MANEJO DE LA NEUTROPENIA FEBRIL EN EL … a hematooncologia. Dr... · Utilitat de la Procalcitonina...
38
Utilitat de la Procalcitonina en el maneig de la neutropènia febril postquimioteràpia Francesc Ferrés Serrat Cap de secció d’Urgències Pediàtriques Hospital Son Espases, Palma de Mallorca
Transcript of MANEJO DE LA NEUTROPENIA FEBRIL EN EL … a hematooncologia. Dr... · Utilitat de la Procalcitonina...
Utilitat de la Procalcitonina en el
maneig de la neutropènia febril
postquimioteràpia
Francesc Ferrés Serrat
Cap de secció d’Urgències Pediàtriques
Hospital Son Espases, Palma de Mallorca
Introducció (1)
Els pacients oncohematològics que reben quimioteràpia presenten en algun moment neutropènia i febre
Les causes més greus són les bacterièmies, especialment si són gèrmens multirresistents
Taxes elevades de morbimortalitat
La INFECCIÓ és la principal causa de mort no relacionada amb l’evolució de la malaltia en els pacients oncològics
Neutropènia febril: URGÈNCIA MÈDICA
Introducció (2)
Aquests pacients no presenten els símptomes usuals d’infecció localitzada i sistèmica
La febre pot ésser l’únic indicador de l’inici d’una infecció greu
Un percentatge significatiu d’aquests pacients es recuperen satisfactòriament sense que es trobi un focus infecciós aparent o es documenta només una infecció vírica
Introducció (3)
Tots els pacients amb neutropènia febril (NF) reben tractament antibiótic d’ampli espectre i generalment ingressen
Les estratègies de tractament precoç de la febre relacionada amb la neutropènia han millorat la supervivència
Però de vegades poden rebre tractaments antibiòtics inadequats, de duració excessiva i poden estar hospitalitzats més temps del necessari
Introducció (4)
Això comporta:
◦ Un impacte en l'ecologia microbiològica del pacient i de l’hospital
◦ Un augment de les resistències bacterianes
◦ Un augment de sobreinfeccions intercurrents
◦ Una disminució de la qualitat de vida del pacient i de la seva família
Introducció (5)
Recerca de dades clíniques i de laboratori que permetin estratificar el risc d’infecció greu, classificant la NF como d’Alt o Baix risc, amb l'objectiu de:
◦ Detectar precoçment les infeccions més greus de cara a la estratègia terapèutica
◦ Identificar adequadament les NF de Baix risc de cara a plantejar-se un maneig ambulatori i/o reduir els temps d’hospitalització
Introducció (6)
És coneguda la producció selectiva de PCT en infeccions bacterianes i potencialment greus en el pacient inmunocompetent
Hi ha una alteració en la producció de PCT en pacients oncològics amb neutropènia:
◦ Neutròfils productors de PCT
◦ Dany hepàtic secundari a la Quimioteràpia
No es coneix bé el valor de la PCT en la predicció i monitorització de la infecció greu en el pacient oncològic sotmès a quimioteràpia
Introducció (7)
Interès en la recerca de factors validats de l’alt o baix risc de les NF i específicament de la contribució dels biomarcadors d’infecció, principalment PCR i PCT, en l'estratificació del risc d'infecció greu i en la monitorització de l’evolució d’aquests pacients
Causes de febre en el pacient
oncològic (1)
Causes infeccioses: ◦ Víriques
◦ Bacterianes
◦ Fúngiques
◦ Parasitàries
Causes no infeccioses: ◦ Reaccions transfusionals
◦ Administració de fàrmacs antitumorals (Ara C)
◦ Febre d’origen tumoral
◦ Leucopènia severa
Causes de febre en el pacient
oncològic (2) IDM: Infecció Documentada Microbiològicament
IDC: Infecció Documentada Clínicament
FSF/FOD: FSF inicial i FSF després de 3 dies amb resultats microbiològics negatius i sense evidència clínica de l’origen de la febre:
◦ Causes no infeccioses
◦ Infeccions víriques no documentades
Edat > 12 anys
Infecció nosocomial
Recaiguda malaltia
Transplantament al·logènic de PH
Quimioteràpia < 7 dies
Hospitalització < 7 dies
Neutropènia > 7 dies
Comorbiditat
Leucèmia mieloide aguda
Afectació estat general
Febre > 39ºC
Calfreds
Hipotensió
Mucositis
Infiltrat pneumònic
Neutròfils < 100/mm3
Monòcits < 100/mm3
Plaquetes < 50000
PCR > 9 mg/dl
Necessitat d'expansió amb líquids IV
Criteris d’alt risc
de infecció greu
Què li demanem a un biomarcador ?
Que ens ajudi a estratificar el baix o alt risc d’una NF
Que ens orienti a decidir iniciar o no Tr antibiòtic en la NF
Que ens orienti en el Tr antibiòtic a administrar
Que ens orienti en la duració del Tr antibiòtic hospitalari
Que ens orienti en l’estratègia diagnòstica en pacients amb febre persistent
Que ens orienti en l’evolució clínica del pacient
Semeraro 2010 (1)
Fins al 60% de les NF son FOD
Objectiu: Valor de PCT en predir evolució de les FOD
FOD evolució favorable: si dia 3 afebril amb 1ª o 2ª línia de tr ATB empíric i si apirèxia persisteix durant la neutropènia o fins el dia 7 de tr ATB
FOD evolució desfavorable: si febre persisteix o reapareix el dia 3 o posterior o si acaba en IDM o IDC
72 episodis, 49 pacients. Tumors Sòlids i Linfomes
PCT cut-off de 0.12ug/L:
◦ Sen 80%, Esp 64% i VPN 82%
Conclou: ◦ Pacients amb una PCT < 0.12 es podrien beneficiar
d’un maneig ambulatori a partir de les 48 hores
◦ Que el 18% d’evolucions desfavorables possibles obliguen a una estreta vigilància clínica.
