Inhibidores de la CDK 4/6: Resultados y papel de la … · • Bind within the ATP-binding pocket...
35
Inhibidores de la CDK 4/6: Resultados y papel de la nueva diana terapéutica en el CM metastásico RE+/HER2- S López-Tarruella, MD, PhD
Transcript of Inhibidores de la CDK 4/6: Resultados y papel de la … · • Bind within the ATP-binding pocket...

Inhibidores de la CDK 4/6: Resultados y papel de la nueva
diana terapéutica en el CM metastásico RE+/HER2- S López-Tarruella, MD, PhD

a
b
c
d
Tumor Microenvironment
NR: ER: variants,
loss
ERβ
EER
AR
Coregulators
TKR/GF: EGFR/HER2
IGFR, FGFR,
VEGFR2
FGFR
Cellular Kinases: MEK/MAPK
PTEN/PI3K/Akt
P38/JNK
SRC/FAK
TF: AP1
SP1
NFkB
Stress
Responses: Treatments
Cytokines
Hypoxia
OS/ROS
Pathways: Cell Cycle (Cyclin D,
E) Survival (Bcl, BAD)
Proliferation (Myc)
F
T
AI
F AI
T +
Integrins
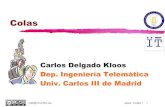
Osborne CK & Schiff R Ann Rev Med 2011, TCGA Nature 2012
ER SIGNALING &
ED_RESISTANCE
MECHANISMS

Killing 2nd messenger: targeting loss of cell cycle control
Lange & Yee End Relat Cancer 2011
Mitogenic signaling pathways
• Mitogenic or GFR signalling
pathways converge on the cyclin
D–CDK4 or CDK6–RB axis
• Activation of CDK4 or CDK6
RB phosphorylation
inactivation of Rb cell
progression from G1 to S…G2...M
(associated with resistance to ED
therapy)
Cell Cycle (Cyclin D1-CDK4/6 pathway)
RB “the master-regulator” of R-point
• Protein kinases control cell cycle
progression & depend on associating
regulatory subunits, cyclins

Cyclin Inhibitors Landscape
Malumbres & Barbacid. Nat Rev Cancer 2001, Asghar et al Nat Rev Drug Discov 2015
Sele
ctiv
ity
Agent Target
Alvociclib (flavopiridol) CDK 1/2/4/6/7/9
Seliciclib (Roscovitine) CDK 2/7/9
Dinaciclib (SCH 727965) CDK 1/2/5/9
SNS-032 CDK 1/2/4/9
Palbociclib (PD 0332991) CDK 4/6
Abemaciclib
(LY2835219)
CDK 4/6
Ribociclib (LEE 011) CDK 4/6
• 1G: pan-CDK inhibitors (relatively non-specific) (phase I/II)
• 2G: increasing selectivity for CDK1/2 and increasing overall potency (phase I/II)
Will improved selectivity for certain CDKs be the key to the successful development of
CDK inhibitors as therapeutic cancer agents? • CDK4/6 inhs: elicit cytostatic G0/G1 arrest & direct reflection of the engagement of RB to
suppress gene expression and proliferation
- lack of clear understanding of the mechanism of action
- lack of appropriate patient selection
- lack of a therapeutic window

Chemical structure of selective CDK4/6 inhibitors
O’Leary et al Nat Rev Clin Oncol 2016
• Orally-administered compounds are of similar structure
• Bind within the ATP-binding pocket of CDK4 and CDK6
• High degree of selectivity for CDK4 and CDK6, compared with CDK1 and CDK2
*

Preclinical PALBOCICLIB
• Identification of differentially expressed genes and sensitivity to PD 0332991: Rb and cyclin D1 expression and CDKN2A (p16) in sensitive cell lines
• PD 0332991 blocks Rb phosphorylation in sensitive cell lines
• PD 0332991 acts synergistically with TAM in inhibiting growth of ER-positive human BC cell lines
• PD 0332991 overcomes acquired resistance to tamoxifen: enhances the effects of TAM in an MCF7 tamoxifen-insensitive cell line
Finn et al Breast Cancer Res 2009
In vitro sensitivity to PD 0332991 across a panel of human BC cell lines

