
Ernesto Báscolo - PHC governance and performance in Latin America: methods, results and lessons...
32
PHC governance and performance in Latin America: methods, results and lessons learned from a research experience funded by IDRC Ernesto Báscolo y Natalia Yavich CENTRO DE ESTUDIOS INTERDISCIPLINARIOS
-
Upload
isags-unasur -
Category
Education
-
view
261 -
download
0
Transcript of Ernesto Báscolo - PHC governance and performance in Latin America: methods, results and lessons...

PHC governance and performance in Latin America: methods, results and lessons learned
from a research experience funded by IDRC
Ernesto Báscolo y Natalia Yavich
CENTRO DE ESTUDIOSINTERDISCIPLINARIOS
EstructuraA) una síntesis del proyecto: objetivos y conclusiones.B) ¿en qué medida y de qué forma el proyecto promovió el análisis, diseño y/o
implementación de una respuesta intersectorial a los determinantes sociales y ambientales de la salud?
C) un análisis de las características más relevantes del proceso de gobernanza de la experiencia presentada, teniendo en cuenta las dimensiones analíticas e interrogantes antes reseñadas;
D) En relación con lo anterior, una reseña sobre cómo el proyecto armonizó o podría vincular la gobernanza del nivel local con los niveles estatales-provinciales y con el nacional (y sus implicancias para la replicación e influencia en políticas públicas)
E) ¿cuál fue la estrategia del proyecto para difundir la investigación a tomadores de decisión y actores sociales, con el propósito de facilitar el uso de los resultados? ¿Cómo y cuándo se involucraron los actores no académicos?
Una síntesis del proyecto: objetivos y conclusiones.
• Desarrollo y aplicación del Marco Analítico de Gobernanza a los procesos de implementación de políticas de extensión de la protección social en salud en América Latina. Project Nro. 103998-001.
• IDRC officers: Roberto Bazzani (Uruguay); David Zakus (Ottawa); Marie-Gloriose Ingabire (Ottawa).
• Responsible Institution: Instituto de la Salud Juan Lazarte, Rosario, Argentina
• Collaborator institution: Instituto para el Desarrollo Humano, Cochabamba, Bolivia
• Period: May 2007 to May 2011.
• Support: IDRC; Instituto de la Salud Juan Lazarte, Municipalities, Agencia Nacional de Ciencia y Técnica.
Project overview
• RationaleWeaknessess of policies implementation in Latin American health
systems due to issues of governability, fragmentation, descentralization → Governance analysis give as clues for intervention and enhance the comprehension of the policy results.
Project overview. Purpose, objetive and methodological approach
• General purposeContribute to enhancement of social protection in health policies implementation
and development.
• General Objetives– Enhance the comprehension of the factors and procesess that
affects the effectiveness of the policies based on PHC strategies inLatin America (and how these aspects affect the effectiveness).
– Develop a governance analytical framework to study thoseprocesess.
• Methodological approachPAR as the umbrella methodological apprach.Design: Multiple-case study → Argentina 3 municipalities (2 Provinces)
Bolivia 2 municipalities (1 Department)
Case studies phases• Contextualization: political, socio-economic,
health status, health system structure and policies.
• Health care services characterization (focus on primary care level)
• Evaluation of primary health care services performance from the point of view of the most vulnerable population.
• Governance analysis of the PHC policies.
Methods and activities
2007-2009: started the pilot case: Rosario (Santa Fé Province).Design of tools and theorical exploration.
Secondary data collectionPrimary data collection
Analysis
2008-2010: started with other 4 cases: 2 in Argentina and 2 in Bolivia.
Tools review and adaptation for Bolivia and Buenos Aires.
Secondary data collectionPrimary data collection
Analysis
2010-2011: Health system perspective reseachTools design
Primary data collectionSecondary (health accounts) data collection
Analysis
Results presentation to policy makers and technical teams - Meeting with managers - Workshop with practitioners –
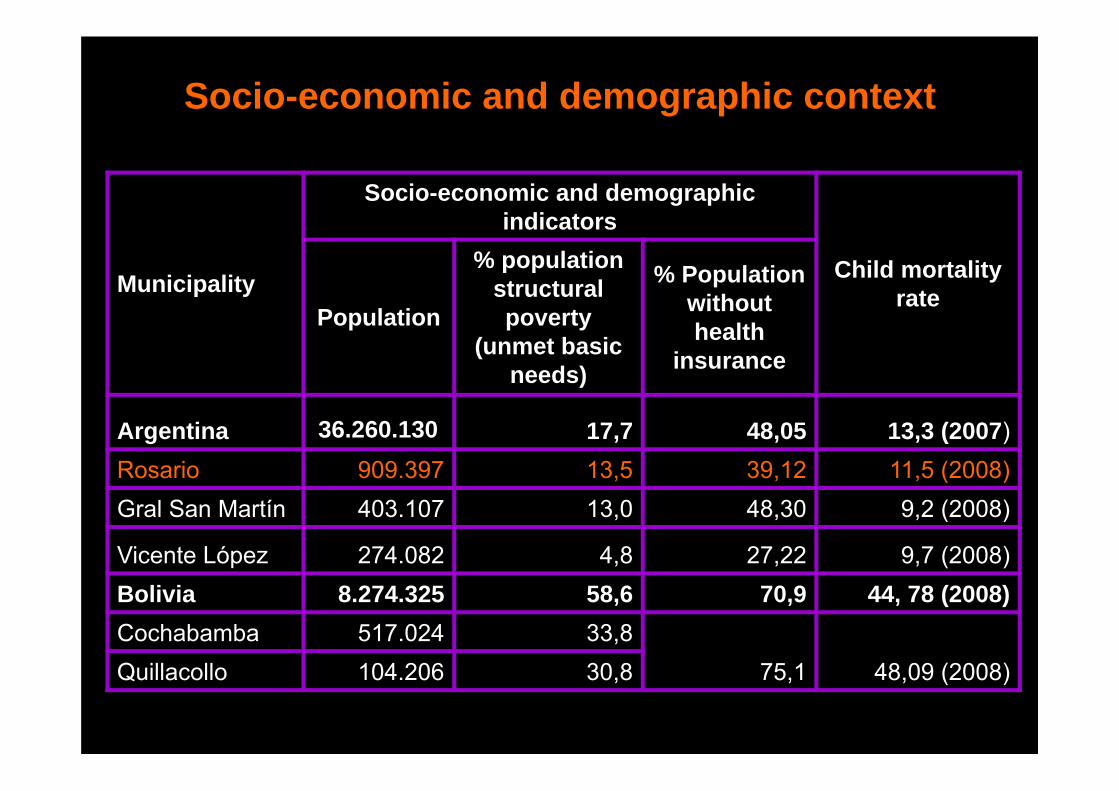
Socio-economic and demographic context
Municipality
Socio-economic and demographic indicators
Child mortality rate
Population
% population structural poverty
(unmet basic needs)
% Population without health
insurance
Argentina 36.260.130 17,7 48,05 13,3 (2007)Rosario 909.397 13,5 39,12 11,5 (2008)Gral San Martín 403.107 13,0 48,30 9,2 (2008)
Vicente López 274.082 4,8 27,22 9,7 (2008)Bolivia 8.274.325 58,6 70,9 44, 78 (2008)Cochabamba 517.024 33,8
75,1 48,09 (2008)Quillacollo 104.206 30,8
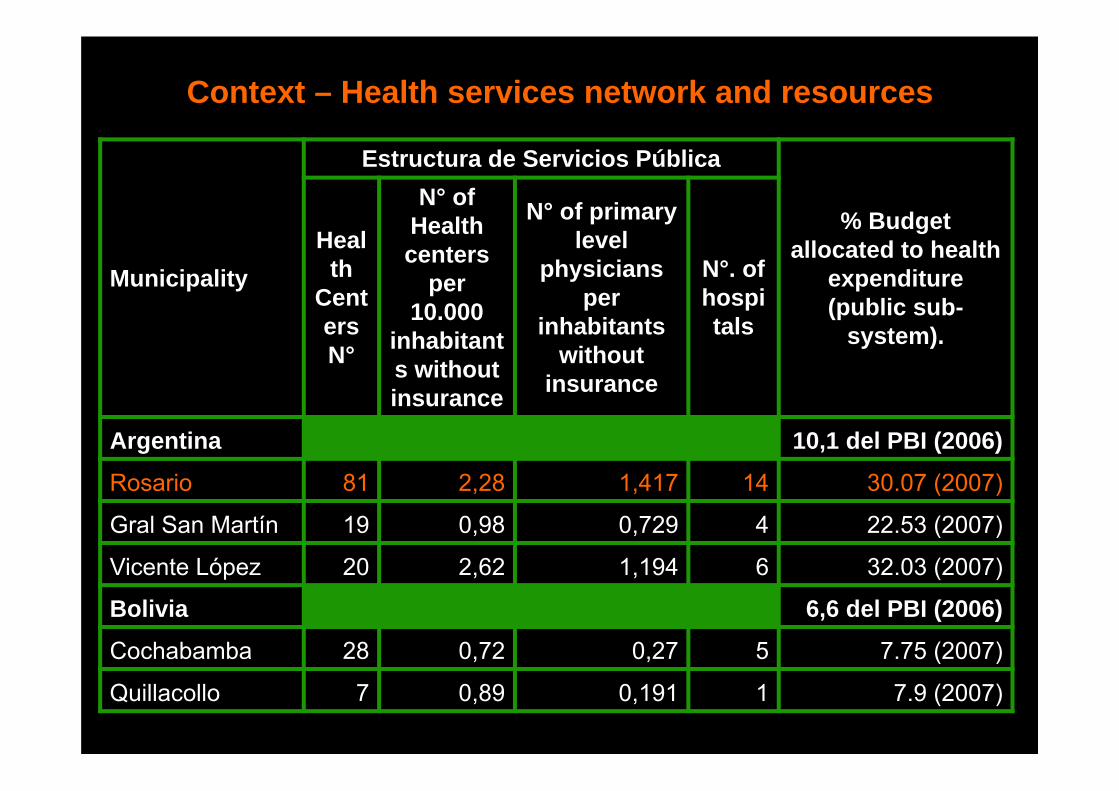
Context – Health services network and resources
Municipality
Estructura de Servicios Pública
% Budget allocated to health
expenditure (public sub-
system).