◦ Que s’han de buscar altres biomarcadors que juntament amb la PCT puguin predir millor l’evolució
Semeraro 2010 (1)
Martínez 2009 (1)
Objectiu: Avaluar valor de PCT i PCR a l’ingrés en identificar evolucions d’alt risc en NF
54 episodis/pacients, 29 LA
Descripció d’Alt Risc (18, 33.3%): 1 o més de:
◦ Signes clínics de sèpsia greu o shock sèptic
◦ Cultius positius de sang o orina
◦ Inici febre < de 7 dies de la darrera Quimioteràpia
4 èxitus (7.4%)
Martínez 2009 (2)
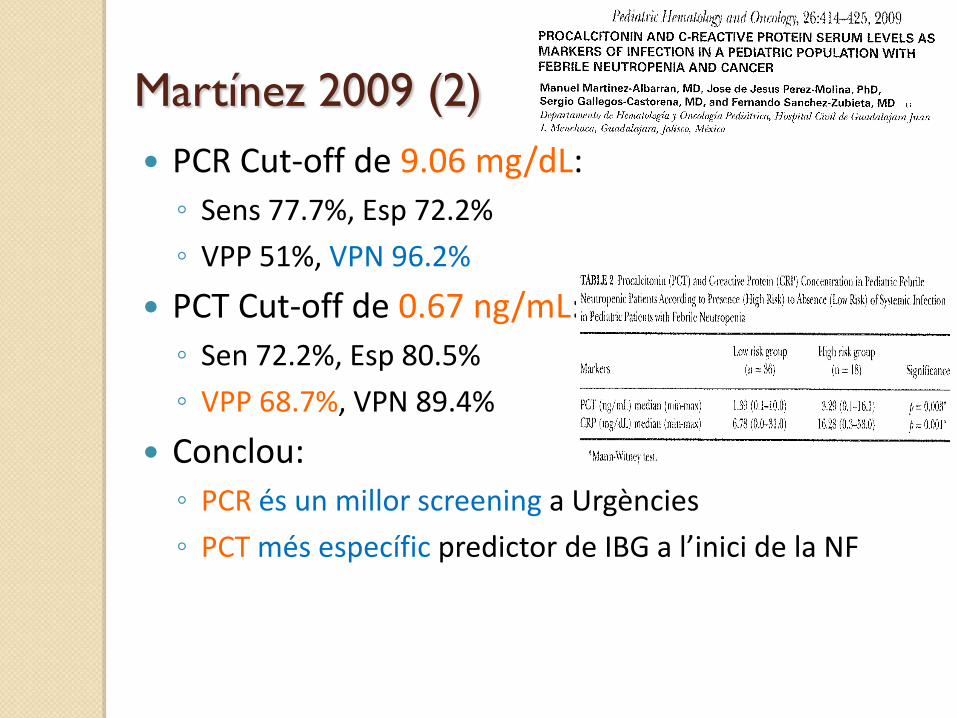
PCR Cut-off de 9.06 mg/dL:
◦ Sens 77.7%, Esp 72.2%
◦ VPP 51%, VPN 96.2%
PCT Cut-off de 0.67 ng/mL:
◦ Sen 72.2%, Esp 80.5%
◦ VPP 68.7%, VPN 89.4%
Conclou:
◦ PCR és un millor screening a Urgències
◦ PCT més específic predictor de IBG a l’inici de la NF
Fleischhack 2000 (1) Objectiu: valor de la PCT en l’avaluació del NF:
◦ Predir la bacterièmia, especialment en BGN
◦ Monitorització del procés febril
376 episodis, 120 pacients (210 L, 166 TS):
◦ 208 FOD (55%)
◦ 125 IDM
◦ 43 IDC
Fleischhack 2000 (2)
A l’ingrés, Cut-off per predir bacterièmia x BGN:
◦ PCT 0.5 ug/L, Sens 60%, Esp 85%
◦ PCT > 5 mg/dl, Sens 40%, Esp 99%
A l’ingrés i durant l’hospitalització:
◦ Els valors més alts de PCT s’associen a bacterièmia x BGN i x GP.
◦ 3 pacients críticament greus x bacterièmia x BGN tenien pic PCT> 100 ug/L (1 EXITUS)
◦ 1 pacient amb fungèmia: pic PCT de 25.8 ug/L (EXITUS)
Fleischhack 2000 (3)
Durant tota l’hospitalització:
◦ La disminució de PCT s'associa a:
Desaparició de la febre
Milloria clínica i/o resposta al tractament antibiòtic
◦ Els increments de PCT acompanyen:
Complicacions sèptiques
Infeccions fúngiques sistèmiques (sobretot després del 3er dia)
◦ Una PCT persistentment elevada:
Representa una infecció activa, encara que estigui controlada
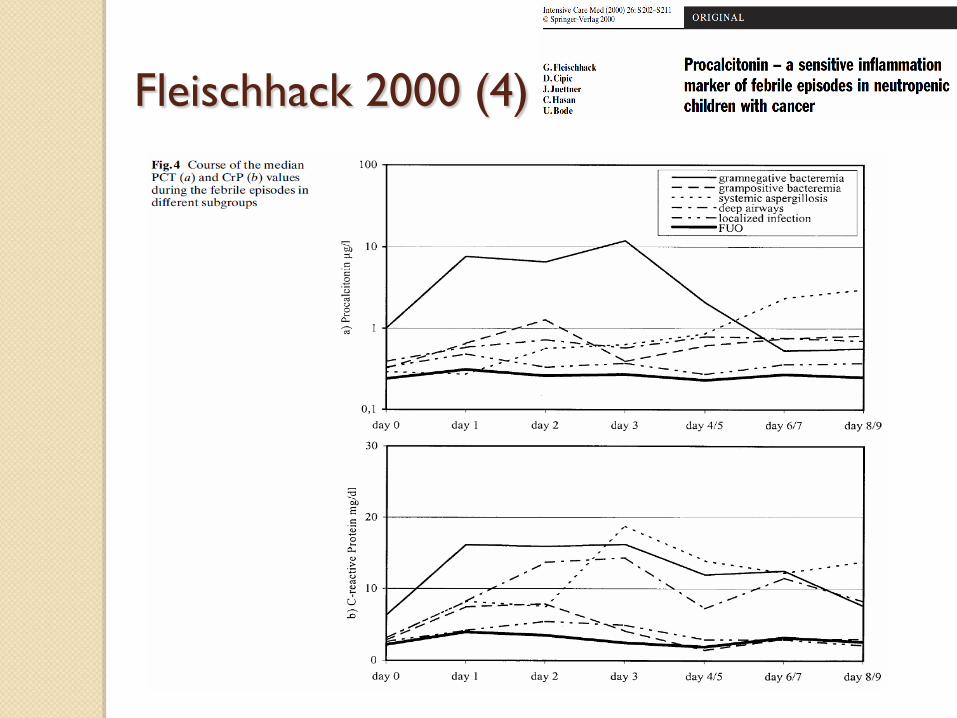
Fleischhack 2000 (4)
Fleischhack 2000 (5)
Conclouen:
◦ PCT és el marcador biològic més útil en NF
◦ Mesures seriades de PCT en NF són útils per:
Predir IBG
Avaluar resposta al tractament antibiòtic
Detecció precoç de complicacions
Monitoritzar pacients críticament malalts
Reitman 2012 (1)
Objectiu: Avaluar els valors seriats de PCT com a predictors de bacterièmia
PCT a l’ingrés i a les 12-24 hores
89 NF
18 hemocultius positius
◦ 6 GP
◦ 12 GN
Clinical Pediatrics
51(12) 1175 –1183
© The Author(s) 2012
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0009922812460913
http://cpj.sagepub.com
Introduction
This article reports on a small-to-medium sized, prospec-
tive, single-center study on the prediction of bacteremia
by serial procalcitonin (PCT) measurements in children
with fever and chemotherapy-induced neutropenia.
Patients undergoing chemotherapy for cancer will have
periods of neutropenia, and during these times, febrile
patients are at a higher risk for developing bacteremia.1
Over the past 3 decades, clinicians have attempted to
identify children with fever and neutropenia to be at
either high or low risk for a serious bacterial infection.
The hopes of risk classification were to decrease the rate
of hospital admissions, to prevent the emergence of anti-
microbial resistance,2 to avoid in-hospital complica-
tions, and to decrease the impairment of quality of life to
patients and their families. Oncologists have categorized
high- and low-risk adult patients for the development of
bacteremia, but their recommendations have been lim-
ited.3-6 Similarly, high- and low-risk classification stud-
ies have been evaluated in pediatric patients. Even
though there have been retrospective,7-14 prospec-
tive,15-19 and validation studies20 for high- and low-risk
patients, the majority of the pediatric oncologists have
been slow to adapt risk classifications for serious bacte-
rial infections in this high-risk population.
Regardless of risk, pediatric patients undergoing che-
motherapy continue to be routinely hospitalized for
fever and neutropenia. The current treatment consensus
for fever and neutropenia in pediatric patients has been
hospital admission, initiation of broad-spectrum antibi-
otics, and maintenance until the blood culture results are
negative for bacterial growth.21 Kara et al22 showed that
pediatric blood cultures may not produce growth for the
first 48 hours. Their study had bacterial growth in 54%
of children by day 3, 77% by day 4, and 89% by day 5.22
Furthermore, even when the clinical picture depicts a
patient who is septic, the blood culture may not produce
bacterial growth.23 Several studies have shown this to be
evident in pediatric patients because the blood volume
obtained is inadequate for bacterial growth.22,24,25 On the
contrary, blood cultures are widely known to have false
positives. Although blood cultures are not perfect, it is
still the gold standard for detecting bacteremia.
