Evolución de la VM con presión positivaintensivo.sochipe.cl/subidos/catalogo3/historia VM.pdf ·...
130
Evolución de la VM con presión positiva Guillermo Bugedo Departamento de Medicina Intensiva Pontificia Universidad Católica de Chile [email protected] Sunday, April 25, 2010
Transcript of Evolución de la VM con presión positivaintensivo.sochipe.cl/subidos/catalogo3/historia VM.pdf ·...

Evolución de la VM con presión positiva
Guillermo BugedoDepartamento de Medicina Intensiva
Pontificia Universidad Católica de [email protected]
Sunday, April 25, 2010

evolución de la VM con presión positiva
• historia• principios físicos básicos• SDRA y fisiopatología• daño inducido por la VM y ventilación protectora• generaciones de ventiladores
Sunday, April 25, 2010

“…you must attempt an opening in the trunk of the trachea and pass into it a tube…, …and you must blow into this so that the lung may expand…, …and the heart take strength afresh and exhibit a great variety of motions”.
From “De humani coporis fabrica”, by Andreas Vesalius (1543).
Sunday, April 25, 2010

Robert Hooke(1635-1703)
Sunday, April 25, 2010

1667: Keeping a dog alive by blowing through its lungs with bellows
Sunday, April 25, 2010

1667: Keeping a dog alive by blowing through its lungs with bellows
Hooke's law: the stress imposed on a solid is directly proportional to the strain produced, within the elastic limit
Sunday, April 25, 2010

Sunday, April 25, 2010

(+)
Sunday, April 25, 2010

(-) (-)
(+)
Sunday, April 25, 2010

“Spirophore”
Eugéne Woillez, 1876
Sunday, April 25, 2010

the “iron lung”
Sunday, April 25, 2010

1952: la epidemia de poliomielitis y los ventiladores de presión positiva
Sunday, April 25, 2010

epidemic of poliomyelitis in Copenhagen
• “It is doubtful indeed if any city of the size of Copenhagen has ever experienced an outbreak of similar magnitude ... for many weeks we received thirty to fifty patients daily, of whom six to twelve were desperately ill ... drowning in their own secretions.
• As we felt that the application of modern principles of anaesthesia to the problem of obstructed airways and respiratory insufficiency in poliomyelitis might improve our results anaesthetists were invited to join our staff, the first being Dr. Bjørn Ibsen.”
Lassen HCA (1954) The Epidemic of Poliomyelitis in Copenhagen, 1952. Proc Roy. Soc. Med 47:67
Sunday, April 25, 2010

epidemic of poliomyelitis in Copenhagen
Sunday, April 25, 2010

epidemic of poliomyelitis in Copenhagen
• Dr Bjørn Ibsen was called into consultation on August 25th.
• In the preceding three weeks there had been 31 patients with life threatening poliomyelitis; 28 of these had died.
Bjørn Ibsen
Lassen HCA (1954) The Epidemic of Poliomyelitis in Copenhagen, 1952. Proc Roy. Soc. Med 47:67
Sunday, April 25, 2010

epidemic of poliomyelitis in Copenhagen
• On August 27th the first patient was treated with the method that was to become the treatment of choice:– tracheotomy just below the
larynx– inflatable rubber cuff tube in
trachea– frequent suction– repeated bronchoscopy– postural drainage– manual positive pressure
ventilation using oxygen and nitrogen.
Lassen HCA (1954) The Epidemic of Poliomyelitis in Copenhagen, 1952. Proc Roy. Soc. Med 47:67
Sunday, April 25, 2010

manual positive pressure ventilation
Sunday, April 25, 2010

epidemic of poliomyelitis in Copenhagen
• At times there were as many as 70 patients requiring artificial respiration.
• Students from the University provided the manpower (handpower!). Overall 1400 students were involved during the course of the epidemic. None of them contracted the disease.
• By the end of the year the mortality in these severe cases had fallen from 87% to 26%.
Lassen HC. A preliminary report on the 1952 epidemic of poliomyelitis in Copenhagen with special reference to the treatment of acute respiratory insufficiency. Lancet. 1953 Jan 3;1(6749):37-41.
Sunday, April 25, 2010

los ventiladores de presión
Sunday, April 25, 2010

first use of the Clevedon ventilator
Macrae et al, September 1953
Sunday, April 25, 2010