Health
CentersN°
N° of Health centers
per 10.000
inhabitants without insurance
N° of primary level
physicians per
inhabitants without
insurance
N°. of hospitals
Argentina 10,1 del PBI (2006)
Rosario 81 2,28 1,417 14 30.07 (2007)
Gral San Martín 19 0,98 0,729 4 22.53 (2007)
Vicente López 20 2,62 1,194 6 32.03 (2007)
Bolivia 6,6 del PBI (2006)
Cochabamba 28 0,72 0,27 5 7.75 (2007)
Quillacollo 7 0,89 0,191 1 7.9 (2007)
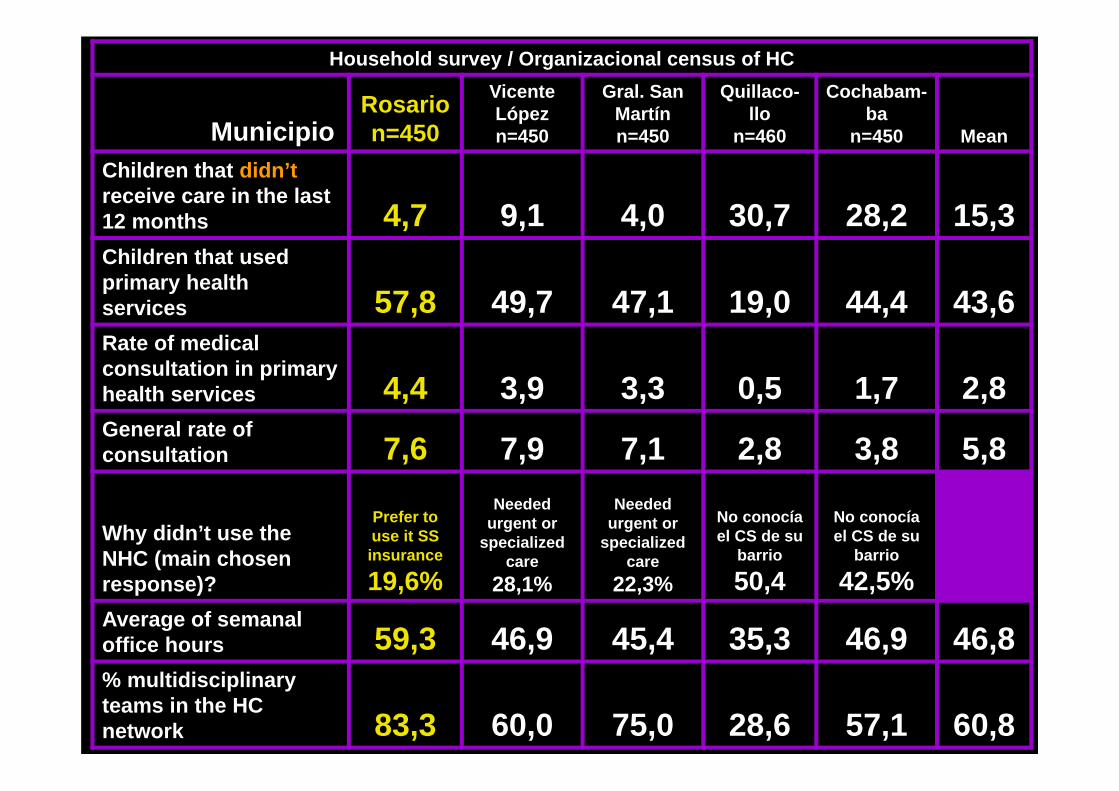
Household survey / Organizacional census of HC
MunicipioRosario n=450
Vicente López n=450
Gral. San Martín n=450
Quillaco-llo
n=460
Cochabam-ba
n=450 Mean
Children that didn’t receive care in the last 12 months 4,7 9,1 4,0 30,7 28,2 15,3Children that used primary health services 57,8 49,7 47,1 19,0 44,4 43,6Rate of medical consultation in primary health services 4,4 3,9 3,3 0,5 1,7 2,8General rate of consultation 7,6 7,9 7,1 2,8 3,8 5,8
Why didn’t use the NHC (main chosen response)?
Prefer to use it SS insurance
19,6%
Needed urgent or
specialized care
28,1%
Needed urgent or
specialized care
22,3%
No conocía el CS de su
barrio
50,4
No conocía el CS de su
barrio
42,5%Average of semanal office hours 59,3 46,9 45,4 35,3 46,9 46,8% multidisciplinary teams in the HC network 83,3 60,0 75,0 28,6 57,1 60,8