Early phases of PALBOCICLIB development
• First-in-human: Advanced solid tumors & NHL with intact Rb (N=33), 2wks
on/1wk off (2/1). DLTs: neutropenia & thrombocytopenia. RP2D 200 mg/d
• Phase 1: Rb-positive advanced solid tumors (N=41), 3wks on/1wk off
(3/1). DLT: neutropenia. RP2D 125 mg/d
Schwartz et al BJC 2011, Flaherty et al CCR 2012, DeMichele et al CCR 2015
Palbociclib Monotherapy
• 3wks on/1wk off (3/1) schedule
• N=37 (84% HR+, 5% HR+/HER2+, 11%
TN)
• CBR 19% (21% HR+ and 29% >2 prior
lines HT)
• Median PFS: 3.7 mo (longer in HR+ 4.5
mo & those progressed to HT 5 mo)
• Toxicity: neutropenia (51%),
thrombopenia (22%) and anemia (5%) – 24% treatment interruption
– 51% dose reduction
Phase II: Rb-positive advanced BC
HR+/HER2-

PALBO in 1L setting. PALOMA-1/TRIO 018
Finn et al SABCS 2009 (Abst 5069) and Finn et al Lancet Oncol 2015
PD 0332991 + Letrozole for 1L postM ER+/HER2- MBC (fase Ib/II)
• Phase 1 part (N=12): Palbo 125 mg/d (3/1 schedule)+Letrozole 2.5 mg/d (no DDI)
• AEs: neutropenia, leukopenia and fatigue
PD 0332991 125 mg QD 3/1 + Letrozole 2.5 mg QDx 4wk
Letrozole 2.5 mg QDx 4wk
Postmenopausal women
with ER-positive, HER2-negative
advanced BC (N= 66)
Stratified by disease site (visceral, bone only, or other); Disease-Free Interval (>12 vs ≤12 mo from
end of adjuvant to recurrence or de novo advanced disease)
Postmenopausal women
with ER-positive, HER2-negative advanced bc &
CCND1 amp, and/or p16 loss
(N= 99)
Part 1 Part 2
*All patients continued assigned treatment until disease progression, withdrawal of consent, or unacceptable toxicity with follow-up tumor assessment every 2 mo & accrual to cohort 2 stopped after interim analysis of cohort 1 amending statistical plan to combine both cohorts
Stratified by disease site (visceral, bone only, or other); Disease-Free Interval (>12 vs ≤12 mo from end
of adjuvant to recurrence or de novo advanced disease)
Exploratory study evaluating safety and efficacy of the combination in patients
selected based on HR status only
PD 0332991 125 mg QD 3/1 + Letrozole 2.5 mg QDx 4wk
Letrozole 2.5 mg QDx 4wk
1:1 1:1
• Primary Endpoint: PFS inv • Designed to detect a 50% improvement in median
PFS from 9 to 13.5 months (80% power, 1-sided α = 10%)
• Open label, randomized phase II study (2 cohorts sequentially enrolled)
• Postmen. ABC (1L)
• No prior AI or stopped adjuvant AI
at least 1 yr before relapse
• Measurable by RECIST or bone-only
disease

PALBO in 1L setting. PALOMA-1/TRIO 018
Finn et al Lancet Oncol 2015
N=165

PALBO in 1L setting. PALOMA-1/TRIO 018
Finn et al Lancet Oncol 2015
Median PFS 20.2 vs 10.2mo
HR 0.499*
Median PFS 26.1 vs 5.7mo
Median PFS 18.1 vs 11.1mo
• Response: ORR 36 vs 27% and CBR 68 vs 47% and DoR 20.3 vs 11.1mo
• OS (median FU 27.9 vs 29.6mo): 37.5 vs 33.3 mo (HR 0.81 NS)
• AEs: neutropenia, leucopenia and fatigue >> anemia, nausea, arthralgia, alopecia
• Dose interruptions bc AEs: 33% vs 4%
• 45% dose delay and 40% dose reduction (mean relative dose-intensity 94%)
• FDA grants breakthrough therapy
designation for Palbociclib in BC (11/APR/13)
• FDA grants accelerated approval (3/FEB/15)
in combination with LET for the treatment of postM ER+HER2-
advanced BC as initial endocrine-based therapy for MBC

PALBO in 1L setting. PALOMA-2/TRIO 22
Finn et al ASCO 2016 (Abst 507)
• Median FU: 23 mo Palbo/LET and 22.3mo Pbo/LET

PALBO in 1L ABC: PALOMA-2/TRIO 22
Finn et al ASCO 2016 (Abst 507)