P
t
t
V
gentileza Dr J. Urzúa
P límite
Sunday, April 25, 2010

P
t
t
V
gentileza Dr J. Urzúa
P límite
Sunday, April 25, 2010

ventilador de presión
ventilador de presión
IN: t LIM: P CIC: P
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

ventilador de presión
ventilador de presión
IN: t LIM: P CIC: P
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

ventilador de presión
ventilador de presión
IN: t LIM: P CIC: P
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

ventilador de presión
ventilador de presión
IN: t LIM: P CIC: P
Presión(cmH2O)
Flujo(lpm)
riesgo de hipoventilación-pat restrictiva-pat obstructiva-tos-desadaptación
Sunday, April 25, 2010

Bird Mark 7
circa 1955
Sunday, April 25, 2010

Puritan-Bennett PR-2
circa 1963
Sunday, April 25, 2010

la medicina intensiva había nacido…
Sunday, April 25, 2010

Ashbaugh DG, Bigelow DB, Petty TL, Levine BEAcute respiratory distress in adults
Lancet, 1967 Aug 12
Sunday, April 25, 2010

• The article outlined clinical, radiological, biochemical and pathological features of a pattern of acute respiratory distress in 12 patients:
• “The clinical pattern... includes severe dyspnoea, tachypnoea, cyanosis that is refractory to oxygen therapy, loss of lung compliance, and a diffuse alveolar infiltrate seen on chest X-ray”.
• It was noted that none of the patients had chronic lung disease and the precipitant of the disorder was varied with severe trauma preceding onset in seven patients, viral infection in four patients and pancreatitis in one patient.
Ashbaugh DG, Bigelow DB, Petty TL, Levine BEAcute respiratory distress in adults
Lancet, 1967 Aug 12
Sunday, April 25, 2010

• Chest X-ray appearances consisted of “patchy, bilateral alveolar infiltrates”, the severity of which paralleled the clinical condition.
• “At necropsy in seven patients, gross inspection showed heavy and deep reddish-purple lungs... the appearance resembled liver tissue”.
• Microscopic appearances were consistent with current descriptions, including the hyaline membrane which prompted comparison with neonatal respiratory distress syndrome.
Ashbaugh DG, Bigelow DB, Petty TL, Levine BEAcute respiratory distress in adults
Lancet, 1967 Aug 12
Sunday, April 25, 2010

discussion (1967…)
• “In view of the similar response of the lung to a variety of stimuli, a common mechanism of injury is postulated. The loss of lung compliance, refractory cyanosis, and microscopic atelectasis point to alveolar instability as a likely source of trouble”.
• They postulated that surfactant dysfunction was a significant contributor to alveolar collapse and acknowledged that PEEP may be beneficial in preventing atelectasis.
• but, “The use of PEEP merely buys time: unless the underlying process can be successfully treated or reversed the prognosis is grave”.
Ashbaugh DG, Bigelow DB, Petty TL, Levine BEAcute respiratory distress in adults
Lancet, 1967 Aug 12
Sunday, April 25, 2010

y aquí empezó a usarse el PEEP…
Sunday, April 25, 2010

válvulas de umbral (threshold resistor)
presión
flujo
presión = F / s
Sunday, April 25, 2010

válvulas de umbral (threshold resistor)
presión
flujo
presión = F / s
Sunday, April 25, 2010

presión
flujo
válvulas de flujo
presión = R x flujo
Sunday, April 25, 2010

presión
flujo
válvulas de flujo
presión = R x flujo
Sunday, April 25, 2010

Falke KJ, et al.J Clin Invest. 1972 Sep;51(9):2315-23.
Sunday, April 25, 2010

Falke KJ, et al.J Clin Invest. 1972 Sep;51(9):2315-23.
• 10 patients• Pa:FiO2<300 on ZEEP• Vt 8.9 to 24.1 ml/kg• ZEEP and PEEP 5, 10, and
15 cmH20
Sunday, April 25, 2010