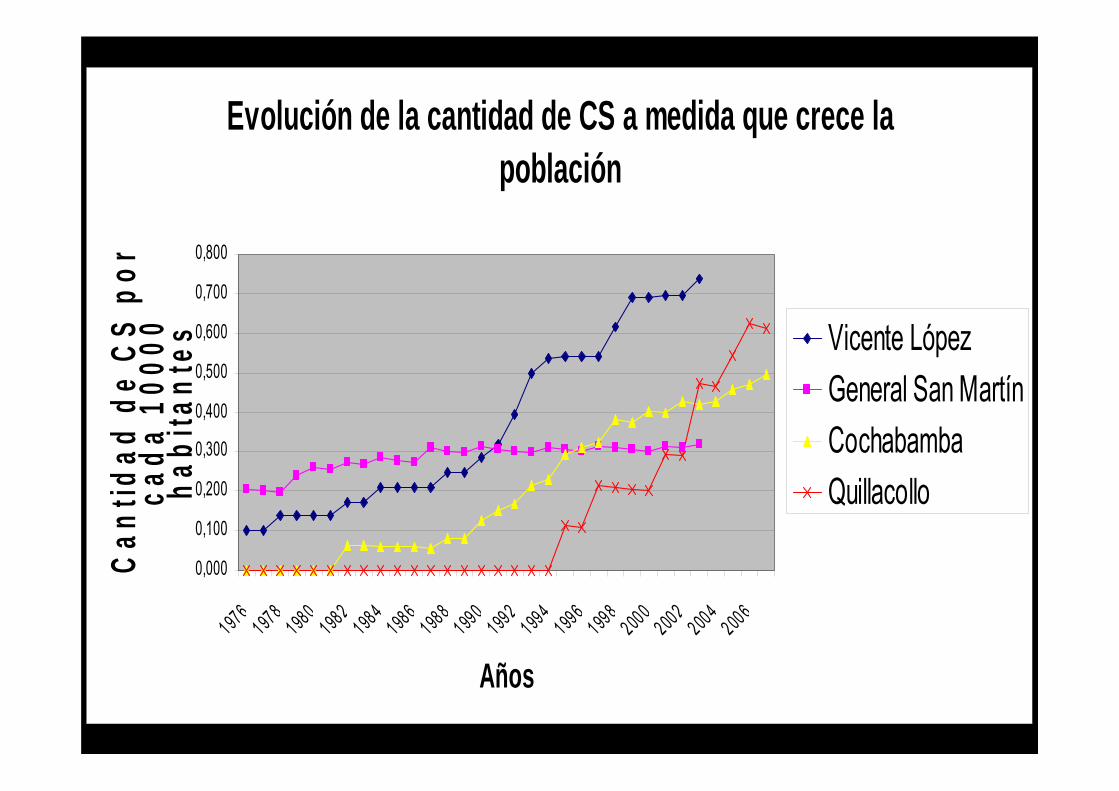
Evolución de la cantidad de CS a medida que crece la población
0,000
0,100
0,200
0,300
0,400
0,500
0,600
0,700
0,800
1976197819801982198419861988199019921994199619982000200220042006
Años
Can
tidad
de
CS
por
cada
100
00
habi
tant
es Vicente LópezGeneral San MartínCochabambaQuillacollo
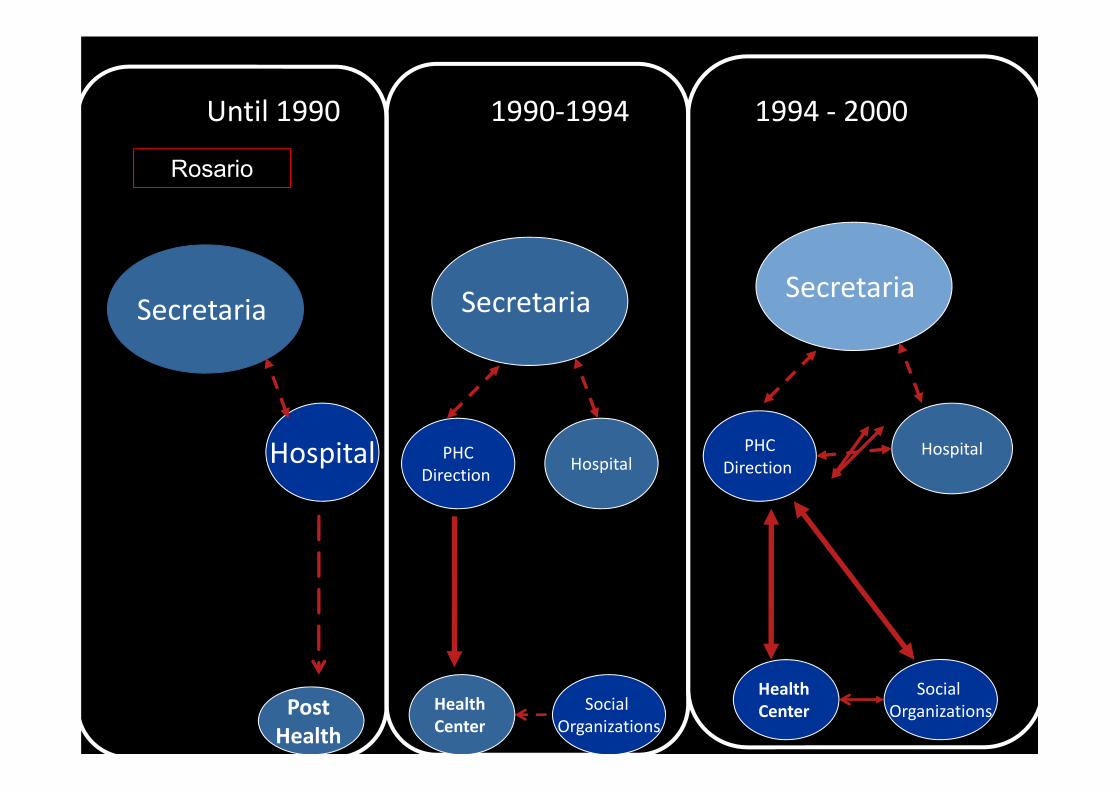
Hospital
Secretaria
Until 1990 1990‐1994 1994 ‐ 2000
Post Health
Social Organizations
Secretaria
HospitalPHCDirection
Health Center
Social Organizations
Secretaria
HospitalPHCDirection
Health Center
Rosario
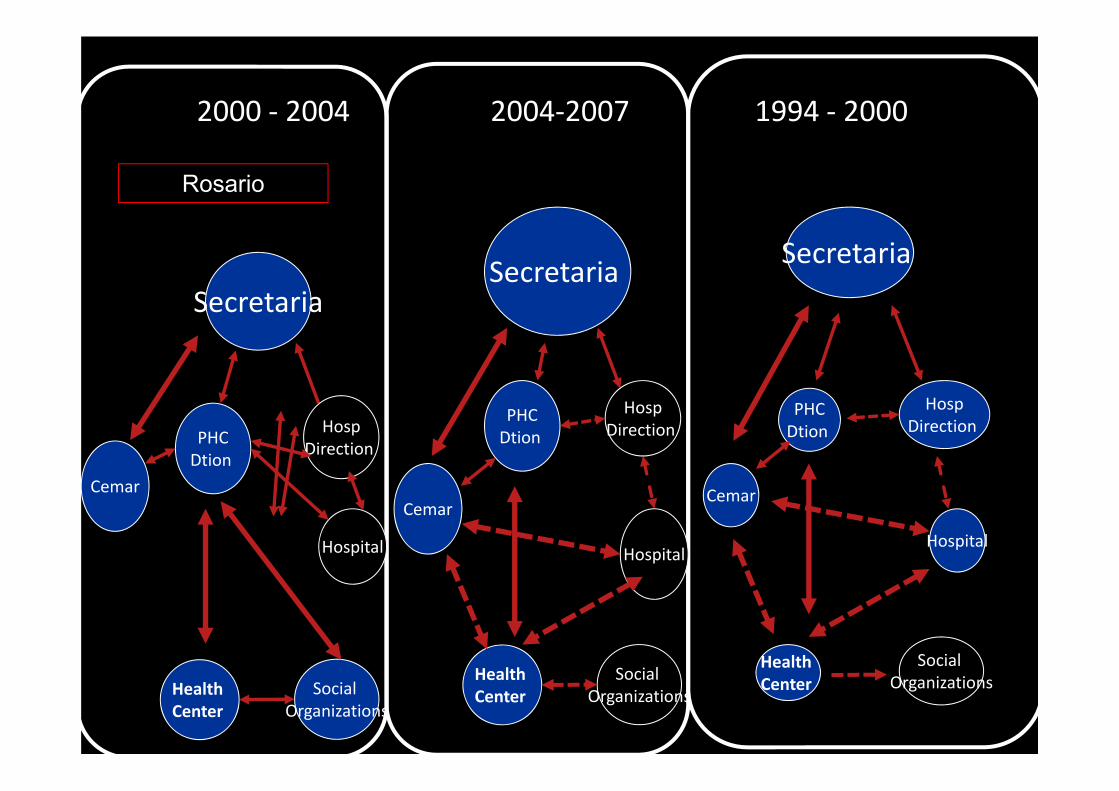
2000 ‐ 2004 2004‐2007 1994 ‐ 2000
Social Organizations
Secretaria
Hospital
PHCDtion
Health Center
Cemar
Social Organizations
Secretaria
Hospital
PHCDtion
Health Center
Cemar
HospDirection
HospDirection
Social Organizations
Secretaria
Hospital
PHCDtion
Health Center
Cemar
HospDirection
Rosario
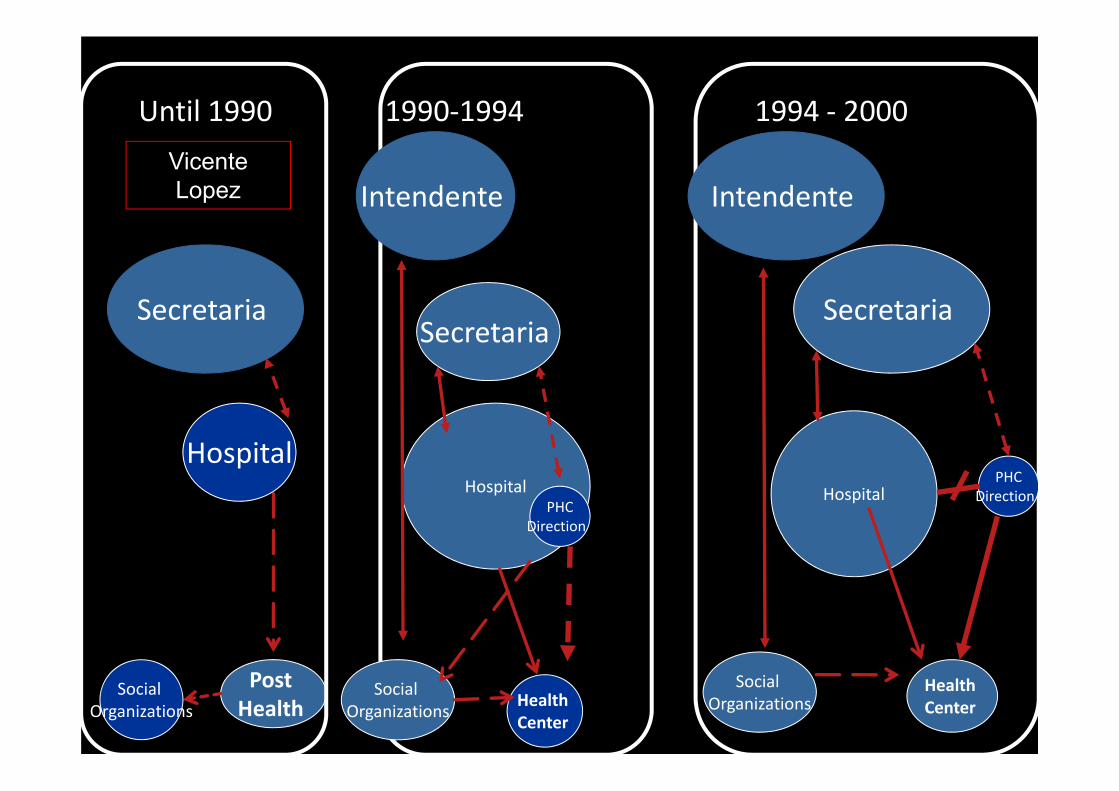
Hospital
Secretaria
Until 1990 1990‐1994 1994 ‐ 2000
Post Health
Social Organizations
Secretaria
HospitalPHC
Direction
HealthCenter
Social Organizations
Intendente
Social Organizations
Secretaria
HospitalPHC
Direction
Health Center
Intendente Vicente Lopez
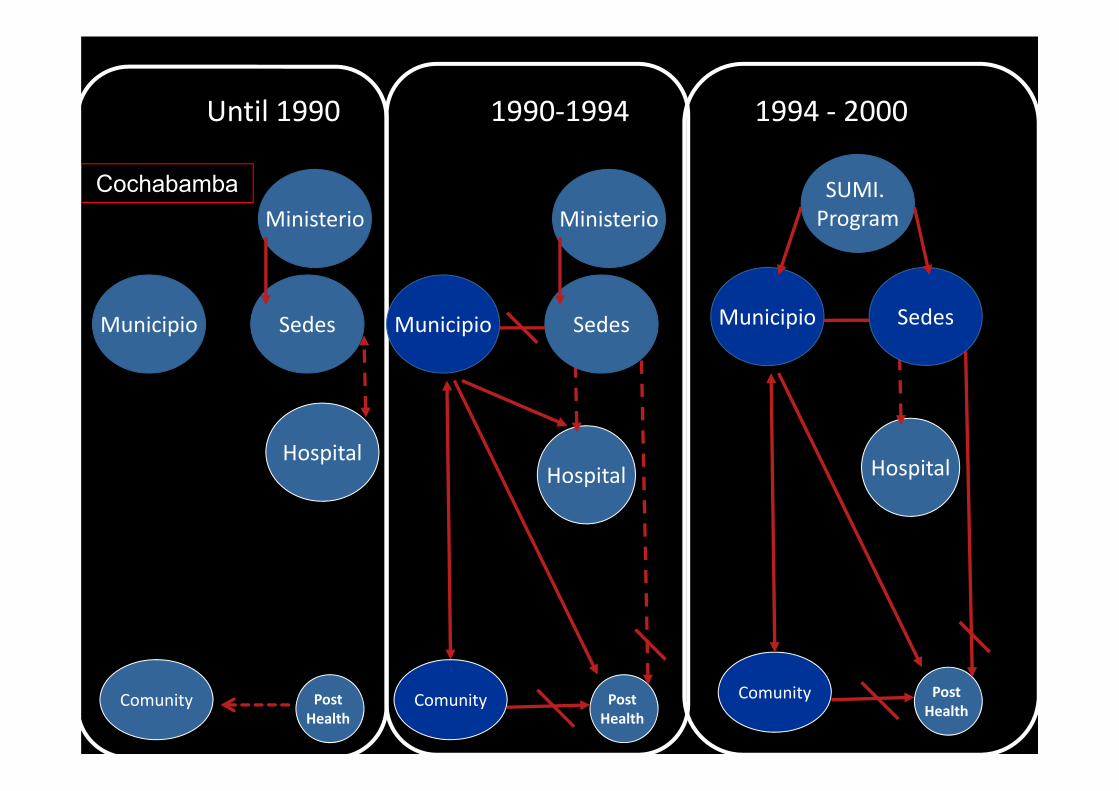
