El caso de la patología vesicular
23
l IV Congreso chileno de Salud Pública y VI Congreso chileno de Epidemiología “Haciendo visibles los problemas de salud de siglo XXI” El Caso de la Patología Vesicular Catterina Ferreccio Escuela de Medicina Dpto. Salud Pública Coquimbo, 1 de Diciembre 2017
-
Upload
salud-en-todas -
Category
Healthcare
-
view
32 -
download
1
Transcript of El caso de la patología vesicular

l IV Congreso chileno de Salud Pública y VI Congreso chileno de Epidemiología
“Haciendo visibles los problemas de salud de siglo XXI”
El Caso de la Patología Vesicular Catterina Ferreccio
Escuela de Medicina Dpto. Salud PúblicaCoquimbo, 1 de Diciembre 2017
Objetivos • Analizar los factores de riesgo del cancer de
vesícula biliar• Discutir posibles externalidades negativas de la
colecistectomía• Agenda de investigación en la materia

1960 1970 1980 1984 1990 2000 2005 2010 0
5
10
15
20
25
30
35 MORTALITY SELECTED DIGESTIVE CANCERS CHILE 1960-2010
STOMACHGALLBLADDERLIVER
RATE
S PE
R 10
0,00
0
Public Health System crisis
Public Health System recovery