estudio internacional VM...
• 15.757 pac’s admitidos a 361 UCI’s en marzo 1998…• 5.183 (33%) →VM x 6 días ( 31%)• 231 (4,5%) pac’s SDRA ( 52%)
día 1 día 2 día 3• pac’s 231 174 82• PEEP, media±DS 8±4 9±3 9±3
mediana (rango) 8 (5-10) 10 (6-12) 9 (5-12)• pac’s sin PEEP 34 (16%) 14 (8%) 8 (10%)
Esteban A, et al. JAMA 2002; 287: 345-355.
Sunday, April 25, 2010

estudio internacional VM...
• 15.757 pac’s admitidos a 361 UCI’s en marzo 1998…• 5.183 (33%) →VM x 6 días ( 31%)• 522 (10,1%) pac’s COPD ( 22%)
día 1 día 2 día 3• pac’s 522 283 85• PEEP, media±DS 5±2 5±2 6±3
mediana (rango) 5 (4-5) 5 (5-6) 5 (4-7)• pac’s sin PEEP 218 (47%) 128 (45%) 33 (39%)
Esteban A, et al. JAMA 2002; 287: 345-355.
Sunday, April 25, 2010

los ventiladores de volumen
Sunday, April 25, 2010

ventilador de presión vs volumen
ventilador de presión
IN: t LIM: P CIC: P
ventilador devolumen
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

ventilador de presión vs volumen
ventilador de presión
IN: t LIM: P CIC: P
ventilador devolumen
IN: t LIM: V CIC: t
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

ventilador de presión vs volumen
ventilador de presión
IN: t LIM: P CIC: P
ventilador devolumen
IN: t LIM: V CIC: t
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

Diseño mecánico (Harvard pump)
La duración del ciclo depende de la velocidad del motor. La inspiración y la espiración duran lo mismo. El límite inspiratorio es el volumen de desplazamiento del pistón. Se puede agregar válvula de escape para evitar sobrepresión. La espiración es activa (aspiración a presión negativa).
gentileza Dr J. Urzúa
Sunday, April 25, 2010

Puritan Bennett MA-1
circa 1967
Sunday, April 25, 2010

Bear-1 (“flipper”)
circa 1975
Sunday, April 25, 2010

Sunday, April 25, 2010

ventilación convencional hacia 1980…
• 1960: VM en pacientes quirúrgicos sometidos a anestesia y relajación muscular– Vt 10-15 ml/Kg para prevención de atelectasias
• 1970: principios de manejo en SDRA– Vt 10-15 ml/Kg– PEEP 5-10-15... cmH2O– PVA ↑↑↑ (controladas, pero no restringidas)– atención en efectos HMD, FiO2 y barotrauma...
• incidencia barotrauma (macro)– PVA 50 cmH2O → 50%– PVA70 cmH2O → 80%
Haake R, et al. Chest 1987; 91: 608.
Sunday, April 25, 2010

15/01 30/01
barotrauma
Sunday, April 25, 2010

14/0 45/0
Webb and Tierney. Am Rev Respir Dis 1974; 110:556-565.
edema pulmonar producido por la ventilación con presión (+) con altas presiones de inflación
Sunday, April 25, 2010

ventiladores de 3ª generación
Sunday, April 25, 2010

asistencia por presión
ventilador de presión
ventiladormicroprocesado
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

asistencia por presión
ventilador de presión
ventiladormicroprocesado
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

asistencia por presión
ventilador de presión
ventiladormicroprocesado
Presión(cmH2O)
Flujo(lpm)
Sunday, April 25, 2010

asistencia por presión
ventilador de presión
ventiladormicroprocesado
Presión(cmH2O)
Flujo(lpm)
IN: t LIM: P CIC: P IN: t-P LIM: P CIC: t-F
Sunday, April 25, 2010