460913CPJ XXX10.1 177/0009922812460913 Clinical PediatricsReitman et al
1University of California, San Francisco-Fresno, Fresno, CA, USA2Children’s Hospital Central California, Madera, CA, USA
Corresponding Author:
Aaron J. Reitman, Children’s Hospital Los Angeles, 4650 Sunset Blvd,
Los Angeles, CA 90027
Email: [email protected]
Serial Procalcitonin Levels to Detect
Bacteremia in Febrile Neutropenia
Aaron J. Reitman, DO1,2, Rhonda M. Pisk, MS2, John V. Gates III, MD1,2, and J. Daniel Ozeran, MD, PhD1,2
Abstract
Background. Our objective was to evaluate serial procalcitonin (PCT) levels compared with an initial PCT level at
admission in predicting bacteremia in pediatric febrile neutropenic oncology patients. Procedure. Serum PCT levels
were measured at admission (t0) and within 24 hours of admission (t1) in pediatric oncology patients presenting
with fever and neutropenia. A blood culture was collected at t0 and monitored for 5 days for bacterial growth. PCT
value of 0.5 ng/mL at either t0 or t1 was considered predictive for bacteremia. Results. PCT levels were significantly
higher in children with positive blood cultures than with negative blood cultures. Serial PCT values mirrored t1
values. Serial PCT showed 76% specificity and negative predictive value of 93% in ruling out bacteremia. Conclusion.
Elevated PCT levels are predictive of bacteremia. Using serial PCT levels within 24 hours allowed a better prediction
of bacteremia than the PCT level at t0.
Keywords
procalcitonin, febrile, neutropenia, oncology, pediatric
Reitman 2012 (2) 1178 Clinical Pediatrics 51(12)
ruling out bacteremia. Using the ROC curve analysis,
the area under the curve (AUC) was determined at t0, t1,
and serial draws (0.77, 0.88, and 0.88, respectively;
Figure 2). The AUC of 0.88 indicates serial PCT draws
to be a better biomarker than a single PCT draw for bac-
teremia in this population.
The prevalence of bacteremia in the study population
was 20% or 1 in 5 patients. Using the positive likelihood
ratio, there is an 85% probability that the patients found
to have a positive serial PCT result will have bactere-
mia. Likewise, the negative likelihood ratios can be
used to determine that a patient with a negative serial
PCT level has less than a 1% chance of having bactere-
mia. These results again suggest that PCT is a useful
diagnostic test in this patient population (Table 3).
In the attempt to establish the optimal PCT cutoff
value to be used in our specific population, the diagnos-
tic sensitivity and specificity of PCT were explored using
the ROC results. The best combination of sensitivity and
specificity in this population was achieved at a cutoff
value of 0.4 ng/mL at both t0 and t1 time points.
Discussion
Children undergoing chemotherapy for cancer will most
certainly have episodes with fever and neutropenia dur-
ing treatment. This association occurs with greater fre-
quency with the growing intensity of chemotherapy.
The rapid progression of bacterial infections in neutro-
penic pediatric patients to sepsis is one reason why
these patients are frequently admitted to the hospital
and broad-spectrum antibiotics are initiated.
The precise volume of blood needed to adequately
detect bacteremia in children has not been established as
in adults.24,43,44 Blood cultures may not yield bacterial
growth for several days. Nonetheless, blood cultures are
still considered the gold standard for the detection of
bacteremia. The presence of a reliable sepsis marker
could assist in clinical decision making.
In children presenting with fever and neutropenia,
PCT has been shown to be a useful biomarker in detect-
ing serious bacterial infections.19,27-30,35-39 This study
confirms the results from previous studies as well as
demonstrates the importance of serial PCT levels in the
detection of bacteremia. This study showed serial PCT
draws to be better at detecting bacteremia than a single
PCT level, with the average increase in sensitivity
Figure 1. Patient flow diagram
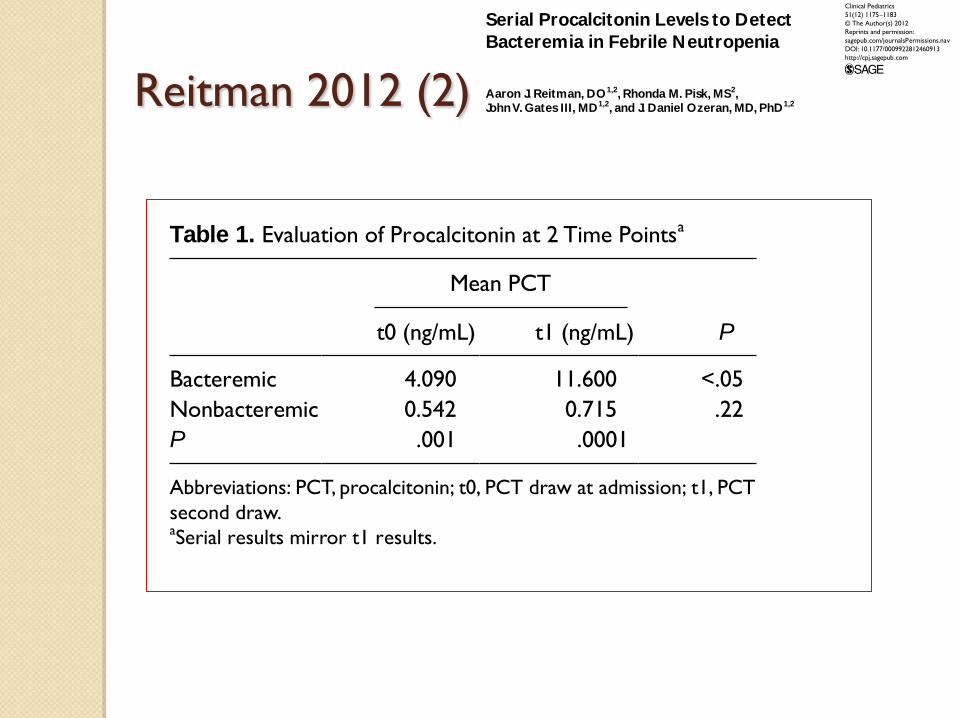
Table 1. Evaluation of Procalcitonin at 2 Time Pointsa
Mean PCT
t0 (ng/mL) t1 (ng/mL) P
Bacteremic 4.090 11.600 <.05
Nonbacteremic 0.542 0.715 .22
P .001 .0001
Abbreviations: PCT, procalcitonin; t0, PCT draw at admission; t1, PCT
second draw.aSerial results mirror t1 results.
