
NOVEDADES(EN(EL(CONTROL( DEL(COLESTEROL(( 2016 ·...
69
NOVEDADES EN EL CONTROL DEL COLESTEROL 2016 Dr. Iñaki Lekuona Sº Cardiología HGU Osakidetza @inaki1954
Transcript of NOVEDADES(EN(EL(CONTROL( DEL(COLESTEROL(( 2016 ·...

NOVEDADES EN EL CONTROL DEL COLESTEROL
2016
Dr. Iñaki Lekuona Sº Cardiología HGU
Osakidetza @inaki1954

ESTATINAS
Mayor LDL-‐c
NPC1L1(EzeJmiba) IMPROVE-‐IT PCSK9 Inhibición*(Ac monoclonales) Lomitapide Mipomersen
ObjeJvo Combinado LDL-‐c HDL-‐c
HDL-‐c
CETP inhibidores Anacetrapib* HPS3-‐TIMI55
HDL reconsJtuido Apo A1 modulación
* Pendiente de ensayos clínicos
Lomitapide: inhibidora de la proteína de transferencia microsomal de TG(MTP) Mipomersen: oligonucleóJdo anJsenJdo RNA mensajero de apo B
LDL

Daniel J. Rader, and John J.P. Kastelein Circulation. 2014;129:1022-1032 Copyright © American Heart Association, Inc. All rights reserved.
LOMITAPIDE-‐MIPOMERSEN
Lomitapide: inhibidora de la proteína de transferencia microsomal de TG(MTP) Mipomersen: oligonucleóJdo anJsenJdo RNA mensajero de apo B

N Engl J Med 2015;372:2387-‐97

Pa@ents stabilized post ACS ≤ 10 days: LDL-‐C 50–125*mg/dL (or 50–100**mg/dL if prior lipid-‐lowering Rx)
Standard Medical & IntervenJonal Therapy
Eze@mibe / Simvasta@n 10 / 40 mg
Simvasta@n 40 mg
Follow-up Visit Day 30, every 4 months
Dura@on: Minimum 2 ½-‐year follow-‐up (at least 5250 events)
Primary Endpoint: CV death, MI, hospital admission for UA, coronary revascularizaJon (≥ 30 days aker randomizaJon), or stroke
N=18,144
UpJtrated to Simva 80 mg if LDL-‐C > 79 (adapted per
FDA label 2011)
IMPROVE-‐IT Diseño
*3.2mM **2.6mM
Cannon CP AHJ 2008;156:826-‐32; Califf RM NEJM 2009;361:712-‐7; Blazing MA AHJ 2014;168:205-‐12
90% power to detect ~9% difference

IMPROVE-‐IT
N Engl J Med 2015;372:2387-‐97
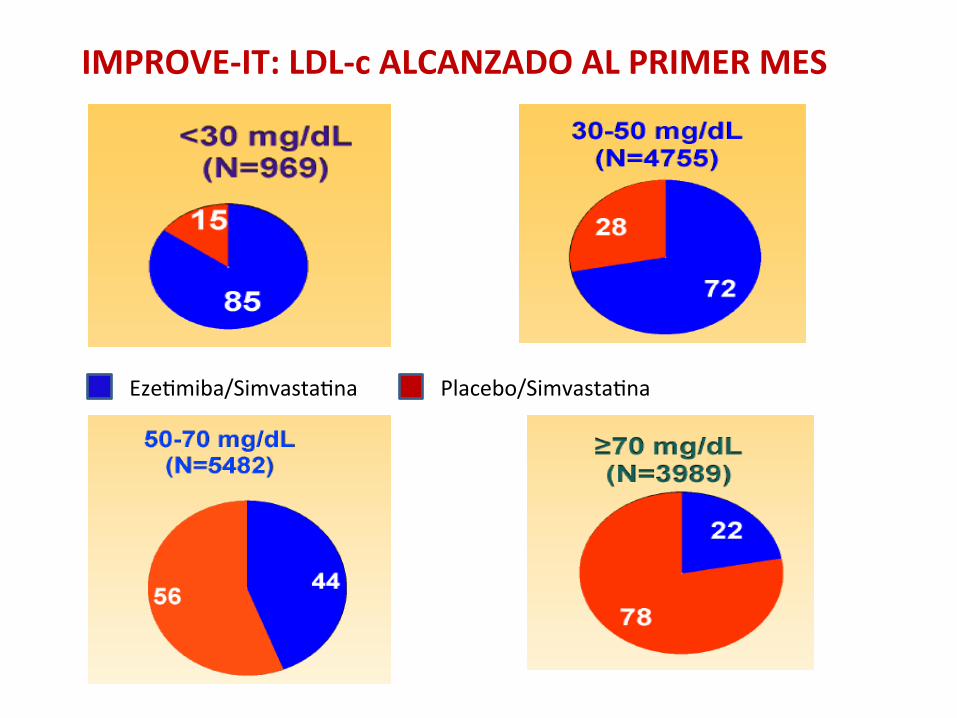
IMPROVE-‐IT: LDL-‐c ALCANZADO AL PRIMER MES
EzeJmiba/SimvastaJna Placebo/SimvastaJna