PALBO in 1L ABC. PALOMA-2/TRIO 22: efficacy
• Palbo/LET significantly improved median PFS vs Pbo/LET as 1L therapy in women with
ER+/HER2– advanced BC
- A >10 month improvement in median PFS was observed (24.8 vs 14.5 mo) HR =
0.58 (95% CI, 0.46–0.72; P<0.0001)
• Benefit from palbociclib demonstrated across prespecified subgroups and confirmed
by blinded independent review
Finn et al ASCO 2016 (Abst 507)

PALBO in 1L ABC. PALOMA-2/TRIO 22: safety
Finn et al ASCO 2016 (Abst 507)
• Overall incidence of SAEs higher in Palbo/LET 19.6% vs 12.6% in Pbo/LET arm • 9.7% pts in Palbo/LET vs 5.9% Pbo/LET permanently discontinue due to AEs • 2.3% vs 1.8% death due to AEs in both arms none due to treatment-related toxicity

PALBO after endocrine failure: PALOMA-3
Turner et al ASCO 2015

PALBO after endocrine failure. PALOMA-3: efficacy
• Response: ORR 10.4 vs 6.3% (NS) and CBR 34 vs19%*
• OS (median FU 5.6 mo) still inmature
* Update 8.9 mo FU (median PFS 9.5 vs 4.6 mo HR 0.46*) benefit in ORR and CBR confirmed (although it can take months to achieve)
• Median age (57 vs 56 yr): 21%
pre/periM
• 60% visceral metastasis & 29% 2
disease sites
• 79% documented sensitivity to
prior HT (relapsed after 24 mo of
adjuvant HT or clinical benefit to prior HT
in ABC)
• 86% prior AI and 60% prior TAM
+/- GnRH
Turner et al NEJM 2015, Cristofanilli et al Lancet Oncol 2016

17
PALBO after endocrine failure. PALOMA-3: efficacy
Turner et al NEJM 2015

• Overall incidence of SAEs was similar (9.6% vs 14.0%)
• Discontinuations due to AEs 2.6 vs 1.7%
• Incidence of febrile neutropenia was the same (0.6% vs 0.6%)
– Neutropenia most common AE leading dose reductions 21%
• Infections (any grade) were more common (34.2% vs 24.4%) mainly G1/2
Turner et al NEJM 2015
• FDA grants breakthrough therapy designation for Palbociclib in BC (11/APR/13)
• FDA grants accelerated approval (3/FEB/15)
in combination with LET for the treatment of postM ER+HER2- advanced BC as initial
endocrine-based therapy for MBC
• FDA grants regular approval (19/FEB/16)
in combination with FULV for the treatment of postM ER+HER2-
advanced or metastatic BC with disease progression following
endocrine therapy
PALBO after endocrine failure. PALOMA-3: safety

PALBOCICLIB ongoing phase III trials in ER+ BC
Finn et al BCR 2016
Trial Phase
(N)
Design Population Primary
Endpoint
PEARL
GEICAM 2013-02
III
(348*)
Palbo+EXE &
Palbo/FUL* vs
Capecitabine
with resistance to
NSAIs MBC postM
PFS
FLIPPER
GEICAM 2014-12
II
(190)
Palbo+FUL vs
Pbo+FUL
1L MBC postM
(after 5yr HT
>12mo DFS or
CMM de novo)
PFS
PENELOPE-B
GBG78/BIG1-13/NSABP-
B64
III
(800)
Palbo+ED vs
Pbo+ED
after NACT with
residual disease
(High Risk EBC)
pre/postM
iDFS
PALLAS
AFT-05, ABCSG 42, BIG 14-
03, 2014-005181-30
III (4600) Palbo (2yrs)+HT (>5yrs)
vs HT (>5yrs)
Stage II-III
pre/postM.
iDFS
NeoPAL
UC-0140/1404, 2014-
002560-33, CARMINA04
II
(132)
Palbo+LET vs FEC-3 –
Docex3
NA. Stage II-
IIIA.PostM. PAM50=
ROR
low/intermediate
RCB
PALLET
NSABP FB-11, WI180455
II
(306)
Palbo+LET vs LET vs
LET-LET/Palbo vs
Palbo-LET/Palbo
NA. T>2 cm. PostM Biomarker
cCR and Ki
67 change

Early phases of RIBOCICLIB development
20
• Specifically inhibits CDK4 and 6 in tumors with
full functional pRb (intact total pRb by IHC)
• Phase I recommended dose 600 mg/d 21-of-28
day dosing schedule
• Most common AE (G3/4): neutropenia (19%),
leukopenia (12%) and lymphopenia (14%)
Infante et al ASCO 2014 & O'Brien et al AACR 2014, Asghar et al Nat Rev Drug Discov 2015, Juric er al ASCO 2016
• 47 pts (dose escalation and dose expansion) had been treated with
Ribo 600 mg QD (3-weeks-on/1-week-off) + LET 2.5 mg QD
90% in dose escalation were
previously treated for aBC
96% in dose expansion treatment-naïve for aBC
46% ORR
79% CBR