Hospital
Municipio
Until 1990 1990‐1994 1994 ‐ 2000
Post Health
Comunity
Sedes
Ministerio
Hospital
Municipio
Post Health
Comunity
Sedes
Ministerio
Hospital
Municipio
Post Health
Comunity
Sedes
SUMI. Program
Cochabamba
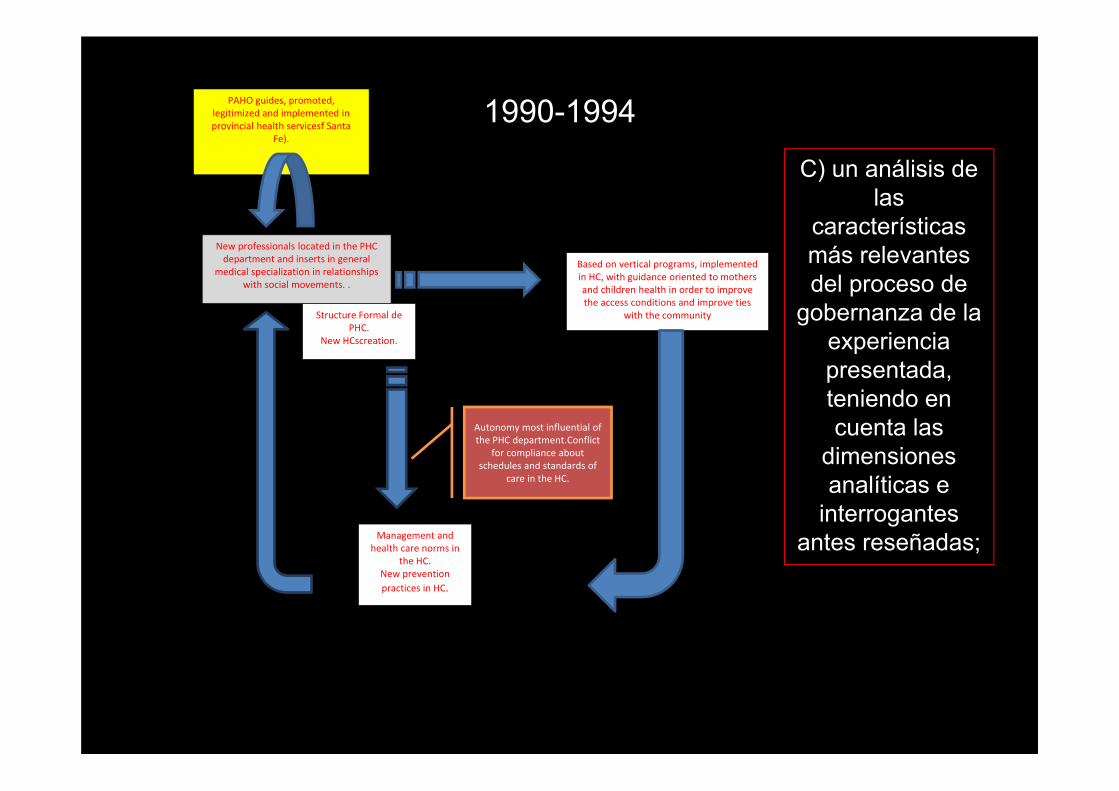
PAHO guides, promoted, legitimized and implemented in provincial health servicesf Santa
Fe).
New professionals located in the PHC department and inserts in general
medical specialization in relationships with social movements. .
Based on vertical programs, implemented in HC, with guidance oriented to mothers and children health in order to improve the access conditions and improve ties
with the communityStructure Formal de PHC.
New HCscreation.
Management and health care norms in
the HC. New prevention practices in HC.
Autonomy most influential of the PHC department.Conflict
for compliance about schedules and standards of
care in the HC.
1990-1994
C) un análisis de las
características más relevantes del proceso de
gobernanza de la experiencia presentada, teniendo en cuenta las
dimensiones analíticas e
interrogantes antes reseñadas;
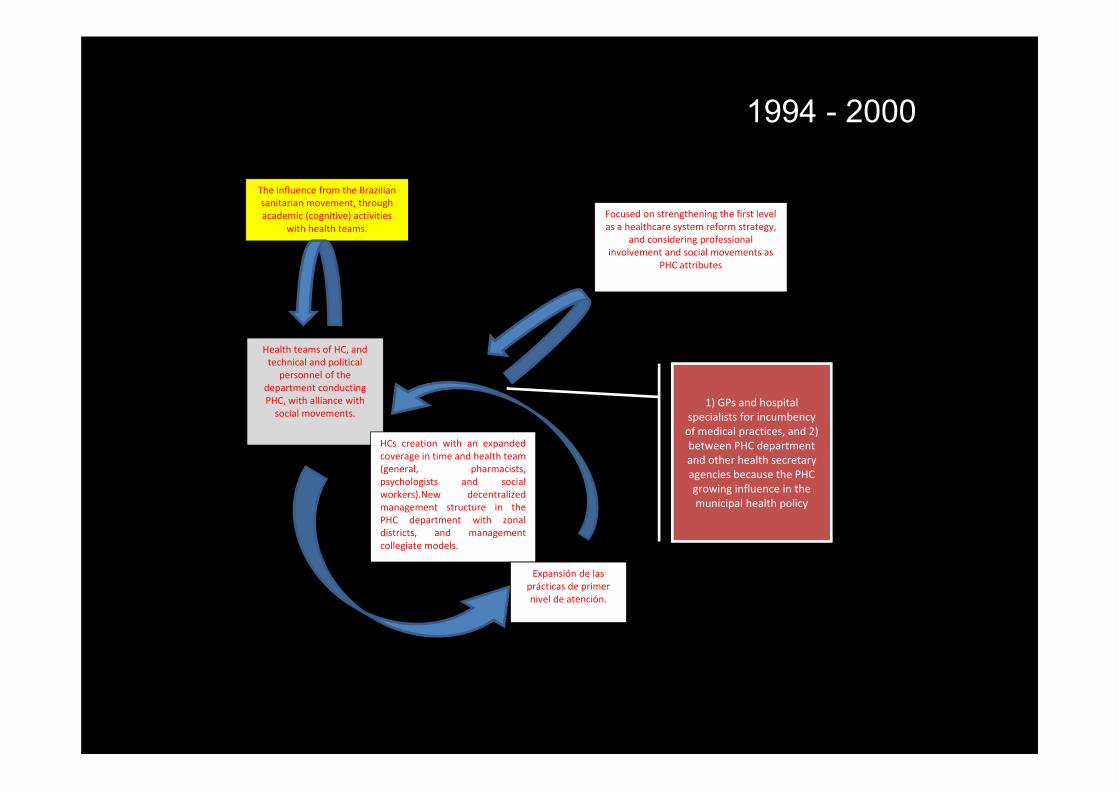
The influence from the Brazilian sanitarian movement, through academic (cognitive) activities
with health teams.