Siemens 900
circa 1982
Sunday, April 25, 2010

Puritan-Bennett 7200
circa 1984
Sunday, April 25, 2010

tiempos modernos
Sunday, April 25, 2010

Wilhelm Conrad Röntgen (1845-1923)premio Nobel Física 1901
Allan M. Cormack (1924-1998)Godfrey N. Hounsfield (1919-2004)
premio Nobel Medicina 1979
Sunday, April 25, 2010

mid 80’s: baby lung
Sunday, April 25, 2010

baby lung: lung surface in ARDS is small→ main pathophysiologic principle for protective ventilation
Gattinoni L et al. Intensive Care Med 1986; 12: 137-142.Gattinoni L & Pesenti A. Intensive Care Med 2005; 31: 776–784.
mid 80’s: baby lung
Sunday, April 25, 2010

0
1000
2000
3000
4000
normal ARDS
weightgas vol
baby lung
• CT-scan study in ARDS:– densities 70-80% at ZEEP– total volume N– gas volume ↓↓↓
• small lung: less surface available for gas exchange…
Gattinoni L et al, Anesthesiology 1987.Gattinoni L et al. Intensive Care Med 1986; 12: 137-142.
Gattinoni L & Pesenti A. Intensive Care Med 2005; 31: 776–784.
Sunday, April 25, 2010

0
1000
2000
3000
4000
normal ARDS
weightgas vol
baby lung
• CT-scan study in ARDS:– densities 70-80% at ZEEP– total volume N– gas volume ↓↓↓
• small lung: less surface available for gas exchange…
Gattinoni L et al, Anesthesiology 1987.
→ main pathophysiologic principle for protective ventilation
Gattinoni L et al. Intensive Care Med 1986; 12: 137-142.Gattinoni L & Pesenti A. Intensive Care Med 2005; 31: 776–784.
Sunday, April 25, 2010
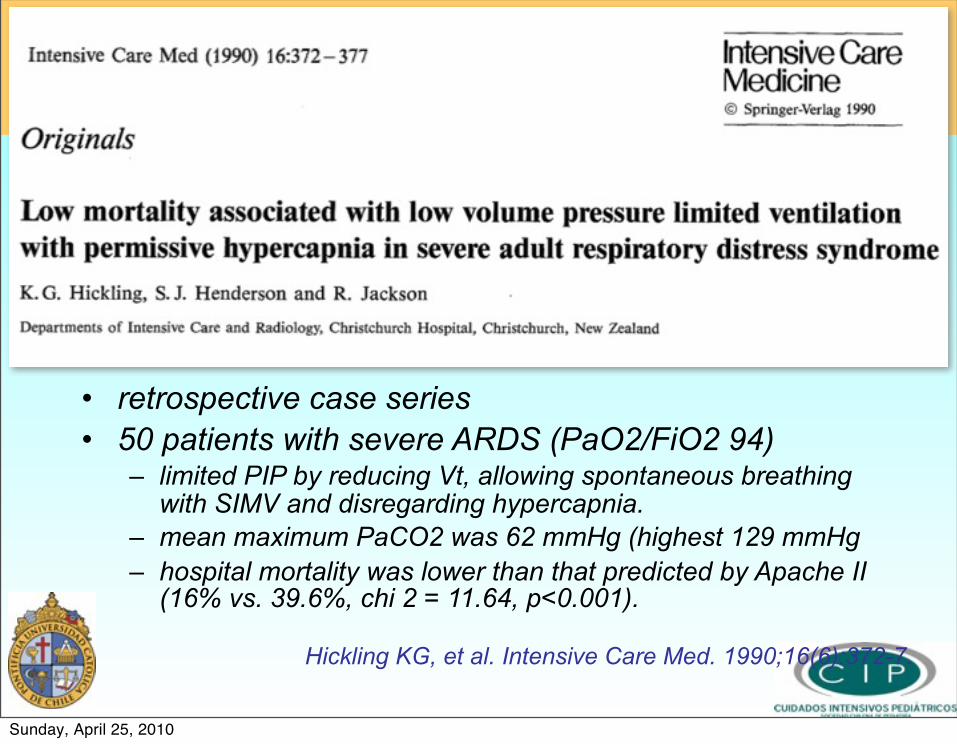
• retrospective case series• 50 patients with severe ARDS (PaO2/FiO2 94)
– limited PIP by reducing Vt, allowing spontaneous breathing with SIMV and disregarding hypercapnia.
– mean maximum PaCO2 was 62 mmHg (highest 129 mmHg– hospital mortality was lower than that predicted by Apache II
(16% vs. 39.6%, chi 2 = 11.64, p<0.001).
Hickling KG, et al. Intensive Care Med. 1990;16(6):372-7.
Sunday, April 25, 2010