EXCESS BODY FATNESS AND CANCER
IARC 2016>1,000 studies, > 20 cancer sites or typesVarious Epi study designs, Experimental animals In vitro studies.
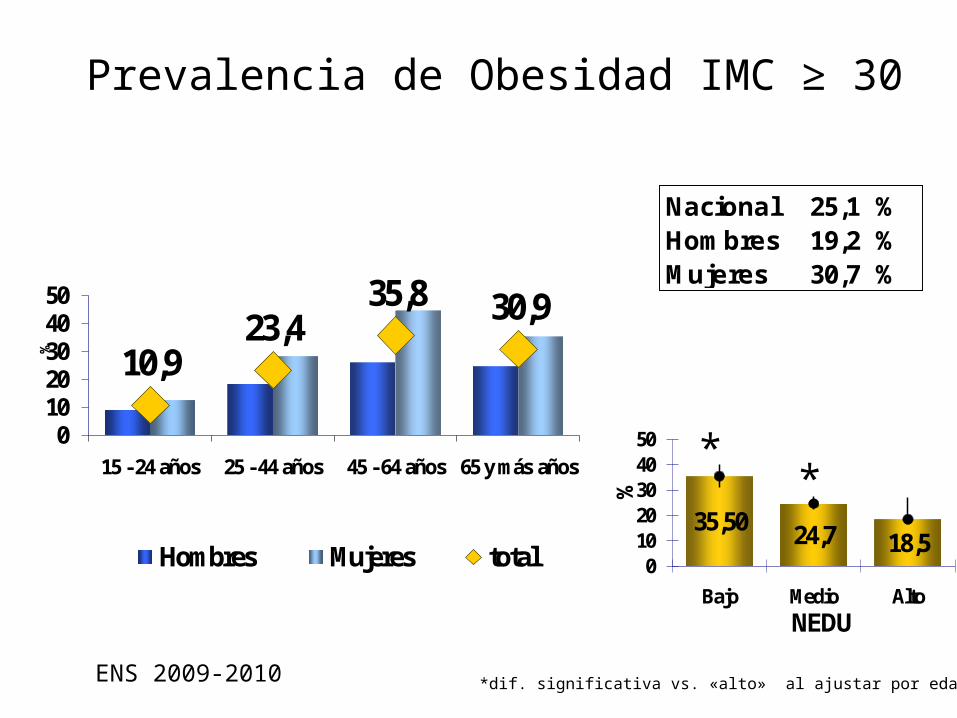
Prevalencia de Obesidad IMC ≥ 30
10,923,4
35,8 30,9
01020304050
15 - 24 años 25 - 44 años 45 - 64 años 65 y más años
%
Hombres Mujeres total
Nacional 25,1 %Hombres 19,2 %Mujeres 30,7 %
35,50 24,7 18,50
1020304050
Bajo Medio Alto%
NEDU
**
*dif. significativa vs. «alto» al ajustar por edad y sexoENS 2009-2010
MAUCO: MEDICION BASAL 2014-2015
• Población de Molina (Adultos 38-74 años)- 30.1% rural- Alta mortalidad CV y cáncer
de estómago y vesicula biliar
• Participantes a abril 2016. • N = 4.000
- Ferreccio et al. Study protocol for the Maule Cohort (MAUCO) of chronic diseases, Chile 2014–2024. BMC Public Health 2016
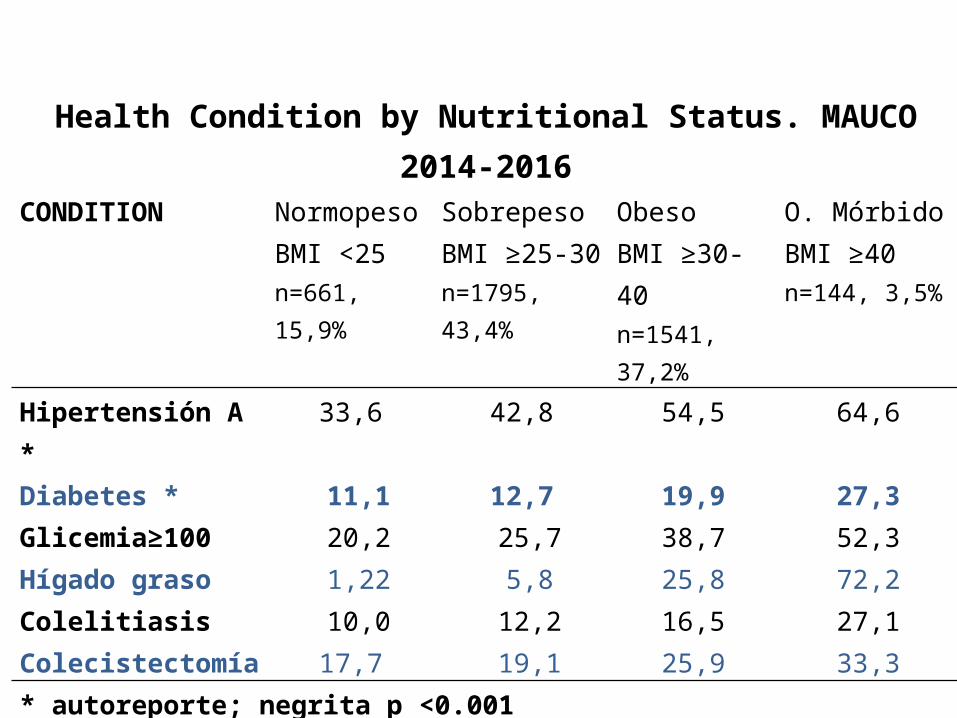
Health Condition by Nutritional Status. MAUCO 2014-2016CONDITION Normopeso
BMI <25n=661, 15,9%
SobrepesoBMI ≥25-30n=1795, 43,4%
ObesoBMI ≥30-40n=1541, 37,2%
O. MórbidoBMI ≥40n=144, 3,5%
Hipertensión A * 33,6 42,8 54,5 64,6Diabetes * 11,1 12,7 19,9 27,3Glicemia≥100 20,2 25,7 38,7 52,3Hígado graso 1,22 5,8 25,8 72,2Colelitiasis 10,0 12,2 16,5 27,1Colecistectomía 17,7 19,1 25,9 33,3* autoreporte; negrita p <0.001
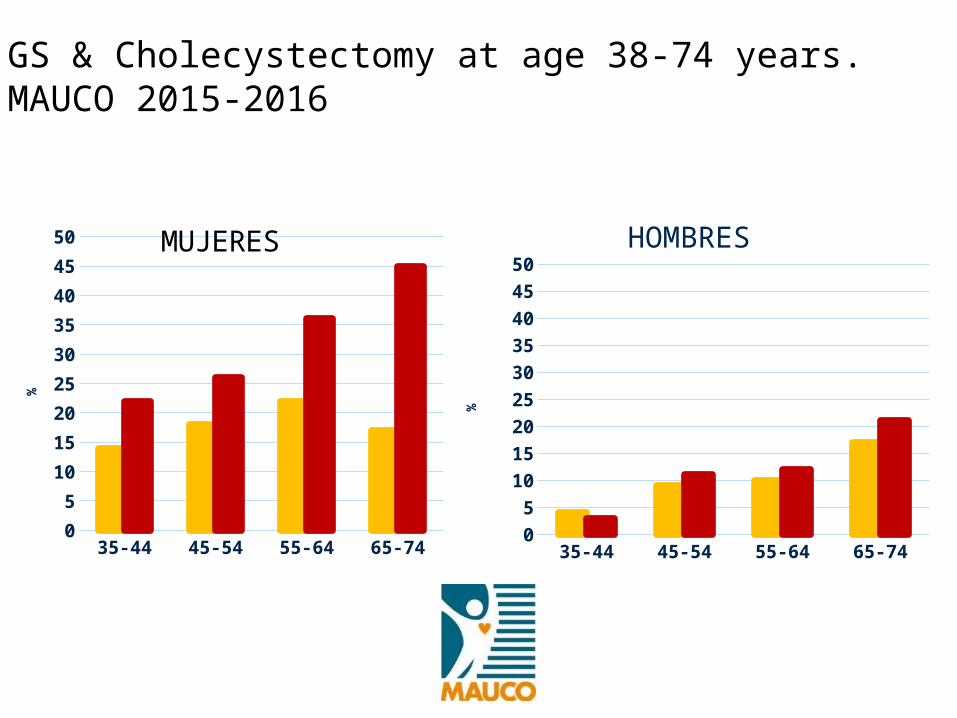
GS & Cholecystectomy at age 38-74 years. MAUCO 2015-2016
35-44 45-54 55-64 65-7405
101520253035404550
colelitiasis colecistectomia
%
MUJERES
35-44 45-54 55-64 65-7405
101520253035404550
colelitiasis colecistectomia
%
HOMBRES