Health teams of HC, and technical and political
personnel of the department conducting PHC, with alliance with social movements.
HCs creation with an expandedcoverage in time and health team(general, pharmacists,psychologists and socialworkers).New decentralizedmanagement structure in thePHC department with zonaldistricts, and managementcollegiate models.
Expansión de las prácticas de primer nivel de atención.
Focused on strengthening the first level as a healthcare system reform strategy,
and considering professional involvement and social movements as
PHC attributes
1) GPs and hospital specialists for incumbency of medical practices, and 2) between PHC department and other health secretary agencies because the PHC growing influence in the municipal health policy
1994 - 2000
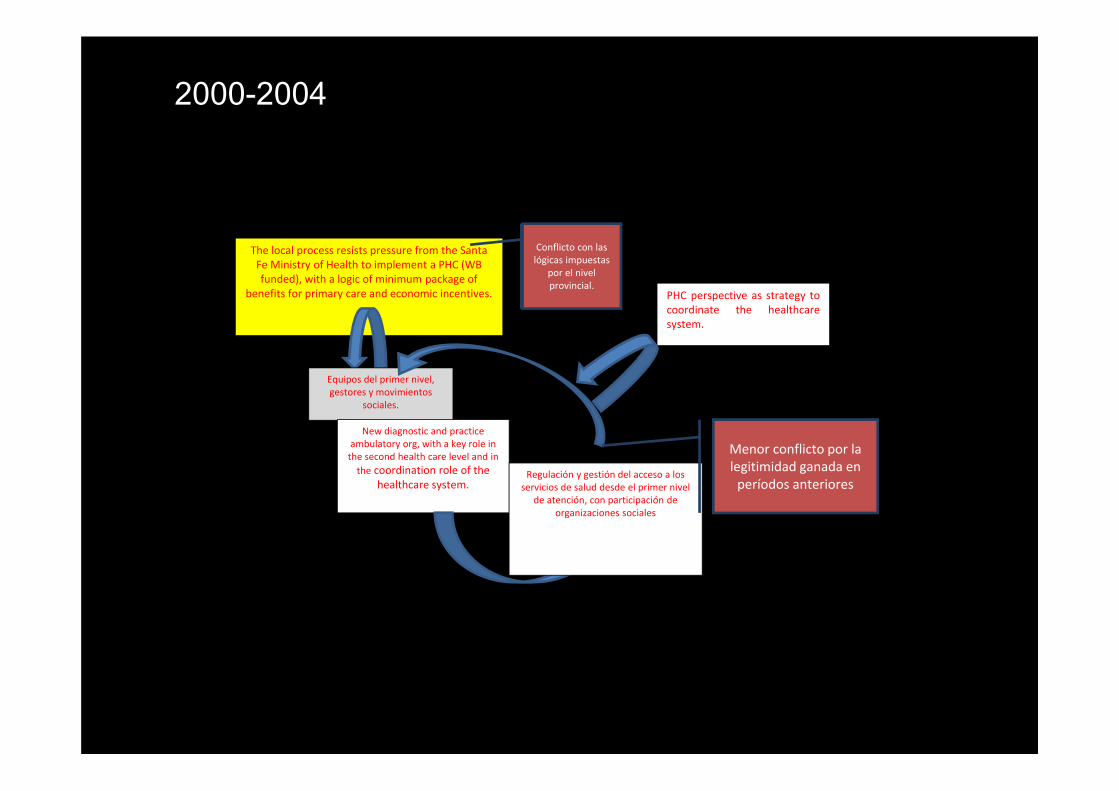
The local process resists pressure from the Santa Fe Ministry of Health to implement a PHC (WB funded), with a logic of minimum package of
benefits for primary care and economic incentives.
Conflicto con las lógicas impuestas
por el nivel provincial.
Equipos del primer nivel, gestores y movimientos
sociales.
New diagnostic and practice ambulatory org, with a key role in the second health care level and in the coordination role of the
healthcare system.Regulación y gestión del acceso a los servicios de salud desde el primer nivel
de atención, con participación de organizaciones sociales
Menor conflicto por la legitimidad ganada en períodos anteriores
PHC perspective as strategy tocoordinate the healthcaresystem.
2000-2004
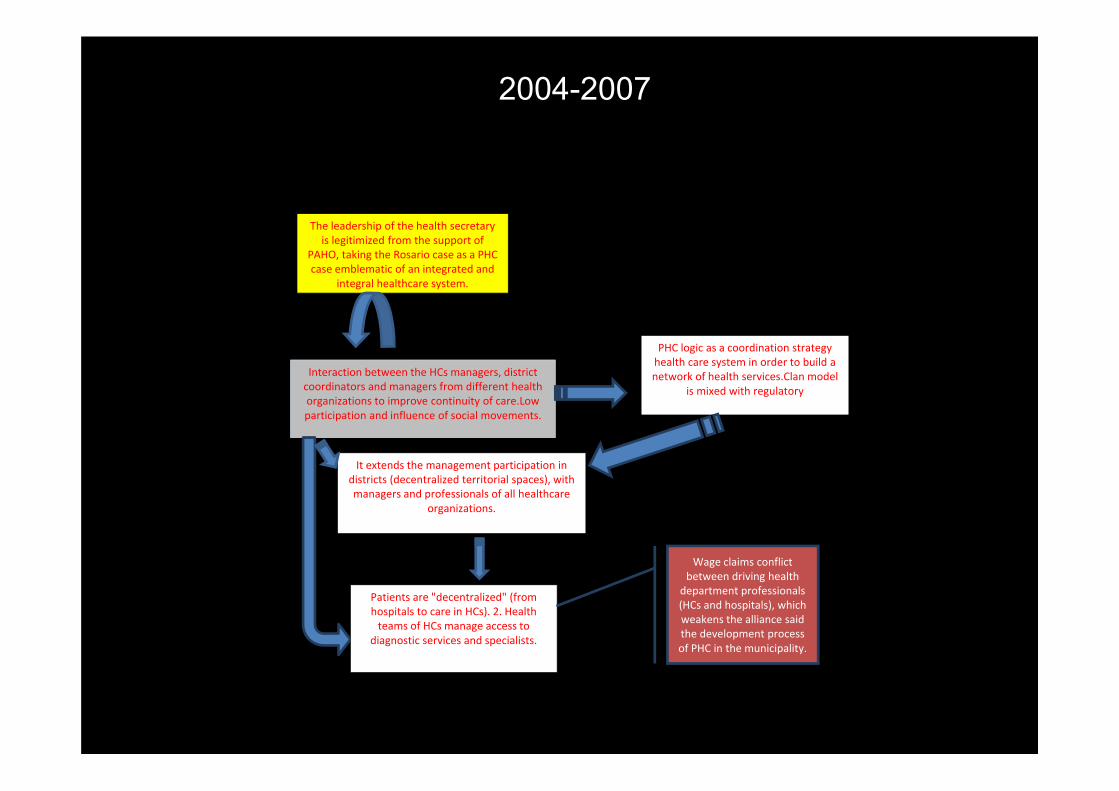
The leadership of the health secretary is legitimized from the support of
PAHO, taking the Rosario case as a PHC case emblematic of an integrated and
integral healthcare system.
Interaction between the HCs managers, district coordinators and managers from different health organizations to improve continuity of care.Lowparticipation and influence of social movements.
It extends the management participation in districts (decentralized territorial spaces), with managers and professionals of all healthcare
organizations.
Patients are "decentralized" (from hospitals to care in HCs). 2. Health teams of HCs manage access to
diagnostic services and specialists.
Wage claims conflict between driving health
department professionals (HCs and hospitals), which weakens the alliance said the development process of PHC in the municipality.