RIBOCICLIB ongoing trials in BC
Trial Phase
(N)
Design Population Primary
Endpoint
MONALEESA-1 II
(120)
LEE011+LET (400 mg or 600
mg) vs LET
NA (resectable
BC)
Cell-cycle
RR (Ki 67)
MONALEESA-2
NCT01958021
III
(650)
LEE011600 mg+LET vs Pbo+LET 1L MBC postM PFS
MONALEESA-3
NCT02422615
III
(660)
LEE011600 mg+FUL
vs Pbo+FUL
>1L MBC postM PFS
MONALEESA-7
NCT02278180
III
(660)
LEE011600
mg+TAM/IA+goserelin vs
Pbo+TAM/IA+goserelin
1L MBC preM PFS
Finn et al BCR 2016

Is there a role for a triple HT+ CDK4/6 and PI3K
inhibitor combination ?
O’Leary et al NRCO 2016, Herrera-Abreu et al Cancer Res 2016, Hamilton et al Cancer Treat Rev 2016
• ER+ BC cells can adapt to CDK4/6 inhibition and evade cytostasis in part via non-
canonical cyclinD1-CDK2-mediated S-phase entry prevented by co-treatment
with PI3K inhs • PI3K inhs failed to re-sensistize cells once resistance is acquired (CDK2 inh role?)
Trial Phase Design
NCT02088684 Ib/II
(216)
Ribociclib+Buparlisib+FUL
Ribociclib+Alpelisib+FUL
Ribociclib+FUL
NCT01872260
Juric et al SABCS
2015
Ib/II
(200)
Ribociclib+Alpelisib+LET
* RP2D for the triplet ribociclib 300 mg/day (3-weeks-on/1-
week-off) + alpelisib 200 mg/day (continuous) + letrozole 2.5
mg/day (continuous)
NCT01857193
Bardia et al
SABCS 2015
Ib
(142)
Ribociblib+EVE+EXE
* RP2D for the triplet 300 mg/day ribociclib (3-weeks-on/1-
week-off) + 2.5 mg/day EVE (continuous) + 25 mg/day EXE
(continuous) with food

Early phases of ABEMACICLIB
development • Specifically inhibits CDK4 (more potent in vitro) and 6
but also reduces CDK9 activity
• Recommended dose 200 milligrams mg LY2835219 given
orally once every 12 hours in 28 day cycles (continuous
dosing)
• Crosses the blood brain barrier (JPBO phase II study)
Infante et al AACR 2012 & Patnaik et al Cancer Discov 2016 & Tolaney et al ASCO 2015, Sahebjan et al ASCO 2016
Phase I dose escalation followed by a tumor-specific cohort trial
• N=225 (33 in dose
escalation and 192
tumor-specific)
• DLT: G3 fatigue
• MTD 200 mg Q12h
• Dose reductions:
• 21% @150mgq12h
• 43% @200mgq12h

Early phases of ABEMACICLIB
development
ER+HER2-hBC xenograft (T47D)
Patnaik et al Cancer Discov 2016
ER+HER2+ responders
• Overall BC (N=47):
ORR 23% and CBR 49% and disease CR 70%
Median DoR 13.4 mo
Median PFS 5.8 mo
• HR+ BC (N=36):
ORR 31% & CBR 61.1% and DCR 81%
Median DoR 13.4 mo
Median PFS 8.8 mo
• MBC cohort (N=47) mixed
intrinsic subtypes
• Median 7 prior regimens
(highly pre-treated)
• 77% visceral involvement
*Non-responding breast tumors were more likely to harbor
TP53 mutations, all in the region encoding the p53 DNA-binding
domain
Phase I Breast Cancer cohort

ABEMA in HR+/HER2- pretreated: MONARCH-1
Dickler et al ASCO 2016 (Abst 510)
Characteristics of the population

ABEMA in HR+/HER2- pretreated: MONARCH-1: efficacy
Dickler et al ASCO 2016 (Abst 510)

ABEMA in HR+/HER2- pretreated: MONARCH-1: safety
Dickler et al ASCO 2016 (Abst 510)
• Overall incidence of SAEs 24.2% • 7.6% of patients permanently discontinue due to AEs • 2.3% death due to AEs