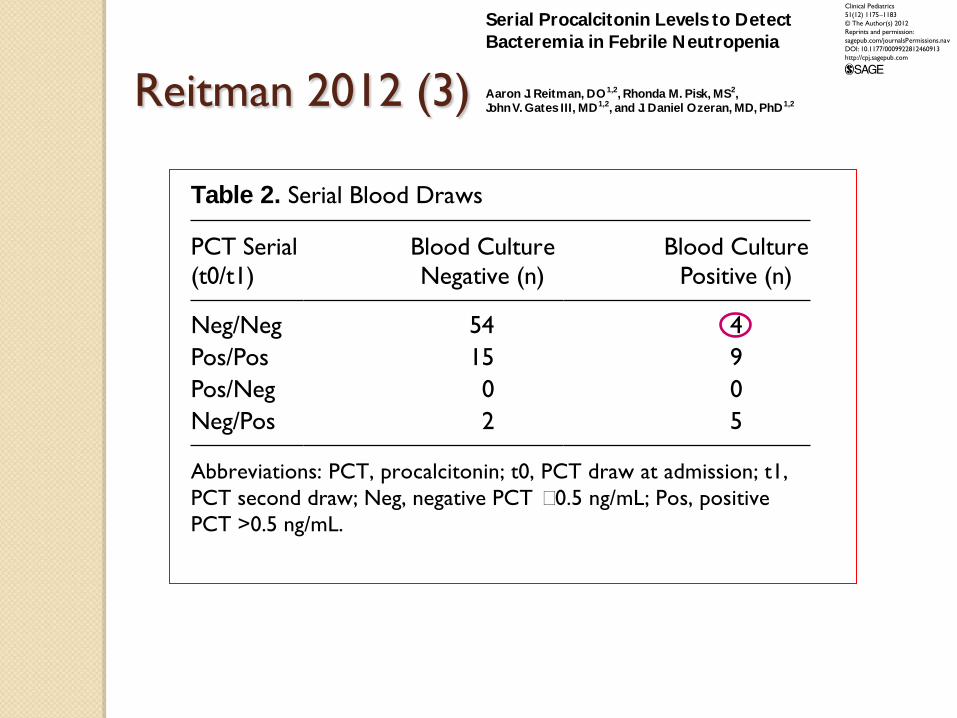
Table 2. Serial Blood Draws
PCT Serial
(t0/t1)
Blood Culture
Negative (n)
Blood Culture
Positive (n)
Neg/Neg 54 4
Pos/Pos 15 9
Pos/Neg 0 0
Neg/Pos 2 5
Abbreviations: PCT, procalcitonin; t0, PCT draw at admission; t1,
PCT second draw; Neg, negative PCT ≤0.5 ng/mL; Pos, positive
PCT >0.5 ng/mL.
Clinical Pediatrics
51(12) 1175 –1183
© The Author(s) 2012
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0009922812460913
http://cpj.sagepub.com
Introduction
This article reports on a small-to-medium sized, prospec-
tive, single-center study on the prediction of bacteremia
by serial procalcitonin (PCT) measurements in children
with fever and chemotherapy-induced neutropenia.
Patients undergoing chemotherapy for cancer will have
periods of neutropenia, and during these times, febrile
patients are at a higher risk for developing bacteremia.1
Over the past 3 decades, clinicians have attempted to
identify children with fever and neutropenia to be at
either high or low risk for a serious bacterial infection.
The hopes of risk classification were to decrease the rate
of hospital admissions, to prevent the emergence of anti-
microbial resistance,2 to avoid in-hospital complica-
tions, and to decrease the impairment of quality of life to
patients and their families. Oncologists have categorized
high- and low-risk adult patients for the development of
bacteremia, but their recommendations have been lim-
ited.3-6 Similarly, high- and low-risk classification stud-
ies have been evaluated in pediatric patients. Even
though there have been retrospective,7-14 prospec-
tive,15-19 and validation studies20 for high- and low-risk
patients, the majority of the pediatric oncologists have
been slow to adapt risk classifications for serious bacte-
rial infections in this high-risk population.
Regardless of risk, pediatric patients undergoing che-
motherapy continue to be routinely hospitalized for
fever and neutropenia. The current treatment consensus
for fever and neutropenia in pediatric patients has been
hospital admission, initiation of broad-spectrum antibi-
otics, and maintenance until the blood culture results are
negative for bacterial growth.21 Kara et al22 showed that
pediatric blood cultures may not produce growth for the
first 48 hours. Their study had bacterial growth in 54%
of children by day 3, 77% by day 4, and 89% by day 5.22
Furthermore, even when the clinical picture depicts a
patient who is septic, the blood culture may not produce
bacterial growth.23 Several studies have shown this to be
evident in pediatric patients because the blood volume
obtained is inadequate for bacterial growth.22,24,25 On the
contrary, blood cultures are widely known to have false
positives. Although blood cultures are not perfect, it is
still the gold standard for detecting bacteremia.
460913CPJ XXX10.1 177/0009922812460913 Clinical PediatricsReitman et al
1University of California, San Francisco-Fresno, Fresno, CA, USA2Children’s Hospital Central California, Madera, CA, USA
Corresponding Author:
Aaron J. Reitman, Children’s Hospital Los Angeles, 4650 Sunset Blvd,
Los Angeles, CA 90027
Email: [email protected]
Serial Procalcitonin Levels to Detect
Bacteremia in Febrile Neutropenia
Aaron J. Reitman, DO1,2, Rhonda M. Pisk, MS2, John V. Gates III, MD1,2, and J. Daniel Ozeran, MD, PhD1,2
Abstract
Background. Our objective was to evaluate serial procalcitonin (PCT) levels compared with an initial PCT level at
admission in predicting bacteremia in pediatric febrile neutropenic oncology patients. Procedure. Serum PCT levels
were measured at admission (t0) and within 24 hours of admission (t1) in pediatric oncology patients presenting
with fever and neutropenia. A blood culture was collected at t0 and monitored for 5 days for bacterial growth. PCT
value of 0.5 ng/mL at either t0 or t1 was considered predictive for bacteremia. Results. PCT levels were significantly
higher in children with positive blood cultures than with negative blood cultures. Serial PCT values mirrored t1
values. Serial PCT showed 76% specificity and negative predictive value of 93% in ruling out bacteremia. Conclusion.
Elevated PCT levels are predictive of bacteremia. Using serial PCT levels within 24 hours allowed a better prediction
of bacteremia than the PCT level at t0.
Keywords
procalcitonin, febrile, neutropenia, oncology, pediatric
Reitman 2012 (3)
1178 Clinical Pediatrics 51(12)
ruling out bacteremia. Using the ROC curve analysis,
the area under the curve (AUC) was determined at t0, t1,
and serial draws (0.77, 0.88, and 0.88, respectively;
Figure 2). The AUC of 0.88 indicates serial PCT draws
to be a better biomarker than a single PCT draw for bac-
teremia in this population.
The prevalence of bacteremia in the study population
was 20% or 1 in 5 patients. Using the positive likelihood
ratio, there is an 85% probability that the patients found
to have a positive serial PCT result will have bactere-
mia. Likewise, the negative likelihood ratios can be
used to determine that a patient with a negative serial
PCT level has less than a 1% chance of having bactere-
mia. These results again suggest that PCT is a useful
diagnostic test in this patient population (Table 3).
In the attempt to establish the optimal PCT cutoff
value to be used in our specific population, the diagnos-
tic sensitivity and specificity of PCT were explored using
the ROC results. The best combination of sensitivity and
specificity in this population was achieved at a cutoff
value of 0.4 ng/mL at both t0 and t1 time points.
Discussion
Children undergoing chemotherapy for cancer will most
certainly have episodes with fever and neutropenia dur-
ing treatment. This association occurs with greater fre-
quency with the growing intensity of chemotherapy.
The rapid progression of bacterial infections in neutro-
penic pediatric patients to sepsis is one reason why
these patients are frequently admitted to the hospital
and broad-spectrum antibiotics are initiated.
The precise volume of blood needed to adequately
detect bacteremia in children has not been established as
in adults.24,43,44 Blood cultures may not yield bacterial
growth for several days. Nonetheless, blood cultures are
still considered the gold standard for the detection of
bacteremia. The presence of a reliable sepsis marker
could assist in clinical decision making.