Kaplan–Meier Curves for the Primary Efficacy End Point*
*Death from cardiovascular disease, a major coronary event (nonfatal myocardial infarcJon, documented unstable angina requiring hospital admission, or coronary revascularizaJon occurring at least 30 days aker randomizaJon), or nonfatal stroke in the intenJon-‐to-‐treat populaJon during the overall study period
N Engl J Med 2015;372:2387-‐97
2.742 eventos vs. 2.572
NNT=50

OBJETIVOS INDIVIDUALES
N Engl J Med 2015;372:2387-‐97
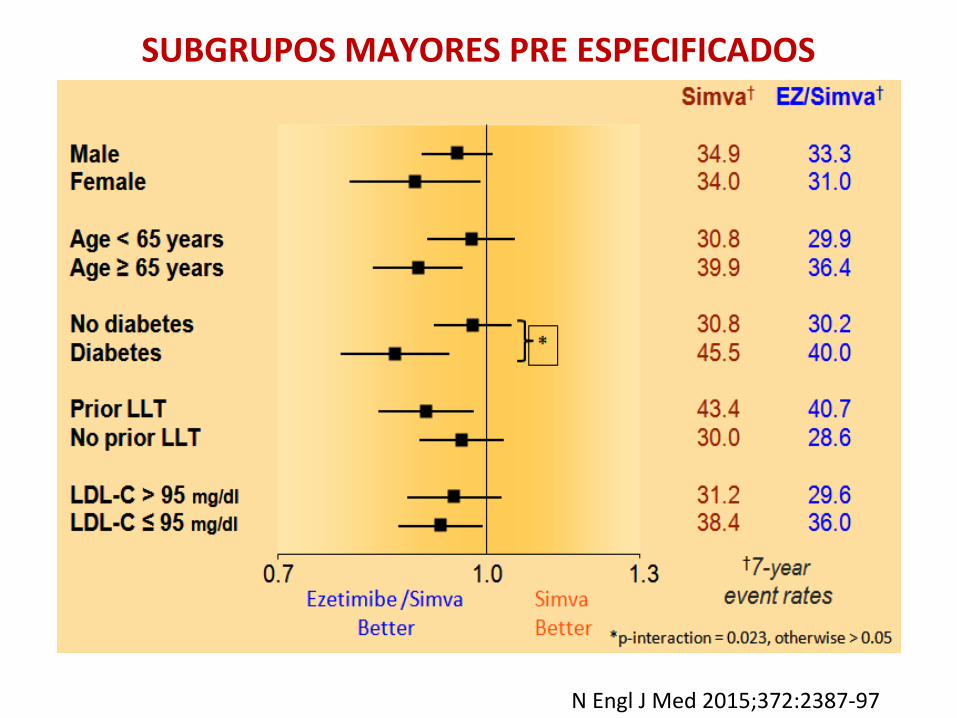
SUBGRUPOS MAYORES PRE ESPECIFICADOS
N Engl J Med 2015;372:2387-‐97