el gran salto
• normalizar gases arteriales• VT elevados para prevenir atelectasias…
ventilación convencional
Sunday, April 25, 2010

el gran salto
• normalizar gases arteriales• VT elevados para prevenir atelectasias…
ventilación convencional
• mecanoprotección• limitar Vt y presiones• CO2 secundario
ventilación protectora
Sunday, April 25, 2010

el gran salto
• normalizar gases arteriales• VT elevados para prevenir atelectasias…
ventilación convencional
• mecanoprotección• limitar Vt y presiones• CO2 secundario
ventilación protectora
la hipercapnia permisiva no es una modalidad ventilatoria per se, sino una consecuencia de la ventilación con bajo Vt en un pulmón con poca superficie de intercambio (baby lung)
Sunday, April 25, 2010

the fact…!!!
Psycho (1960)
Sunday, April 25, 2010

mechanicalventilation
ALI/ARDS
the fact…!!!
Psycho (1960)
Sunday, April 25, 2010

opening-closing
• 44 pat‘s ARDS:– Pa/fiO2 ~150– LIS (Murray) 2.5
• control group (n=19)– TV 11.1 ml/Kg ®Ppl 31
cmH2O– PEEP 6.5 cmH2O– PaCO2 37.4 mmHg
• protective strategy (n=18)– TV 7.6 ml/Kg → Ppl 25
cmH2O– PEEP 14.8 cmH2O– PaCO2 46.9 mmHg
LBA
Ranieri VM et al. JAMA 1999; 282: 54-61.
control protective
TNF-α
IL-8
IL-6
Sunday, April 25, 2010

Sunday, April 25, 2010

• Brochard L, et al. AJRCCM 1998; 158: 1831-8.– 108 pac, 25 centros, SDRA<72 horas, OSF=1– low Vt: Pplat ≤25 cmH2O 48%– control: Vt ≥10 ml/Kg, Ppeak <60, PaCO2 38-42 41%
Sunday, April 25, 2010

• Brochard L, et al. AJRCCM 1998; 158: 1831-8.– 108 pac, 25 centros, SDRA<72 horas, OSF=1– low Vt: Pplat ≤25 cmH2O 48%– control: Vt ≥10 ml/Kg, Ppeak <60, PaCO2 38-42 41%
• Stewart TE, et al. N Engl J Med. 1998;338: 355-61.– 120 pac SDRA<24 horas.– low Vt: Vt ≤8 ml/Kg, Ppeak ≤30 cmH2O 48%– control: Vt 10-15, Ppeak <50 cmH2O 46%
Sunday, April 25, 2010

• Brochard L, et al. AJRCCM 1998; 158: 1831-8.– 108 pac, 25 centros, SDRA<72 horas, OSF=1– low Vt: Pplat ≤25 cmH2O 48%– control: Vt ≥10 ml/Kg, Ppeak <60, PaCO2 38-42 41%
• Stewart TE, et al. N Engl J Med. 1998;338: 355-61.– 120 pac SDRA<24 horas.– low Vt: Vt ≤8 ml/Kg, Ppeak ≤30 cmH2O 48%– control: Vt 10-15, Ppeak <50 cmH2O 46%
• Brower R, et al. Crit Care Med. 1999; 27: 1492-8.– 52 pac SDRA, algoritmo similar FiO2-PEEP.– low Vt: Vt ≤8 ml/Kg, Pplat ≤30 cmH2O 50%– control: Vt 10-12, Pplat ≤50 cmH2O 46%
Sunday, April 25, 2010