In children presenting with fever and neutropenia,
PCT has been shown to be a useful biomarker in detect-
ing serious bacterial infections.19,27-30,35-39 This study
confirms the results from previous studies as well as
demonstrates the importance of serial PCT levels in the
detection of bacteremia. This study showed serial PCT
draws to be better at detecting bacteremia than a single
PCT level, with the average increase in sensitivity
Figure 1. Patient flow diagram
Table 1. Evaluation of Procalcitonin at 2 Time Pointsa
Mean PCT
t0 (ng/mL) t1 (ng/mL) P
Bacteremic 4.090 11.600 <.05
Nonbacteremic 0.542 0.715 .22
P .001 .0001
Abbreviations: PCT, procalcitonin; t0, PCT draw at admission; t1, PCT
second draw.aSerial results mirror t1 results.
Table 2. Serial Blood Draws
PCT Serial
(t0/t1)
Blood Culture
Negative (n)
Blood Culture
Positive (n)
Neg/Neg 54 4
Pos/Pos 15 9
Pos/Neg 0 0
Neg/Pos 2 5
Abbreviations: PCT, procalcitonin; t0, PCT draw at admission; t1,
PCT second draw; Neg, negative PCT ≤0.5 ng/mL; Pos, positive
PCT >0.5 ng/mL.
Clinical Pediatrics
51(12) 1175 –1183
© The Author(s) 2012
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0009922812460913
http://cpj.sagepub.com
Introduction
This article reports on a small-to-medium sized, prospec-
tive, single-center study on the prediction of bacteremia
by serial procalcitonin (PCT) measurements in children
with fever and chemotherapy-induced neutropenia.
Patients undergoing chemotherapy for cancer will have
periods of neutropenia, and during these times, febrile
patients are at a higher risk for developing bacteremia.1
Over the past 3 decades, clinicians have attempted to
identify children with fever and neutropenia to be at
either high or low risk for a serious bacterial infection.
The hopes of risk classification were to decrease the rate
of hospital admissions, to prevent the emergence of anti-
microbial resistance,2 to avoid in-hospital complica-
tions, and to decrease the impairment of quality of life to
patients and their families. Oncologists have categorized
high- and low-risk adult patients for the development of
bacteremia, but their recommendations have been lim-
ited.3-6 Similarly, high- and low-risk classification stud-
ies have been evaluated in pediatric patients. Even
though there have been retrospective,7-14 prospec-
tive,15-19 and validation studies20 for high- and low-risk
patients, the majority of the pediatric oncologists have
been slow to adapt risk classifications for serious bacte-
rial infections in this high-risk population.
Regardless of risk, pediatric patients undergoing che-
motherapy continue to be routinely hospitalized for
fever and neutropenia. The current treatment consensus
for fever and neutropenia in pediatric patients has been
hospital admission, initiation of broad-spectrum antibi-
otics, and maintenance until the blood culture results are
negative for bacterial growth.21 Kara et al22 showed that
pediatric blood cultures may not produce growth for the
first 48 hours. Their study had bacterial growth in 54%
of children by day 3, 77% by day 4, and 89% by day 5.22
Furthermore, even when the clinical picture depicts a
patient who is septic, the blood culture may not produce
bacterial growth.23 Several studies have shown this to be
evident in pediatric patients because the blood volume
obtained is inadequate for bacterial growth.22,24,25 On the
contrary, blood cultures are widely known to have false
positives. Although blood cultures are not perfect, it is
still the gold standard for detecting bacteremia.
460913CPJ XXX10.1 177/0009922812460913 Clinical PediatricsReitman et al
1University of California, San Francisco-Fresno, Fresno, CA, USA2Children’s Hospital Central California, Madera, CA, USA
Corresponding Author:
Aaron J. Reitman, Children’s Hospital Los Angeles, 4650 Sunset Blvd,
Los Angeles, CA 90027
Email: [email protected]
Serial Procalcitonin Levels to Detect
Bacteremia in Febrile Neutropenia
Aaron J. Reitman, DO1,2, Rhonda M. Pisk, MS2, John V. Gates III, MD1,2, and J. Daniel Ozeran, MD, PhD1,2
Abstract
Background. Our objective was to evaluate serial procalcitonin (PCT) levels compared with an initial PCT level at
admission in predicting bacteremia in pediatric febrile neutropenic oncology patients. Procedure. Serum PCT levels
were measured at admission (t0) and within 24 hours of admission (t1) in pediatric oncology patients presenting
with fever and neutropenia. A blood culture was collected at t0 and monitored for 5 days for bacterial growth. PCT
value of 0.5 ng/mL at either t0 or t1 was considered predictive for bacteremia. Results. PCT levels were significantly
higher in children with positive blood cultures than with negative blood cultures. Serial PCT values mirrored t1
values. Serial PCT showed 76% specificity and negative predictive value of 93% in ruling out bacteremia. Conclusion.
Elevated PCT levels are predictive of bacteremia. Using serial PCT levels within 24 hours allowed a better prediction
of bacteremia than the PCT level at t0.
Keywords
procalcitonin, febrile, neutropenia, oncology, pediatric
Reitman 2012 (4)
Reitman et al 1179
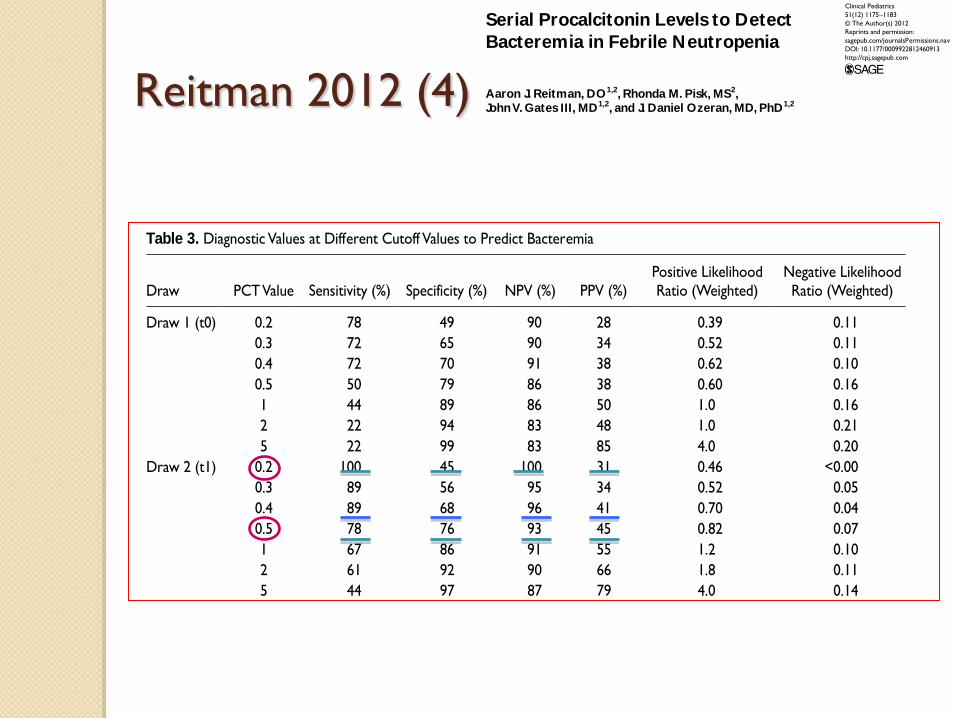
Table 3. Diagnostic Values at Different Cutoff Values to Predict Bacteremia
Draw PCT Value Sensitivity (%) Specificity (%) NPV (%) PPV (%)
Positive Likelihood
Ratio (Weighted)
Negative Likelihood
Ratio (Weighted)
Draw 1 (t0) 0.2 78 49 90 28 0.39 0.11
0.3 72 65 90 34 0.52 0.11
0.4 72 70 91 38 0.62 0.10
0.5 50 79 86 38 0.60 0.16
1 44 89 86 50 1.0 0.16
2 22 94 83 48 1.0 0.21
5 22 99 83 85 4.0 0.20
Draw 2 (t1) 0.2 100 45 100 31 0.46 <0.00
0.3 89 56 95 34 0.52 0.05
0.4 89 68 96 41 0.70 0.04
0.5 78 76 93 45 0.82 0.07
1 67 86 91 55 1.2 0.10
2 61 92 90 66 1.8 0.11
5 44 97 87 79 4.0 0.14
Seriala 0.2 100 45 100 31 0.46 <0.00
0.3 89 56 95 34 0.52 0.05
0.4 89 68 96 41 0.70 0.04
0.5 78 76 93 45 0.82 0.07
1 67 86 91 55 1.2 0.10
2 61 92 90 66 1.8 0.11
5 44 97 87 79 4.0 0.14
Abbreviations: PCT, procalcitonin; t0, PCT draw at admission; t1, PCT second draw; NPV, negative predictive value; PPV, positive predictive value.aSerial results mirror t1 results.