J Am Coll Cardiol 2016;67:353–61

J Am Coll Cardiol 2016;67:353–61
Total Events During Follow-‐Up by Randomiza@on Group for Components of the Primary Endpoint
First, Addi@onal, and Total Primary Endpoint Events During Follow-‐Up by Randomiza@on Group
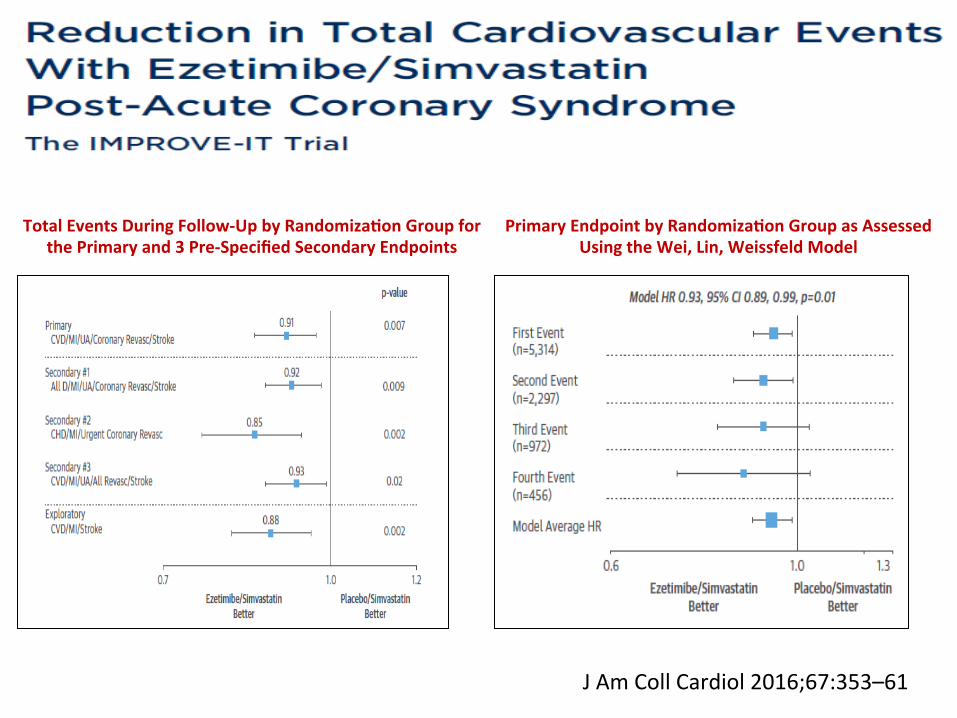
Primary Endpoint by Randomiza@on Group as Assessed Using the Wei, Lin, Weissfeld Model
Total Events During Follow-‐Up by Randomiza@on Group for the Primary and 3 Pre-‐Specified Secondary Endpoints
J Am Coll Cardiol 2016;67:353–61