• Brochard L, et al. AJRCCM 1998; 158: 1831-8.– 108 pac, 25 centros, SDRA<72 horas, OSF=1– low Vt: Pplat ≤25 cmH2O 48%– control: Vt ≥10 ml/Kg, Ppeak <60, PaCO2 38-42 41%
• Stewart TE, et al. N Engl J Med. 1998;338: 355-61.– 120 pac SDRA<24 horas.– low Vt: Vt ≤8 ml/Kg, Ppeak ≤30 cmH2O 48%– control: Vt 10-15, Ppeak <50 cmH2O 46%
• Brower R, et al. Crit Care Med. 1999; 27: 1492-8.– 52 pac SDRA, algoritmo similar FiO2-PEEP.– low Vt: Vt ≤8 ml/Kg, Pplat ≤30 cmH2O 50%– control: Vt 10-12, Pplat ≤50 cmH2O 46%
• Amato M, et al. NEJM 1998; 338: 347-354.– 53 pac SDRA, algoritmo similar FiO2-PEEP.– low Vt: curva P-V, Vt ≤4-6, PEEP 16, hipercapnia 38%– control: Vt 11-12, least PEEP (8-9), normocarbia 71%
Sunday, April 25, 2010

Sunday, April 25, 2010

Sunday, April 25, 2010

Vt 6 ml/kg: mort 31%Vt 12 ml/kg: mort 39%
Sunday, April 25, 2010

Tobin MJ. Culmination of an era in research on the ARDS.N Engl J Med 2000; 342: 1360–1361.
ARDS network: ¿fin de la historia?
Sunday, April 25, 2010

Tobin MJ. Culmination of an era in research on the ARDS.N Engl J Med 2000; 342: 1360–1361.
→Vt 6 ml / kg… estándar en SDRA...
ARDS network: ¿fin de la historia?
Sunday, April 25, 2010

clinical trials
Protective ControlAuthor n Ppl PEEP Mort Ppl PEEP Mort p
Brochard'98 108 25.7 10.7 48.0% 31.7 10.7 41.0% ns Stewart'98 120 22.3 8.6 48.0% 26.8 7.2 46.0% ns Ranieri'99 44 24.6 14.8 38.0% 31.0 6.5 58.0% 0.19Brower'99 52 27.0 9.3 50.0% 30.0 8.2 46.0% nsAmato’98 53 31.8 16.3 38.0% 34.4 6.9 71.0% <0.001ARDSnet'00 861 25.0 9.4 31.0% 33.0 8.6 39.8% 0.007Kallet'05 292 27.5 10.0 32.0% 33.8 7.4 51.0% 0.004Villar’06 95 30.6 14.1 34.0% 32.6 9.0 55.5% 0.041 low PEEP high PEEPARDSnet'04 549 24.0 9.1 24.9% 27.0 14.7 27.5% nsMercat’08 767 21.1 8.4 39.0% 27.5 15.8 35.4% nsMeade’08 983 24.9 10.1 40.4% 30.2 15.6 36.4% ns
Sunday, April 25, 2010

clinical trials
Protective ControlAuthor n Ppl PEEP Mort Ppl PEEP Mort p
Brochard'98 108 25.7 10.7 48.0% 31.7 10.7 41.0% ns Stewart'98 120 22.3 8.6 48.0% 26.8 7.2 46.0% ns Ranieri'99 44 24.6 14.8 38.0% 31.0 6.5 58.0% 0.19Brower'99 52 27.0 9.3 50.0% 30.0 8.2 46.0% nsAmato’98 53 31.8 16.3 38.0% 34.4 6.9 71.0% <0.001ARDSnet'00 861 25.0 9.4 31.0% 33.0 8.6 39.8% 0.007Kallet'05 292 27.5 10.0 32.0% 33.8 7.4 51.0% 0.004Villar’06 95 30.6 14.1 34.0% 32.6 9.0 55.5% 0.041 low PEEP high PEEPARDSnet'04 549 24.0 9.1 24.9% 27.0 14.7 27.5% nsMercat’08 767 21.1 8.4 39.0% 27.5 15.8 35.4% nsMeade’08 983 24.9 10.1 40.4% 30.2 15.6 36.4% ns
P distensión = P meseta - PEEP
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