Figure 2. Receiver operating characteristic cur ve
Clinical Pediatrics
51(12) 1175 –1183
© The Author(s) 2012
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0009922812460913
http://cpj.sagepub.com
Introduction
This article reports on a small-to-medium sized, prospec-
tive, single-center study on the prediction of bacteremia
by serial procalcitonin (PCT) measurements in children
with fever and chemotherapy-induced neutropenia.
Patients undergoing chemotherapy for cancer will have
periods of neutropenia, and during these times, febrile
patients are at a higher risk for developing bacteremia.1
Over the past 3 decades, clinicians have attempted to
identify children with fever and neutropenia to be at
either high or low risk for a serious bacterial infection.
The hopes of risk classification were to decrease the rate
of hospital admissions, to prevent the emergence of anti-
microbial resistance,2 to avoid in-hospital complica-
tions, and to decrease the impairment of quality of life to
patients and their families. Oncologists have categorized
high- and low-risk adult patients for the development of
bacteremia, but their recommendations have been lim-
ited.3-6 Similarly, high- and low-risk classification stud-
ies have been evaluated in pediatric patients. Even
though there have been retrospective,7-14 prospec-
tive,15-19 and validation studies20 for high- and low-risk
patients, the majority of the pediatric oncologists have
been slow to adapt risk classifications for serious bacte-
rial infections in this high-risk population.
Regardless of risk, pediatric patients undergoing che-
motherapy continue to be routinely hospitalized for
fever and neutropenia. The current treatment consensus
for fever and neutropenia in pediatric patients has been
hospital admission, initiation of broad-spectrum antibi-
otics, and maintenance until the blood culture results are
negative for bacterial growth.21 Kara et al22 showed that
pediatric blood cultures may not produce growth for the
first 48 hours. Their study had bacterial growth in 54%
of children by day 3, 77% by day 4, and 89% by day 5.22
Furthermore, even when the clinical picture depicts a
patient who is septic, the blood culture may not produce
bacterial growth.23 Several studies have shown this to be
evident in pediatric patients because the blood volume
obtained is inadequate for bacterial growth.22,24,25 On the
contrary, blood cultures are widely known to have false
positives. Although blood cultures are not perfect, it is
still the gold standard for detecting bacteremia.
460913CPJ XXX10.1 177/0009922812460913 Clinical PediatricsReitman et al
1University of California, San Francisco-Fresno, Fresno, CA, USA2Children’s Hospital Central California, Madera, CA, USA
Corresponding Author:
Aaron J. Reitman, Children’s Hospital Los Angeles, 4650 Sunset Blvd,
Los Angeles, CA 90027
Email: [email protected]
Serial Procalcitonin Levels to Detect
Bacteremia in Febrile Neutropenia
Aaron J. Reitman, DO1,2, Rhonda M. Pisk, MS2, John V. Gates III, MD1,2, and J. Daniel Ozeran, MD, PhD1,2
Abstract
Background. Our objective was to evaluate serial procalcitonin (PCT) levels compared with an initial PCT level at
admission in predicting bacteremia in pediatric febrile neutropenic oncology patients. Procedure. Serum PCT levels
were measured at admission (t0) and within 24 hours of admission (t1) in pediatric oncology patients presenting
with fever and neutropenia. A blood culture was collected at t0 and monitored for 5 days for bacterial growth. PCT
value of 0.5 ng/mL at either t0 or t1 was considered predictive for bacteremia. Results. PCT levels were significantly
higher in children with positive blood cultures than with negative blood cultures. Serial PCT values mirrored t1
values. Serial PCT showed 76% specificity and negative predictive value of 93% in ruling out bacteremia. Conclusion.
Elevated PCT levels are predictive of bacteremia. Using serial PCT levels within 24 hours allowed a better prediction
of bacteremia than the PCT level at t0.
Keywords
procalcitonin, febrile, neutropenia, oncology, pediatric
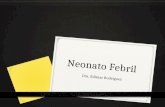
Reitman 2012 (5)
Conclou: ◦ La utilització de 2 determinacions de PCT en les 1es 24
hores pot ésser utilitzada en la detecció precoç de bacterièmies
◦ L’òptim cut-off de PCT és de 0.4 ng/ml (S 89%, E 68%, VPP 41% i VPN 96%)
◦ Una sensibilitat i VPN del 100% s’aconsegueix amb un cut-off de 0.2 ng/ml, que podria ésser utilitzat per un alta hospitalària precoç, en pacients clínicament bé abans de que els hemocultius siguin definitivament negatius
◦ La incorporació del nivells de PCT seriats de forma rutinària en aquests nins pot permetre intervencions més precoces davant elevacions dels valors de la PCT
Clinical Pediatrics
51(12) 1175 –1183
© The Author(s) 2012
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0009922812460913
http://cpj.sagepub.com
Introduction
This article reports on a small-to-medium sized, prospec-
tive, single-center study on the prediction of bacteremia
by serial procalcitonin (PCT) measurements in children
with fever and chemotherapy-induced neutropenia.
Patients undergoing chemotherapy for cancer will have
periods of neutropenia, and during these times, febrile
patients are at a higher risk for developing bacteremia.1
Over the past 3 decades, clinicians have attempted to
identify children with fever and neutropenia to be at
either high or low risk for a serious bacterial infection.
The hopes of risk classification were to decrease the rate
of hospital admissions, to prevent the emergence of anti-
microbial resistance,2 to avoid in-hospital complica-
tions, and to decrease the impairment of quality of life to
patients and their families. Oncologists have categorized
high- and low-risk adult patients for the development of
bacteremia, but their recommendations have been lim-
ited.3-6 Similarly, high- and low-risk classification stud-
ies have been evaluated in pediatric patients. Even
though there have been retrospective,7-14 prospec-
tive,15-19 and validation studies20 for high- and low-risk
patients, the majority of the pediatric oncologists have
been slow to adapt risk classifications for serious bacte-
rial infections in this high-risk population.
Regardless of risk, pediatric patients undergoing che-
motherapy continue to be routinely hospitalized for
fever and neutropenia. The current treatment consensus
for fever and neutropenia in pediatric patients has been
hospital admission, initiation of broad-spectrum antibi-
otics, and maintenance until the blood culture results are
negative for bacterial growth.21 Kara et al22 showed that
pediatric blood cultures may not produce growth for the
first 48 hours. Their study had bacterial growth in 54%
of children by day 3, 77% by day 4, and 89% by day 5.22
Furthermore, even when the clinical picture depicts a
patient who is septic, the blood culture may not produce
bacterial growth.23 Several studies have shown this to be
evident in pediatric patients because the blood volume
obtained is inadequate for bacterial growth.22,24,25 On the
contrary, blood cultures are widely known to have false
positives. Although blood cultures are not perfect, it is
still the gold standard for detecting bacteremia.
