH, Kenoyer G, Rapaport SI, et al. Defibrinationafter brain-tissue destruction. A serious complication of headinjury. N Engl J Med 1974;290:1043–1047
11. Disseminated intravascular coagulation and head injury.
Lancet 1982;2:531.Editorial12. Abnormal blood clotting after head injury. Lancet 1989;2:
957–958.Review 13. Gando S, Nanzaki S, Kemmotsu O. Coagulofibrinolytic
changes after isolated head injury are not different from thosein trauma patients without head injury. J Trauma 1999;46:1070–1077
14. Levi M, ten Cate H, van der Poll T, van Deventer SJH.Pathogenesis of disseminated intravascular coagulation insepsis. JAMA 1993;270:975–979
15. Gando S, Nanzaki S, Morimoto Y, et al. Tissue factor path- way inhibitor response does not correlate with tissue-factorinduced DIC and MODS in trauma patients. Crit Care Med2001;24:262–266
16. Gando S. Serial studies of protein C in trauma patients. Jpn J Thromb Hemost 1996;7:312–318 [In Japanese]
17. Owings JT, Gosselin R. Acquired antithrombin deficiency following severe traumatic injury: Rationale for study of anti-thrombin supplementation. Semin Thromb Hemost 1997;23(Suppl 1):17–24
18. Gando S, Nakanishi Y, Kameue T, Nanzaki S.Soluble throm-bomodulin increases in patients with disseminated intravas-cular coagulation and in those with multiple organ dysfunc-tion syndrome after trauma: Role of neutrophil elastase. J
Trauma 1995;39:660–66419. Donnelly SC, Robertson CR. Mediators, mechanisms and
mortality in major trauma. Resuscitation 1994;28:87–9220. Moor FA, Sauaia A, Moor EE, et al. Postinjury multiple
organ failure: A bimodal phenomenon. J Trauma 1996;40:501–512
21. Yao YM, Redl H, Bahrami S, Schlag G. The inflammatory basis of trauma/shock-associated multiple organ failure. In-flamm Res 1998;47:201–210
22. Penner JA. Disseminated intravascular coagulation in patients with multiple organ failure of non-septic origin. Semin Thromb Hemost 1998;24:45–52
23. Gando S, Kameue T, Nanzaki S, et al. Increased neutrophilelastase, persistent intravascular coagulation, and decreasedfibrinolytic activity in patients with posttraumatic acute respi-ratory distress syndrome. J Trauma 1997;42:1068–1072
24. Gando S, Nanzaki S, Morimoto Y, et al. Systemic activationof tissue-factor dependent coagulation pathway in evolving
acute respiratory distress syndrome in patients with traumaand sepsis. J Trauma 1999;47:719–723
25. Taylor FB, Chang ACK, Peer GT, et al. DEGR-Factor Xablocks disseminated intravascular coagulation initiated by Escherichia coli without preventing shock or organ damage.Blood 1991;78:364–368
26. Taylor FB, Stearns-Kurosawa J,Ferrell G, et al.The endothe-lial cell protein C receptor aids in host defense against Echerichia coli sepsis. Blood 2000;95:1680–1686
27. Cirino G, Cicala C, Bucci M, et al. Factor Xa as an interfacebetween coagulation and inflammation. J Clin Invest 1997;99:2446–2451
28. Nast-Kolb D, Waydhas C, Gippner-Steppert C, et al. Indica-tor of the posttraumatic inflammatory response correlate with
DIC IN TRAUMA PATIENTS/GANDO 591
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l

7/23/2019 Coagulopatía Vascular Disemjhkhjhinada
http://slidepdf.com/reader/full/coagulopatia-vascular-disemjhkhjhinada 8/8
organ failure in patients with multiple injuries. J Trauma1997;42:446–455
29. Gando S, Kameue T, Nanzaki S, et al. Participation of tissuefactor and thrombin in posttraumatic systemic inflammatory syndrome. Crit Care Med 1997;25:1820–1826
30. Gando S, Nanzaki S,Kemmotsu O. Disseminated intravascu-lar coagulation and sustained systemic inflammatory responsesyndrome predict organ dysfunctions after trauma. Appli-cation of clinical decision analysis. Ann Surg 1999;229:121–127
592 SEMINARS IN THROMBOSIS AND HEMOSTASIS/VOLUME 27, NUMBER 6 2001
D o w n l o a d e d b y : C o l l e c t i o n s a n d T e c h n i c a l S e r v i c e s D e p a r t m e n t C o p y r i g h
t e d m a t e r i a l