at risk…safe zone
driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

clinical data: low vs high PEEP
low PEEP high PEEP ( max recruitment)
Author n Ppl PEEP Mort Ppl PEEP Mort p
ARDSnet'04 549 24.0 9.1 25% 27.0 14.7 27% ns
Mercat’08 767 21.1 8.4 31% 27.4 15.8 27% ns
Meade’08 983 24.0 9.4 40% 27.0 13.5 36% ns
Sunday, April 25, 2010

at risk…safe zone
driving pressure (Pplateau - PEEP)
Sunday, April 25, 2010

Meade MO, et al. JAMA 2008
Mercat A, et al. JAMA 2008
Express study
LOV study
high (15-16) vs low (9-10) PEEP (1750 patients)
Sunday, April 25, 2010

Meade and Mercat study: 1750 patientslow PEEP
890high PEEP
860
severehypoxemia
184706
severehypoxemia
94 766
Gattinoni L, Caironi P. JAMA 2008; 299: 691-3.
20.7% 10.9%
Sunday, April 25, 2010

Meade and Mercat study: 1750 patientslow PEEP
890high PEEP
860
severehypoxemia
184706
severehypoxemia
94 766
Gattinoni L, Caironi P. JAMA 2008; 299: 691-3.
20.7% 10.9%
S: 77NS: 107
S: 459NS: 247
S: 37NS: 57
S: 514NS: 252
58.2% 60.6%35.0% 32.9%
Sunday, April 25, 2010

Meade and Mercat study: 1750 patientslow PEEP
890high PEEP
860
severehypoxemia
184706
severehypoxemia
94 766
Gattinoni L, Caironi P. JAMA 2008; 299: 691-3.
20.7% 10.9%
pulmonarydeath12.0%
non-pulmdeath27.8%
globalmortality39.8%
pulmonarydeath6.6%
non-pulmdeath29.3%
globalmortality35.9%
S: 77NS: 107
S: 459NS: 247
S: 37NS: 57
S: 514NS: 252
58.2% 60.6%35.0% 32.9%
Sunday, April 25, 2010

concept: VILI is at first mechanical
overdistentionopening-closing
release of mediators
↑ ventilatory requirements
increase in permeability
Pinhu L, et al. LANCET • Vol 361 • January 25, 2003Fan E, Needham DM, Stewart TE. JAMA 2005; 294: 2889-96.
• fem, 44 yo, pancreatitis• 6 days on MV before transferred• died
Sunday, April 25, 2010

concept: VILI is at first mechanical
overdistentionopening-closing
release of mediators
↑ ventilatory requirements
increase in permeability
Pinhu L, et al. LANCET • Vol 361 • January 25, 2003Fan E, Needham DM, Stewart TE. JAMA 2005; 294: 2889-96.
• fem, 44 yo, pancreatitis• 6 days on MV before transferred• died
biotrauma
barotrauma / volutrauma
atelectrauma
Sunday, April 25, 2010

concept: VILI is at first mechanical
overdistentionopening-closing
release of mediators
↑ ventilatory requirements
increase in permeability
Pinhu L, et al. LANCET • Vol 361 • January 25, 2003Fan E, Needham DM, Stewart TE. JAMA 2005; 294: 2889-96.
• fem, 44 yo, pancreatitis• 6 days on MV before transferred• died
biotrauma
barotrauma / volutrauma
atelectrauma
strain ⇒ Vt / EELV
Sunday, April 25, 2010