460913CPJ XXX10.1 177/0009922812460913 Clinical PediatricsReitman et al
1University of California, San Francisco-Fresno, Fresno, CA, USA2Children’s Hospital Central California, Madera, CA, USA
Corresponding Author:
Aaron J. Reitman, Children’s Hospital Los Angeles, 4650 Sunset Blvd,
Los Angeles, CA 90027
Email: [email protected]
Serial Procalcitonin Levels to Detect
Bacteremia in Febrile Neutropenia
Aaron J. Reitman, DO1,2, Rhonda M. Pisk, MS2, John V. Gates III, MD1,2, and J. Daniel Ozeran, MD, PhD1,2
Abstract
Background. Our objective was to evaluate serial procalcitonin (PCT) levels compared with an initial PCT level at
admission in predicting bacteremia in pediatric febrile neutropenic oncology patients. Procedure. Serum PCT levels
were measured at admission (t0) and within 24 hours of admission (t1) in pediatric oncology patients presenting
with fever and neutropenia. A blood culture was collected at t0 and monitored for 5 days for bacterial growth. PCT
value of 0.5 ng/mL at either t0 or t1 was considered predictive for bacteremia. Results. PCT levels were significantly
higher in children with positive blood cultures than with negative blood cultures. Serial PCT values mirrored t1
values. Serial PCT showed 76% specificity and negative predictive value of 93% in ruling out bacteremia. Conclusion.
Elevated PCT levels are predictive of bacteremia. Using serial PCT levels within 24 hours allowed a better prediction
of bacteremia than the PCT level at t0.
Keywords
procalcitonin, febrile, neutropenia, oncology, pediatric
Niño Jesús 2015 (1)
Objectiu: Avaluar el valor predictiu de PCT i PCR en detectar infecció greu en les NF que acudeixen a Urgències (2013-2014)
Definició d’infecció greu: ◦ Bacterièmia ◦ Inestabilitat hemodinàmica ◦ Ingrés a la UCI
75 NF
Utilidad de PCR y PCT para y ppredecir infección grave en niños con neutropenia febril.
J L Al d S R d i M Ji M J M tíJ.L. Almodovar, S. Rodriguez, M. Jimenez, M.J. Martín
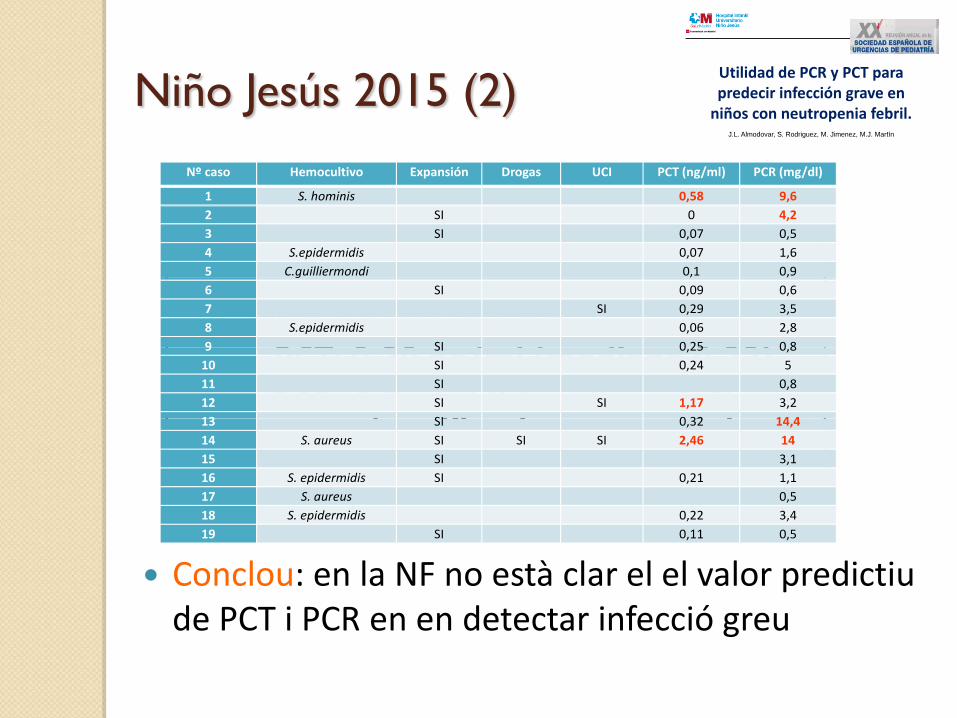
Niño Jesús 2015 (2)
Conclou: en la NF no està clar el el valor predictiu de PCT i PCR en en detectar infecció greu
ResultadosResultadosNº caso Hemocultivo Expansión Drogas UCI PCT (ng/ml) PCR (mg/dl)
1 S. hominis 0,58 9,6
2 SI 0 4,2
3 SI 0,07 0,5
4 S.epidermidis 0,07 1,6
5 C.guilliermondi 0,1 0,9
De los 19 pacientes: PCT 0 39 / l ( di 0 32)
g , ,
6 SI 0,09 0,6
7 SI 0,29 3,5
8 S.epidermidis 0,06 2,8
9 SI 0 25 0 8
‐PCT: 0,39 ng/ml (mediana 0,32)‐PCR: 3,7 mg/dl (mediana 2,8)
9 SI 0,25 0,8
10 SI 0,24 5
11 SI 0,8
12 SI SI 1,17 3,2
13 SI 0 32 14 4, g/ ( , )
13 SI 0,32 14,4
14 S. aureus SI SI SI 2,46 14
15 SI 3,1
16 S. epidermidis SI 0,21 1,1
17 S. aureus 0,5
18 S. epidermidis 0,22 3,4
19 SI 0,11 0,5
Utilidad de PCR y PCT para y ppredecir infección grave en niños con neutropenia febril.