PHC logic as a coordination strategy health care system in order to build a network of health services.Clan model
is mixed with regulatory
2004-2007
¿en qué medida y de qué forma el proyecto promovió el análisis, diseño y/o implementación de una respuesta intersectorial a los
determinantes sociales y ambientales de la salud?
A través del análisis de:
1) los actores involucrados. 2) las innovaciones organizacionales
producidas, qué tipo de prácticas realizadas y en qué tipo de organizaciones.
3) sus efectos sobre las condiciones de acceso a los servicios.
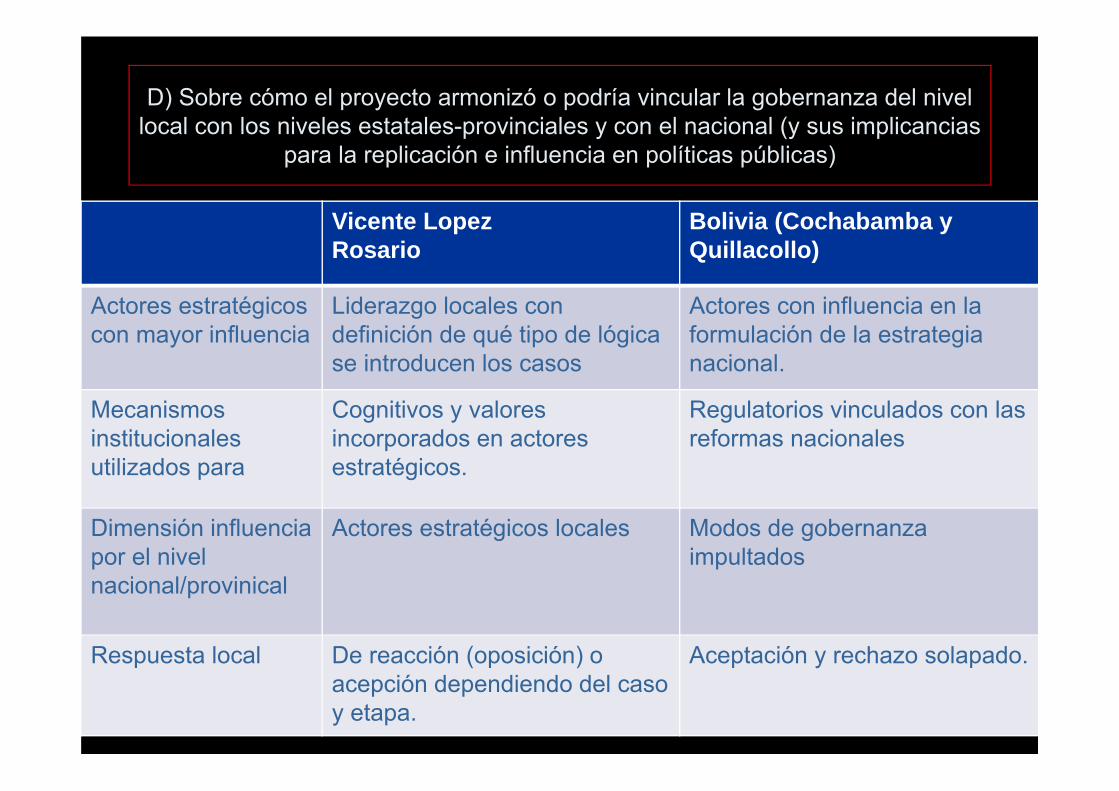
D) Sobre cómo el proyecto armonizó o podría vincular la gobernanza del nivel local con los niveles estatales-provinciales y con el nacional (y sus implicancias
para la replicación e influencia en políticas públicas)
Vicente LopezRosario
Bolivia (Cochabamba y Quillacollo)
Actores estratégicos con mayor influencia
Liderazgo locales con definición de qué tipo de lógicase introducen los casos
Actores con influencia en la formulación de la estrategianacional.
Mecanismos institucionalesutilizados para
Cognitivos y valoresincorporados en actoresestratégicos.
Regulatorios vinculados con lasreformas nacionales
Dimensión influenciapor el nivelnacional/provinical
Actores estratégicos locales Modos de gobernanzaimpultados
Respuesta local De reacción (oposición) o acepción dependiendo del casoy etapa.
Aceptación y rechazo solapado.
E) ¿Cuál fue la estrategia del proyecto para difundir la investigación a tomadores de decisión y actores sociales, con el propósito de facilitar el uso de los resultados? ¿Cómo y cuándo se involucraron los actores no académicos?
• Learning through previous project.• Importance of early involvement of
stakeholders and articulation of the knowledge process between diferent “logics”
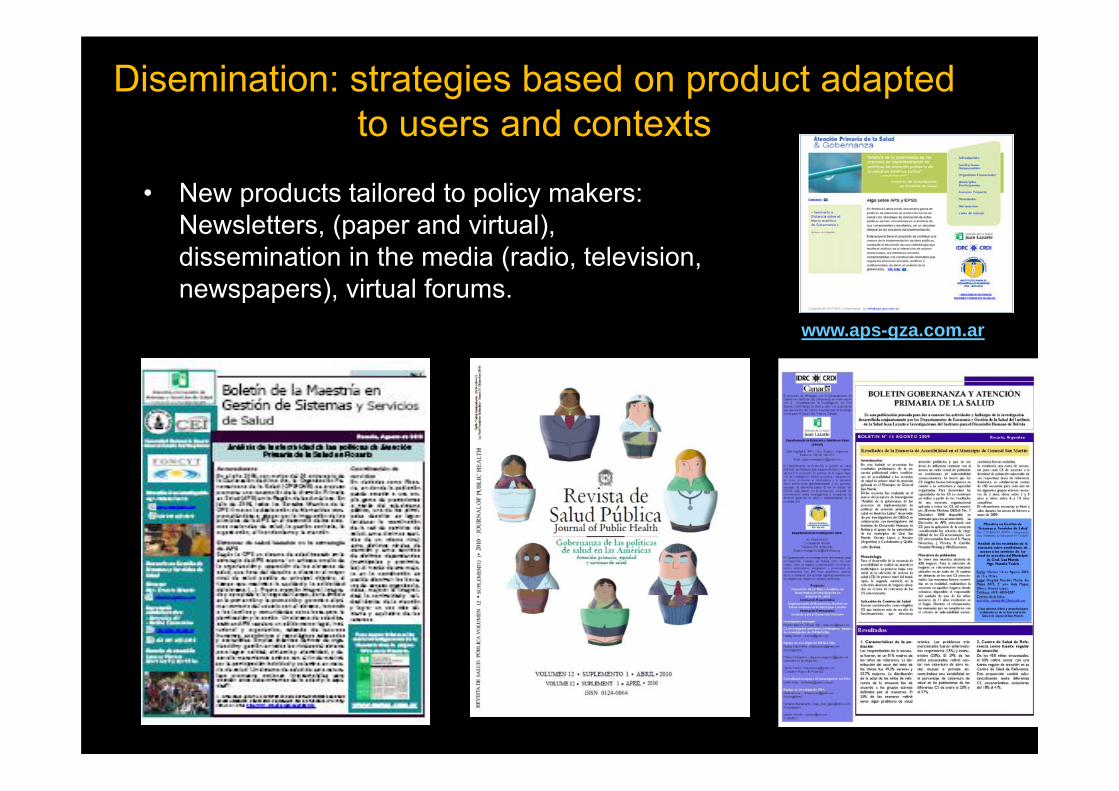
Disemination: strategies based on product adapted to users and contexts
• New products tailored to policy makers: Newsletters, (paper and virtual), dissemination in the media (radio, television, newspapers), virtual forums.