RISK FACTORS
CONTAMINANTES QUIMICOS??

Chile BiLSChile Biliary Longitudinal Study
Maule Cohort sub-study:Natural History of Gallbladder Cancer
Litiasis y cancer de la vesicular biliar

Chronic Salmonella typhi infection
Nature Reviews Microbiology; Jan2011, Vol. 9 Issue 1, p9-14, 6p, 3 Diagrams

ST and GBC facts
• 3% of infected with S. typhi (ST) become chronic carriers.
• GS cases: 6 -15 higher risk of becoming chronic carrier.
• Chronic carriers: 3 a 200 higher Risk of GBC ;1-6% lifetime risk


GBC (51)
GS(49)
Control POP(52)
WOMEN% 78,4 81,6 81,1MEAN AGE 62 61 64MAPUCHE % 15,7 14,3 9,4SCHOOL YEARS 7,4 7,6 8,5S typhi high Vi abP <0.03
15.4 % 5.2 % 2.6%
CASE-CONTROL STUDY OF GBC Chile 2011-2014
Meta-analysis > 1,000 cases: Summary relative risk = 4.6 (95% CI: 3.1–6.8) for anti-Vi; 5.0 (95% CI: 2.7–9.3) for bile or stool culture. Pheterogeneity=0.6 and = 0.2.
Koshiol 2016

Del libro de Sonia Montecino sobre la cocina criolla
Previous study found GBC risk associated to red pepper consumptionAflatoxin was found in samples of DRIED Chile pepper

GBC Gallstone Control P‡Factor (n=36) (n=29) (n=47)
AFB1 adduct detection, (%)*
63.9 27.6 21.3 <0.001
Red Chili Pepper paste, ≥ 1/week (%)
47.2 17.9 19.1 0.007
Fresh Green chili pepper , ≥ 1/week (%)
55.6 42.9 38.3 0.3
Aflatoxina B1-lysine adducts among Gallbladder cancers
(GBC) and controls