J L Al d S R d i M Ji M J M tíJ.L. Almodovar, S. Rodriguez, M. Jimenez, M.J. Martín
Son Espases 2015 (1)
Objectiu: ◦ Avaluar el valor predictiu de PCT i PCR en detectar
infecció sistèmica en NF que acudeixen a Urgències (2011-2015)
Definició de infecció sistèmica: ◦ Creixement de bacteri o fong a l’hemocultiu
40 NF:
◦ 13 FSF ◦ 7 febres documentades clínicament (cap sèpsia clínica) ◦ 6 infeccions víriques documentades ◦ 6 infeccions bacterianes localitzades documentades ◦ 7 bacterièmies i 1 candidèmia (cap sèpsia clínica o
severa)
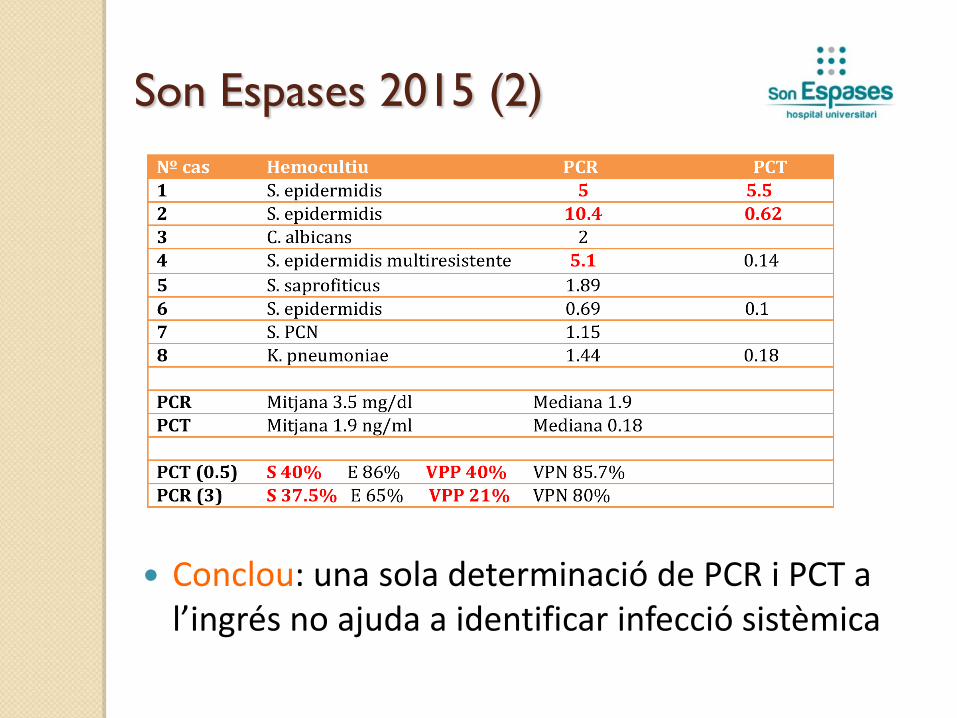
Son Espases 2015 (2)
Conclou: una sola determinació de PCR i PCT a l’ingrés no ajuda a identificar infecció sistèmica
Shu-Guang 2012 (1)
Objectiu: Avaluar el rol de la PCT en el diagnòstic de sèpsia bacteriana en la NF
Avaluen:
◦ 10 estudis de PCT
◦ 8 de PCR
PCT i PCR: 304 SB de 1031 NF (29.5%)
PCR: 741 SB de 1316 NF(56.3%)
Role of Procalcitonin in the Diagnosis of Severe
Infection in Pediatric Patients With Fever and
Neutropenia—A Systemic Review and Meta-analysis
Shu-Guang Lin et al.
The Pediatric Infectious Disease Journal – October 2012
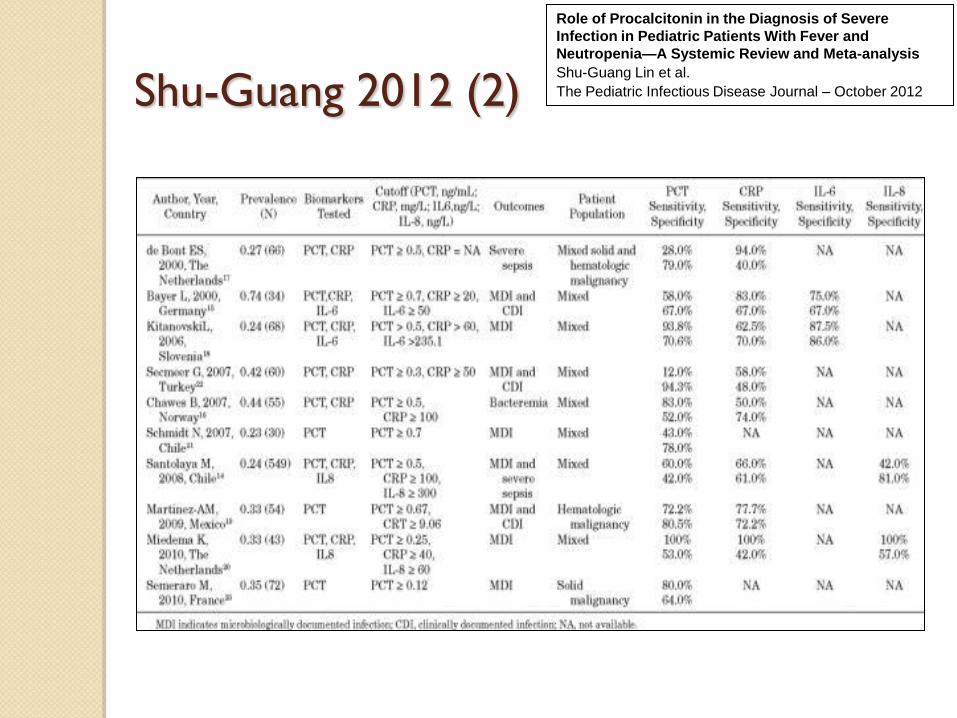
Shu-Guang 2012 (2)
Role of Procalcitonin in the Diagnosis of Severe
Infection in Pediatric Patients With Fever and
Neutropenia—A Systemic Review and Meta-analysis
Shu-Guang Lin et al.
The Pediatric Infectious Disease Journal – October 2012
Shu-Guang 2012 (3)
Conclou:
◦ La PCT i la PCR tenen un valor comparable i complementari en el diagnòstic de SB
◦ La PCT es més específica i que la PCR es més sensible
◦ Recomanen per la PCT el cut-off de 0.5 ng/ml
◦ Suggereixen que amb una 2ª mostra de PCT a les 24 hores de la 1ª augmentaria en gran mesura la sensibilitat de la PCT
Role of Procalcitonin in the Diagnosis of Severe
Infection in Pediatric Patients With Fever and
Neutropenia—A Systemic Review and Meta-analysis
Shu-Guang Lin et al.
The Pediatric Infectious Disease Journal – October 2012
Dificultats en l’avaluació del paper
dels biomarcadors Les sèries estudiades corresponen a pacients
heterogenis (malaltia de base, nº de neutròfils,
etc.)
No estan ben definides les definicions de NF
d’evolució desfavorable
L’agrupació de diagnòstics finals de les NF no és
uniforme i en alguns casos agrupa quadres clínics i
situacions clíniques ben diferents
Causes de NF
Febre sense focus o FOD
Infecció vírica documentada
Infecció fúngica documentada: ◦ Localitzada
◦ Sistèmica
Infecció bacteriana documentada: ◦ Localitzada
◦ Bacterièmia
◦ Bacterièmia amb criteris clínics de sèpsia
Infecció clínicament documentada: ◦ Infecció localitzada
◦ Sèpsia clínica
Coinfeccions
Què ens pot oferir la PCT?
Descartar inicialment infecció greu?: ◦ NO, especialment en una sola determinació
Orientar a decidir iniciar Tr antibiòtic en NF?: ◦ NO, sempre tractarem les NF
Orientar en el Tr antibiòtic a administrar?: ◦ Sí, valors alts de PCT poden decidir-nos a ampliar la cobertura ATB
Orientar en la duració del Tr antibiòtic hospitalari?: ◦ Sí, valors persistentment baixos de PCT poden decidir-nos a escurçar
el tr antibiòtic hospitalari
Orientar en l’estratègia diagnòstica en NF persistent?: ◦ Sí, PCT persistentment altes o normals poden influir-nos en la nostra
estratègia diagnòstica
Orientar en l’evolució clínica del pacient?: ◦ Sí, ens pot ser molt útil
Conclusions (1) Resultats no coincidents a la literatura
No existeixen uns punts de tall òptims validats
Els valors inicials de PCT i PCR a les NF NO es poden utilitzar per descartar inicialment infeccions greus
La combinació de determinacions seriades PCT i PCR pot ser MOLT ÚTIL en el maneig de les NF
Conclusions (2) Fa falta un esforç per tal de millorar el
rendiment diagnòstic de la combinació d’ambdós biomarcadors i trobar adequats punts de tall que ens ajudin a les decisions clíniques
Calen treballs col·laboratius amb una ADEQUADA i CONSENSUADA tipificació dels pacients, de les agrupacions de diagnòstics finals i de les definicions d’evolució desfavorable de les NF