www.aps-gza.com.ar

Product Innovations: media
Newpapers
Television
Radio
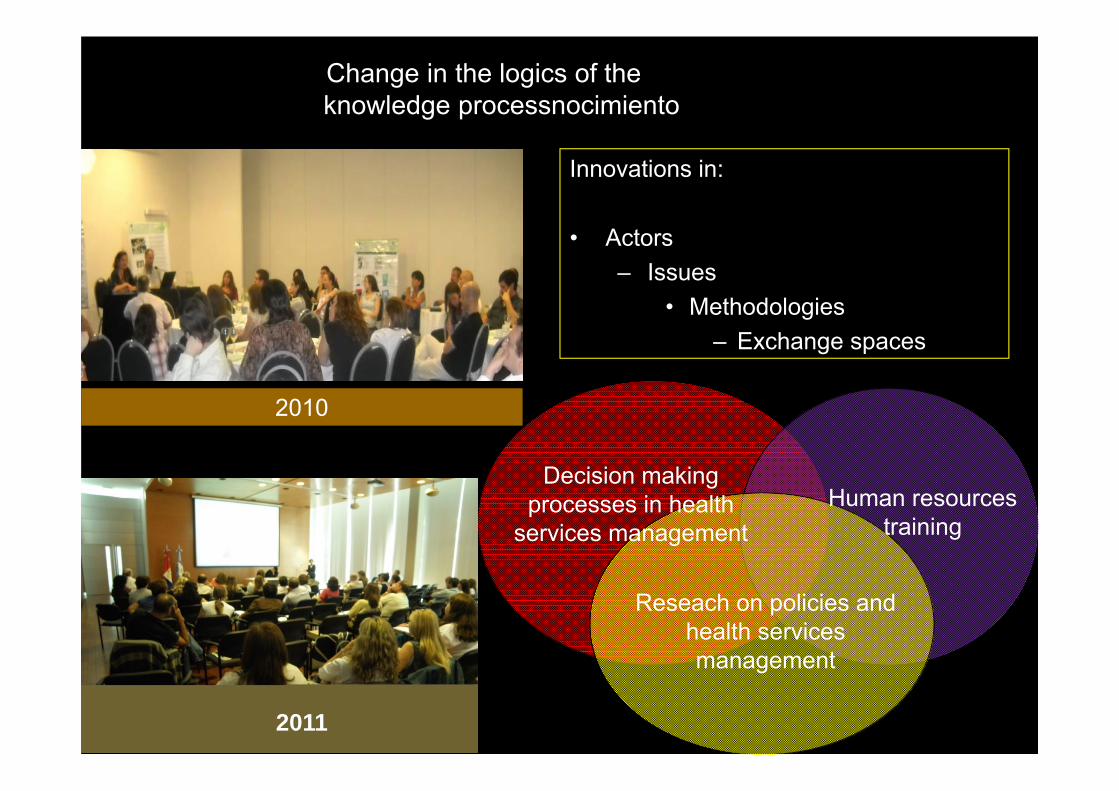
Human resources training
Decision making processes in health
services management
Reseach on policies and health services management
Change in the logics of theknowledge processnocimiento
Innovations in:
• Actors– Issues
• Methodologies– Exchange spaces
2010
2011
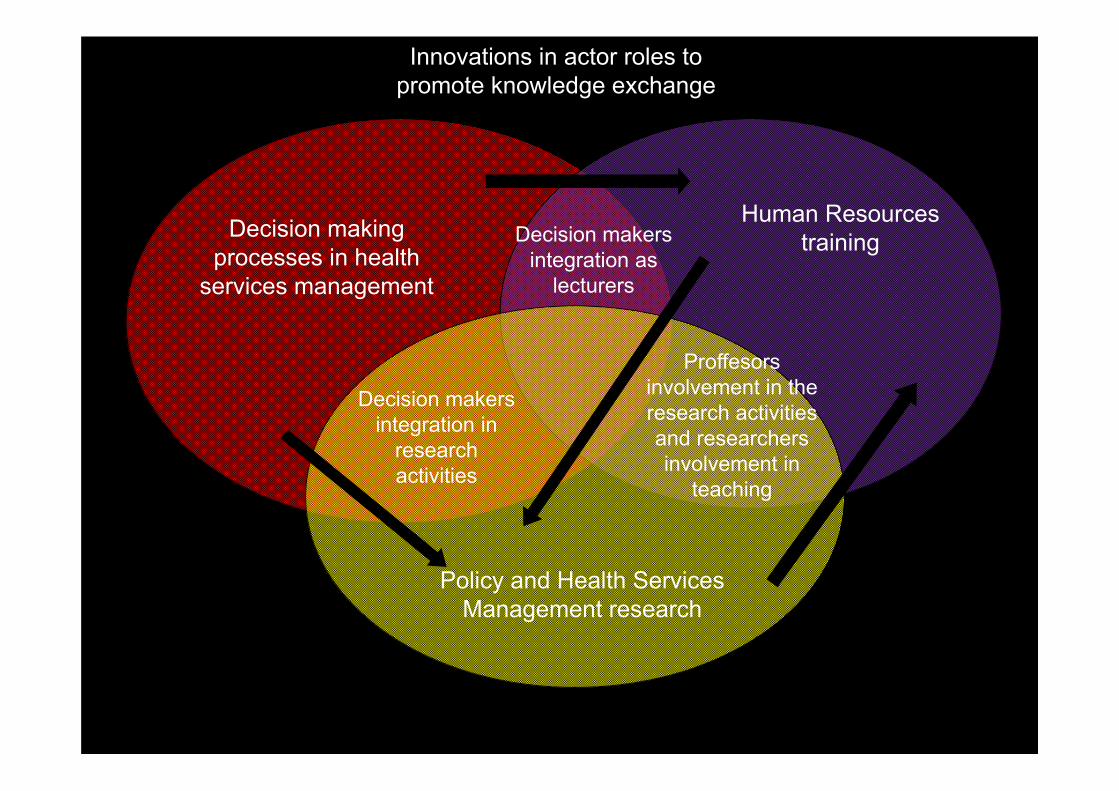
Human Resources trainingDecision making
processes in health services management
Policy and Health Services Management research
Decision makers integration in
research activities
Proffesors involvement in the research activities and researchers involvement in
teaching
Decision makers integration as
lecturers
Innovations in actor roles to promote knowledge exchange
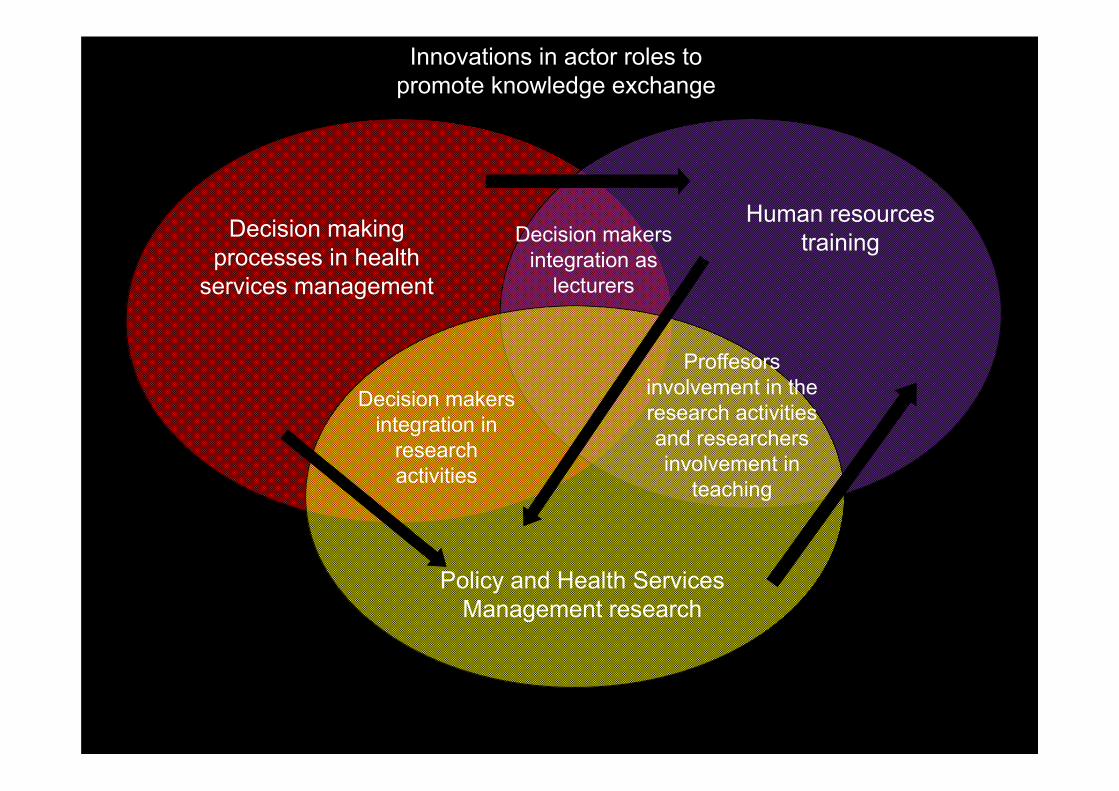
Human resources trainingDecision making
processes in health services management
Policy and Health Services Management research
Decision makers integration in
research activities
Proffesors involvement in the research activities and researchers involvement in
teaching
Decision makers integration as
lecturers
Innovations in actor roles to promote knowledge exchange
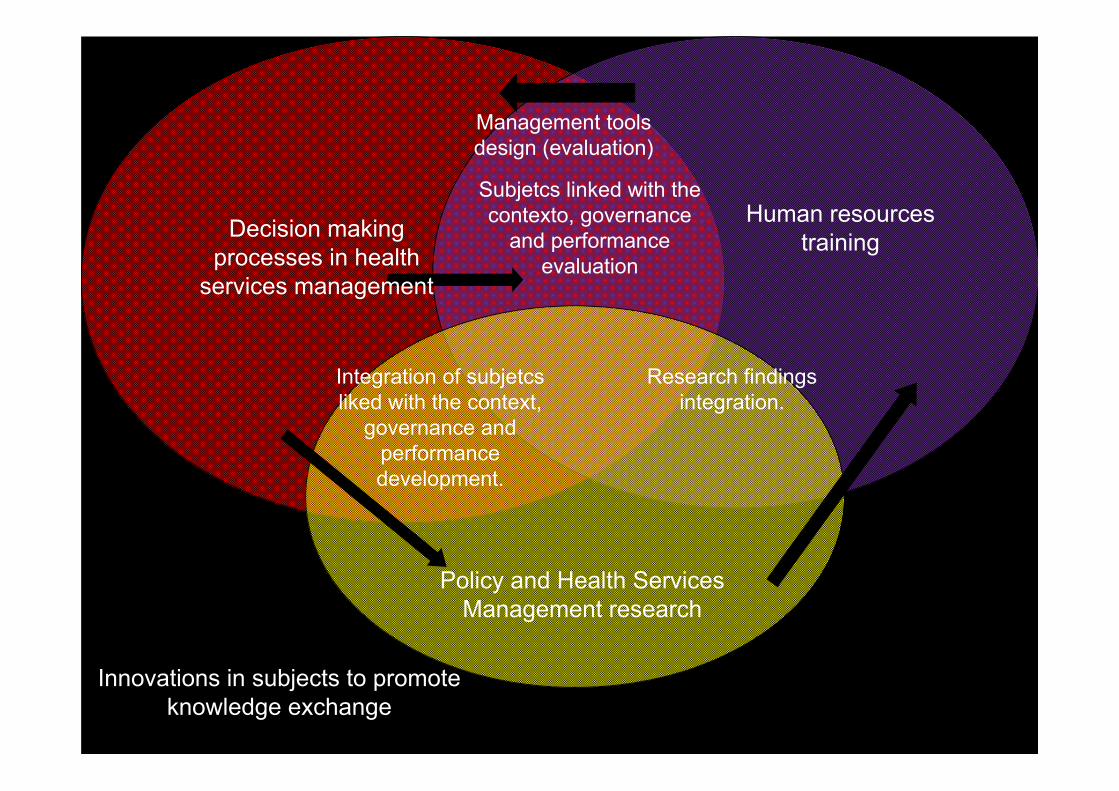
Human resources trainingDecision making
processes in health services management
Policy and Health Services Management research
Integration of subjetcs liked with the context,
governance and performance development.