ORGBC vs. PBC: 13.2, 95% CI: 4.3-47.9*
ORGBC vs. GS: 5.8, 95% CI: 2.0-18.4*
*Adjusted for age, gender, and residence area
GBC cases vs stones and population controls % aflatoxin B1-albumin adducts levels above
detection level
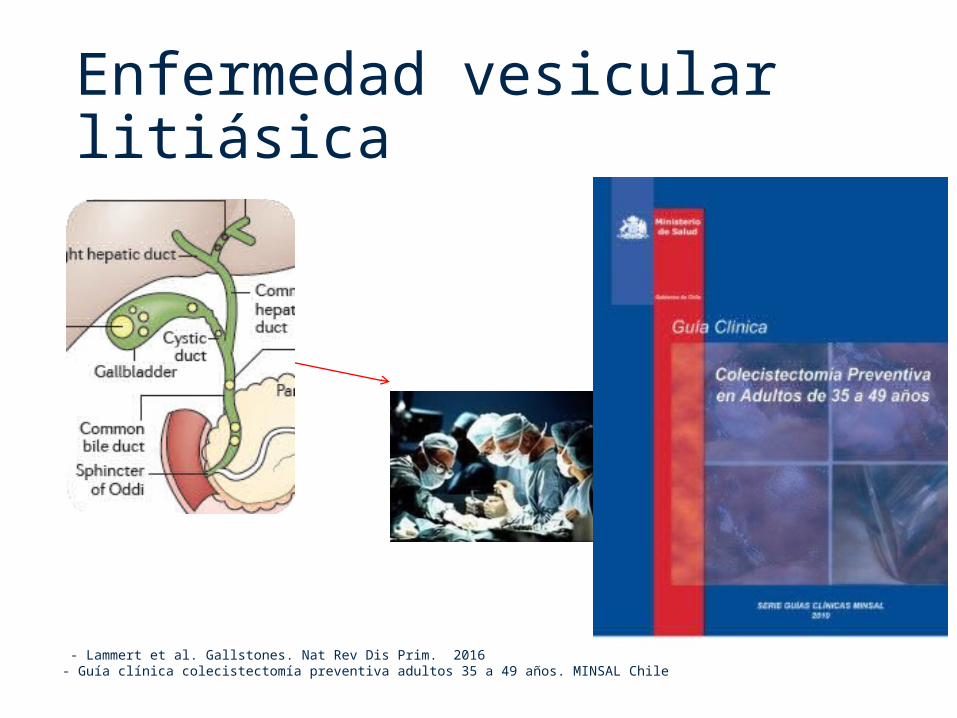
Enfermedad vesicular litiásica
- Lammert et al. Gallstones. Nat Rev Dis Prim. 2016- Guía clínica colecistectomía preventiva adultos 35 a 49 años. MINSAL Chile
Long term risks of Cholecystectomy
• NAFLD: Higado Graso no alcoholico• Metabolic syndrome• Liver cancer, Cáncer Hepático
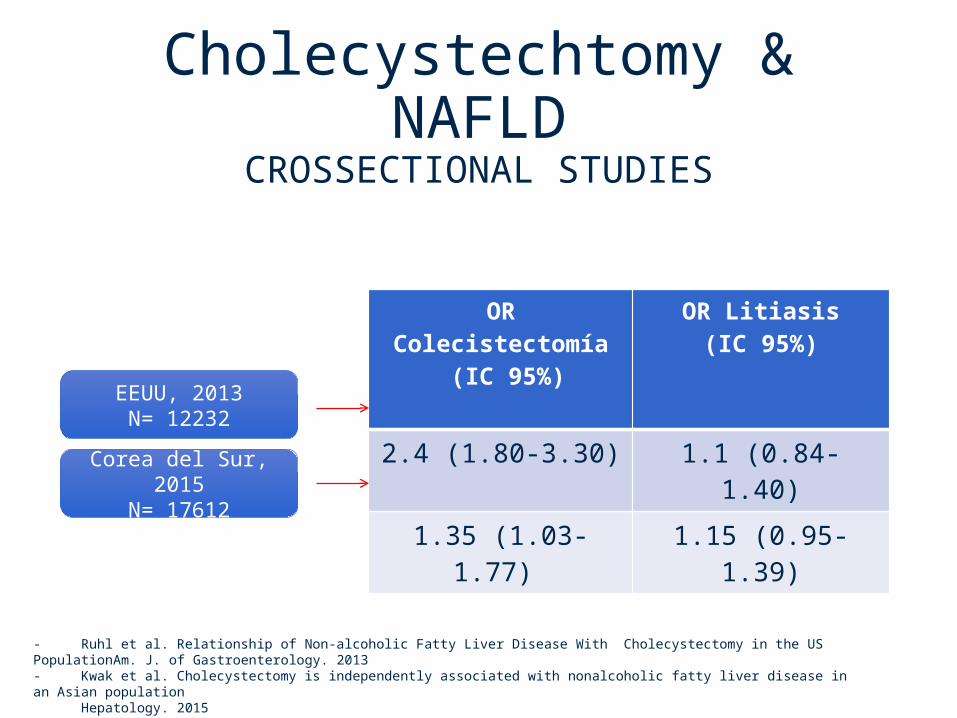
Cholecystechtomy & NAFLD
CROSSECTIONAL STUDIES
OR Colecistectomía (IC 95%)
OR Litiasis(IC 95%)
2.4 (1.80-3.30) 1.1 (0.84-1.40)
1.35 (1.03-1.77) 1.15 (0.95-1.39)