ABEMACICLIB ongoing trials
Trial Phase
(N)
Design Population Primary
Endpoint
MONARCH 1
NCT02102490 II
(128)
LY2835219 200mg/12hx28d MBC ORR
MONARCH 2
NCT02107703 III
(630)
LY2835219150mg/12h+FULvs
Pbo+FUL MBC PFS
MONARCH 3
NCT02246621 III
(450)
LY2835219150mg/12h+NSAIs vs
Pbo+NSAIS MBC
PFS
neoMONARCH
NCT02441946 II
(220)
LY2835219150mg/12h+ANA vs ANA vs
LY2835219150mg/12h
LY2835219150mg/12h+ANA
NA early
BC
Changes in
Ki 67
• Abemaciclib demonstrates single agent activity in heavily pre-treated pts
with HR+/HER2-MBC (ORR 19.7%, DoR 8.9 mo, CBR 42.4% and median PFS 6
mo OS 17.7 mo)
Dickler et al ASCO 2016 (Abst 510)
• FDA grants breakthrough therapy designation
for Abemaciclib in BC (8/OCT/2015)

HR+ BC most promising agents & TOXICITY
Rugo et al ASCO Educational book 2016

CDK4/6 inhibition and BIOMARKERS
• A number of biologically plausible biomarkers of sensitivity to CDK4/6
inhibition are available, for example cyclin D, CDKN2A and/or RB1 status;
however, ER-positivity in BC is the only selection marker currently
confirmed for use in the clinical setting
O’Leary et al NRCO 2016

CDK4/6 inhibition and BIOMARKERS
• PALOMA-1: ER+ in BC (very dependent on cyclin D1 and CDK4/6 to drive
proliferation) and cyclin D1 amp and/or p16 loss NOT correlated with
palbo benefit
• PALOMA-3: palbo benefit NOT related to degree of endocrine sensitivity
(clinically assessed previous endocrine response), pathologically assessed
(levels of ER/PR expression) or PI3K mut status (cfDNA exon 9 and 20
muts BEAMing tech)
O’Leary et al NRCO 2016, Cristofanilli et al Lancet Oncol 2016
PIK3CA wt PIK3CA mut

CDK4/6 inhibition and BIOMARKERS
• PALOMA-3: ESR1 muts were detected in 27% of baseline cfDNA and were
strongly associated with acquired resistance to prior AIs & palbo offers
high efficacy regardless of ESR1 mut status.
Turner et al ASCO 2016 (Abst 512)

Post-Menopausal Pre-Menopausal
• Patient: age, menopausal status, comorbidities, PS, expectations and
preferences, toxicities to previous treatments, adherence and compliance
• Tumor: histological subtype, HR expression, HER2 amp, intrinsic subtype,
predictive biomarkers*
• Disease: site of metastasis, tumor burden, symptoms/need rapid response,
previous HT, DFI on adjuvant setting, response to previous HT, DoR to
previous HT
• Agent: mechanism of action, expected toxicities, pharmacological
interactions, availability, cost, route of administration
• Availability of clinical research, existing guidelines, financial issues, social
support
Rugo et al JCO 2016, Reinert et al Ther Adv Med Oncoll 2015

CONCLUSIONES
Explosión actual de datos sobre la eficacia de Inhs CDK4/6 en CMM:
• Palbociclib es “first in class” queda apoyado por los datos del fase II (PALOMA1) y dos
fase III (PALOMA 2&3) con beneficio en términos de SLP (FDA breakthrough
designation regular approval)
• Ribocliclib acaba de anunciar datos positivos en su fase III en combinación con LET
en SLP (MONALEESA2) y abre la posibilidad de triples combinaciones con inhs PI3K
• Abemaciclib aporta datos en monoterapia de tasa de respuestas aprox 20% (fase II
MONARCH1) con un perfil de toxicidad algo diferente al resto (diarrea vs
neutropenia)
El descubrimiento y validación de BIOMARCADORES de respuesta para la
combinación de Inhs CDK4/6 & HT representa un reto, la re-biopsia de
lesiones metastásicas o la biopsia líquida son herramientas que pueden
ayudarnos a caracterizar molecularmente la dinámica de la enfermedad en
cada paciente y avanzar en la individualización del tratamiento (value in
cancer care context)
El panorama de la terapia hormonal para el CMM está cambiando
rápidamente y es preciso integrar los resultados de los estudios con el
balance riesgo/beneficio individual de cada alternativa para ofrecer el
mejor tratamiento a nuestras pacientes