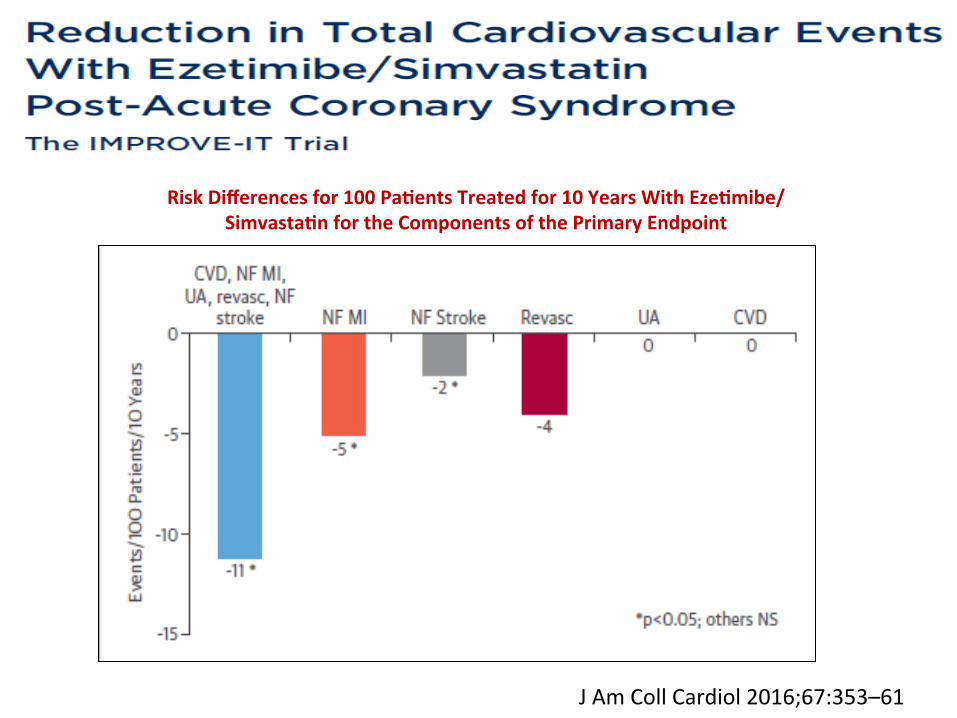
J Am Coll Cardiol 2016;67:353–61
Risk Differences for 100 Pa@ents Treated for 10 Years With Eze@mibe/ Simvasta@n for the Components of the Primary Endpoint
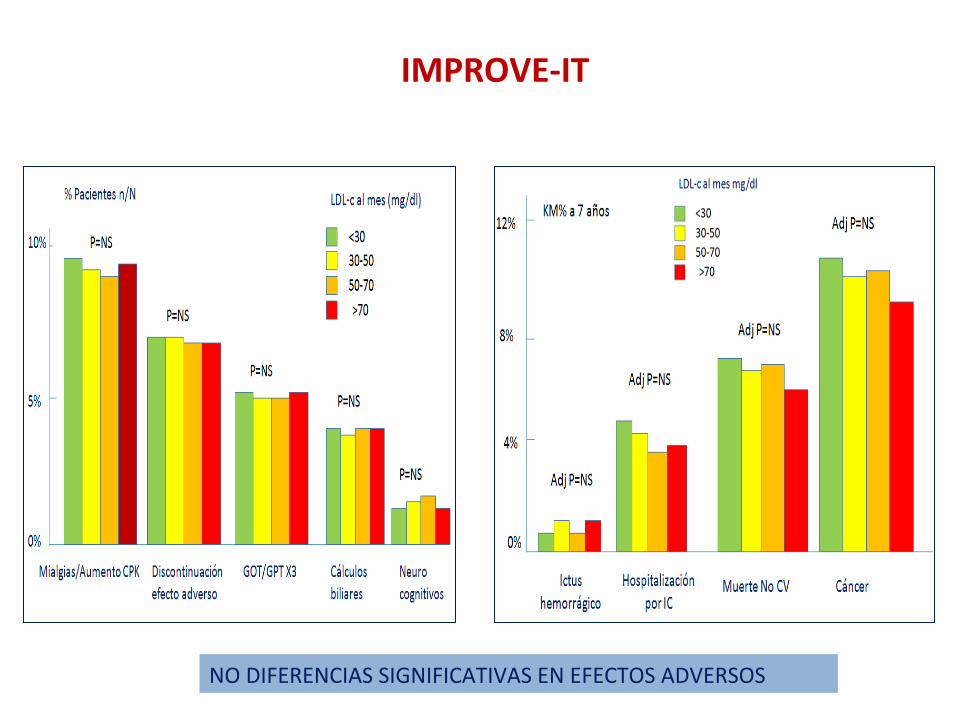
IMPROVE-‐IT
NO DIFERENCIAS SIGNIFICATIVAS EN EFECTOS ADVERSOS
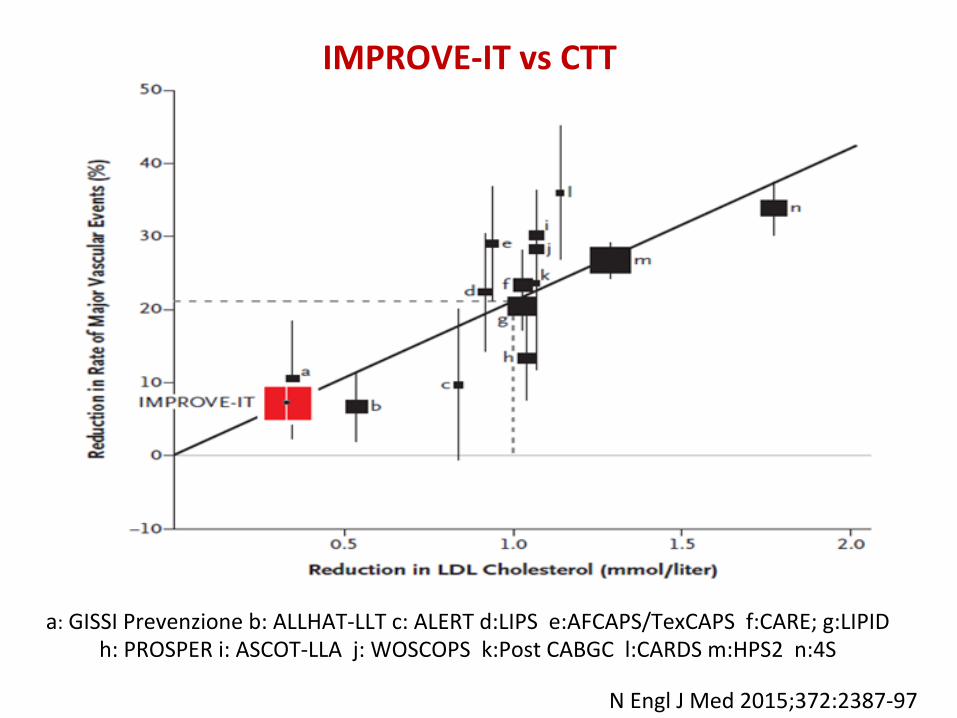
a: GISSI Prevenzione b: ALLHAT-‐LLT c: ALERT d:LIPS e:AFCAPS/TexCAPS f:CARE; g:LIPID h: PROSPER i: ASCOT-‐LLA j: WOSCOPS k:Post CABGC l:CARDS m:HPS2 n:4S
IMPROVE-‐IT vs CTT
N Engl J Med 2015;372:2387-‐97