1667: Keeping a dog alive by blowing through its lungs with bellows
Hooke's law: the stress imposed on a solid is directly proportional to the strain produced, within the elastic limit
Sunday, April 25, 2010

qué tienen en común?
Sunday, April 25, 2010

su volumen corriente es 6 ml/kg…!!!
qué tienen en común?
Sunday, April 25, 2010

Tenney SM and Remmers JE. Nature 1963; 197: 54-56,
Sunday, April 25, 2010

falla respiratoria severa
en cualquiera estrategia, el punto más importante es limitar el volumen corriente a no
más de 6 ml/kg (peso ideal)
• frecuencias respiratorias rápidas 30-35 /min• modalidad ventilatoria no afecta• protocolos sedación y analgesia• protocolos reanimación y depleción• control infecciones
Sunday, April 25, 2010

ventiladores de 4ª generación
Sunday, April 25, 2010

classic modes of ventilation
output inputpatient physicianpatient
assistanceVt - RR - I:EFiO2 - PEEP
Sunday, April 25, 2010

classic modes of ventilation
output inputpatient physician
patient adapts to ventilator
patientassistance
Vt - RR - I:EFiO2 - PEEP
Sunday, April 25, 2010

close loop technology
output input
patientdemand
patientassistance
patient physicianinspiratory
supportFiO2 - PEEP
Sunday, April 25, 2010

hipoxemia permisiva
Grocott MP, et al. N Engl J Med 2009; 360: 140-9.
Sunday, April 25, 2010

Sunday, April 25, 2010

21% mortality rate!!!
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
PEEP IMV PS
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
PEEP IMV PS
CT-scan
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
pulmón rígido
PEEP IMV PS
CT-scan
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
pulmón rígido
babylung
PEEP IMV PS
CT-scan
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
pulmón rígido
babylung
PEEP IMV PS
CT-scan
daño inducido por la VM
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
pulmón rígido
babylung
PEEP IMV PS
CT-scan ARDSnetstudy
daño inducido por la VM
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
Sunday, April 25, 2010

historia VM
SDRA
iron lung
ventpresión
ventvolumen
ventiladoresmicroprocesados
VPP
pulmón rígido
babylung
PEEP IMV PS
CT-scan ARDSnetstudy
daño inducido por la VM
1950 1960 1970 1980 1990 2000 2010
ustedestá aquí
ventiladores4a generación
estrategia protectora
Sunday, April 25, 2010

objetivos de la VM... siglo XXI
• sostener la ventilación• reclutar alvéolos colapsados
– mejorar intercambio– ↓ trabajo ventilatorio
• evitar el daño inducido por la ventilación mecánica– limitar presión transpulmonar
Sunday, April 25, 2010

principles of protective ventilation
Sunday, April 25, 2010

principles of protective ventilation
• limit Vt– ↓ transpulmonary pressure– no magic number…
Sunday, April 25, 2010

principles of protective ventilation
• limit Vt– ↓ transpulmonary pressure– no magic number…
• optimize PEEP– optimize recruitment → mecánica, ↓Vd/Vt– no magic number…
Sunday, April 25, 2010

principles of protective ventilation
• limit Vt– ↓ transpulmonary pressure– no magic number…
• optimize PEEP– optimize recruitment → mecánica, ↓Vd/Vt– no magic number…
• analgesia based sedation– ↓ ventilatory drive
Sunday, April 25, 2010

principles of protective ventilation
• limit Vt– ↓ transpulmonary pressure– no magic number…
• optimize PEEP– optimize recruitment → mecánica, ↓Vd/Vt– no magic number…
• analgesia based sedation– ↓ ventilatory drive
try the lung gently
Sunday, April 25, 2010

Bundles: prevención NAV
• No realizar cambios en circuito ventilatorio a menos que esté específicamente indicado
• Higiene de manos estricto usando alcohol• Staff apropiadamente educado y entrenado• Incorporación de vacaciones de sedación y
protocolos de destete• Aseo oral con clorhexidina
A European care bundle for prevention of ventilator-associated pneumonia.Rello J. et al. Intensive Care Med 2009.
Sunday, April 25, 2010

Sunday, April 25, 2010

Sunday, April 25, 2010