Research findings integration.
Subjetcs linked with the contexto, governance
and performance evaluation
Innovations in subjects to promote knowledge exchange
Management tools design (evaluation)
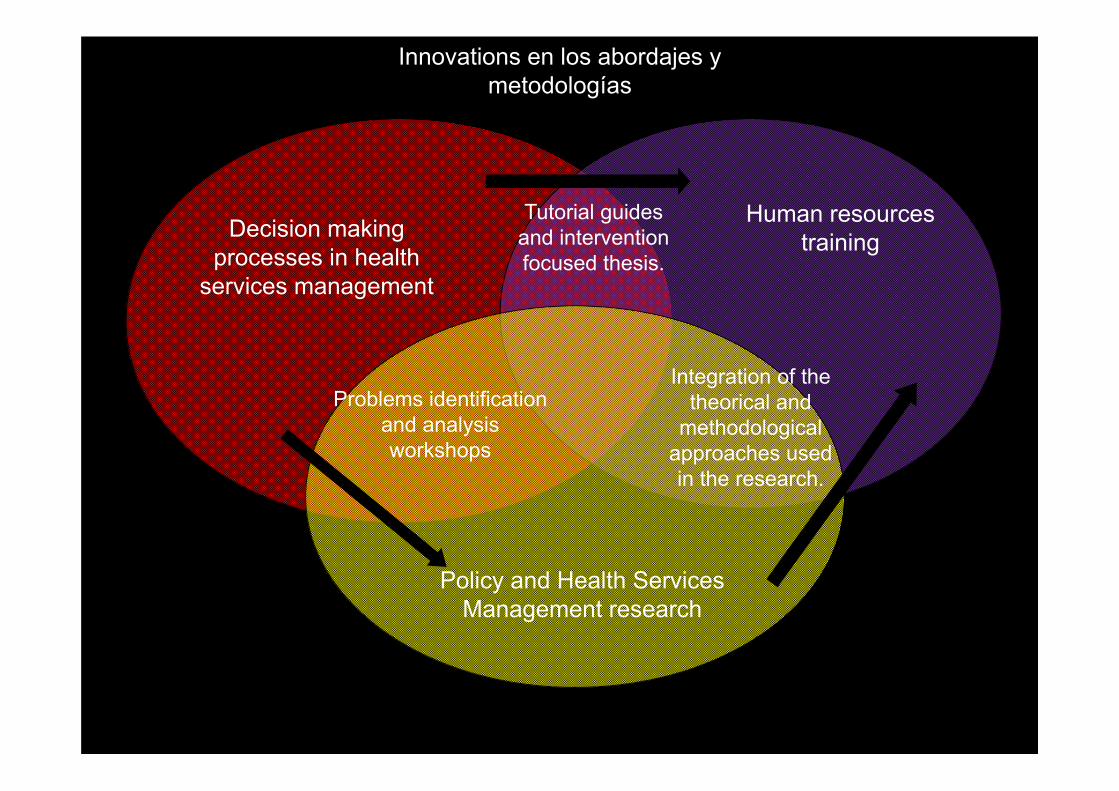
Human resources trainingDecision making
processes in health services management
Policy and Health Services Management research
Problems identification and analysis workshops
Integration of the theorical and
methodological approaches used in the research.
Tutorial guides and intervention focused thesis.
Innovations en los abordajes y metodologías
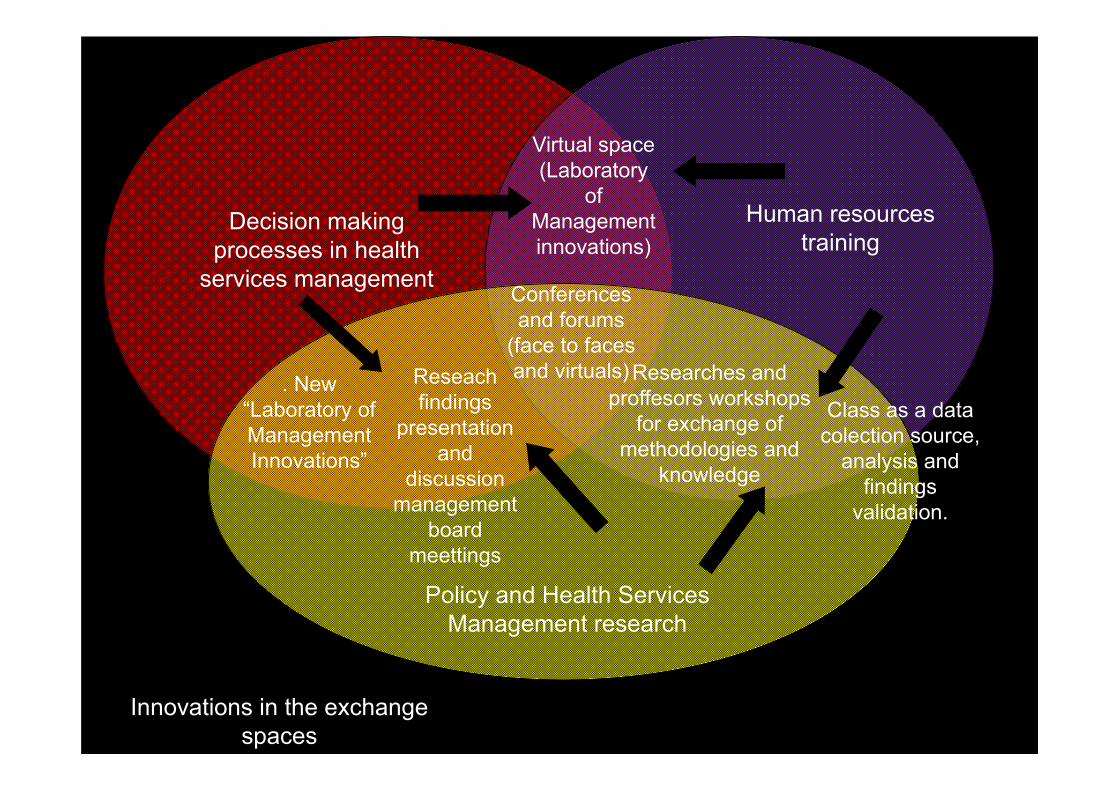
Human resources training
Decision making processes in health
services management
Policy and Health Services Management research
Reseach findings
presentation and
discussion management
board meettings
Researches and proffesors workshops
for exchange of methodologies and
knowledge
Virtual space (Laboratory
of Management innovations)
Innovations in the exchange spaces
Conferences and forums
(face to faces and virtuals). New
“Laboratory of Management Innovations”
Class as a data colection source,
analysis and findings
validation.
Some lessons learned from KT strategies
• If KT can turn into a component of the governance model, KT mechanisms are more effective.
• Nevertheless, it’s necesary a huge integration decision makers and research producers effort to integrate different logics (actors, subjects, methodologies and exchange space).