- Ruhl et al. Relationship of Non-alcoholic Fatty Liver Disease With Cholecystectomy in the US PopulationAm. J. of Gastroenterology. 2013 - Kwak et al. Cholecystectomy is independently associated with nonalcoholic fatty liver disease in an Asian population Hepatology. 2015
EEUU, 2013N= 12232
Corea del Sur, 2015N= 17612
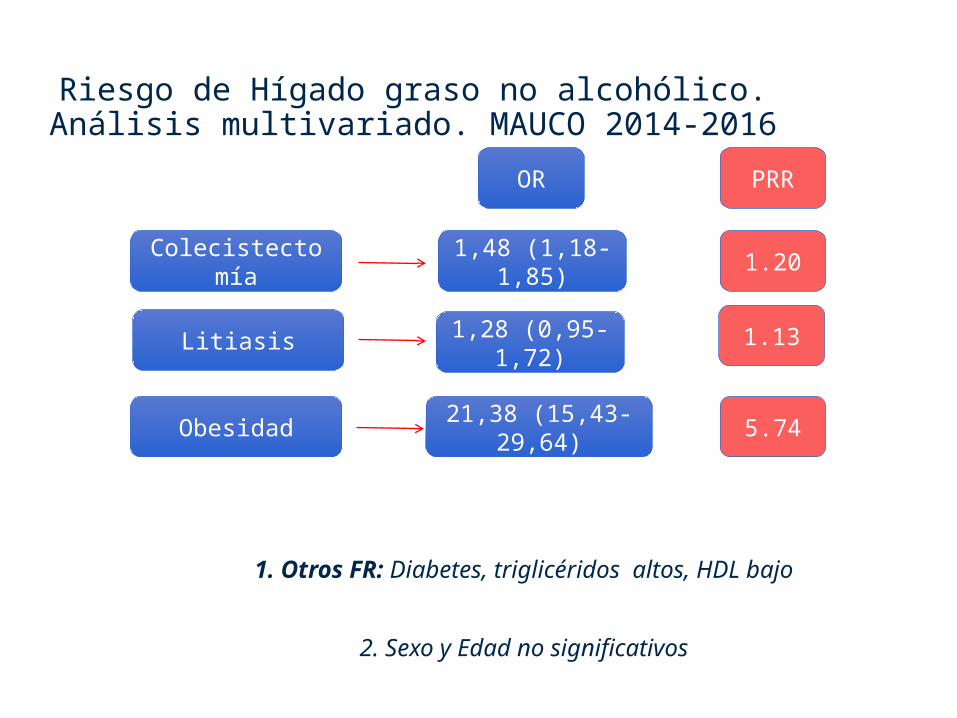
Riesgo de Hígado graso no alcohólico. Análisis multivariado. MAUCO 2014-2016
1. Otros FR: Diabetes, triglicéridos altos, HDL bajo
2. Sexo y Edad no significativos
Colecistectomía
Litiasis
Obesidad
OR PRR
1,48 (1,18-1,85)
1,28 (0,95-1,72)
21,38 (15,43-29,64)
1.20
1.13
5.74
FONDAP ADVANCED CENTER FOR CHRONIC DISEASES ACCDiS
MUCHAS GRACIAS
DISCUSION1. NECESIDAD DE INVESTIGAR EL EFECTO A LARGO PLAZO DE LA COLECISTECTOMIA2. BUSCAR ALTERNATIVAS DE SCREENING PARA SELECCIONAR Y PRIORIZAR ESTA INTERVENCIÓN