PRECISE–IVUS Trial
J Am Coll Cardiol 2015; 66:495–507
63.2 ± 16.3 mg/dl vs. 73.3 ± 20.3 mg/dl
PAV: absolute change in percent atheroma volume
Plaque regression (78% vs. 58%; p < 0.004)
LDL-‐c

N Engl J Med 2014; 371:2072-‐2082
COLESTEROL Y GENÉTICA
12 mg/dl menos C-‐LDL de por vida se asocia a reducción del 53% de EC
ACC/AHA 2013
50%
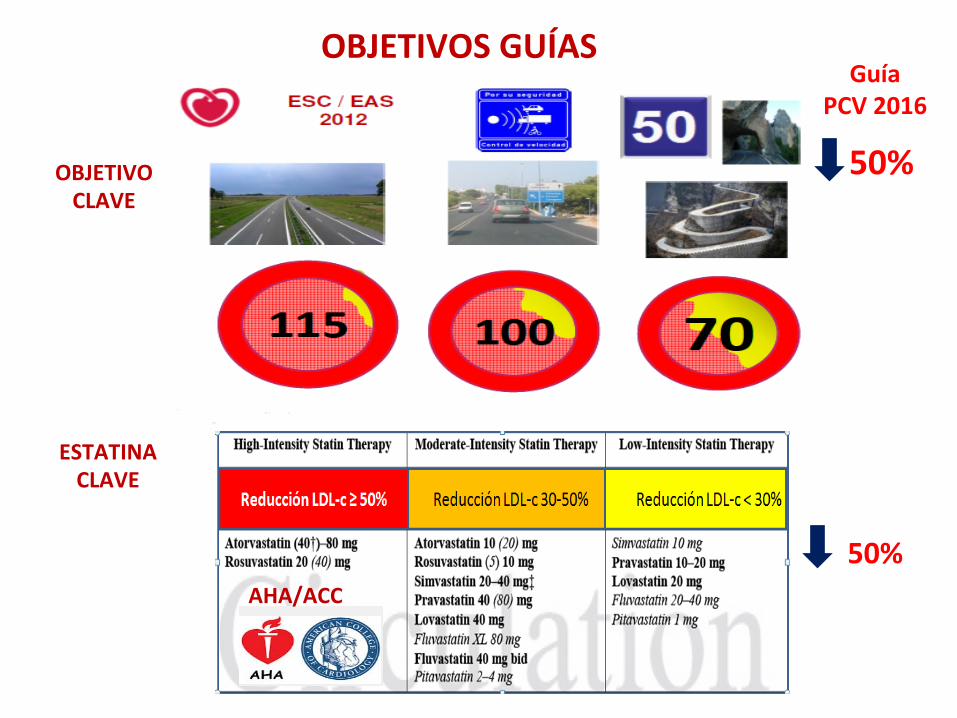
OBJETIVOS GUÍAS
AHA/ACC
OBJETIVO CLAVE
ESTATINA CLAVE
50%
Guía PCV 2016


ESC 2015
CONSECUCIÓN DE OBJETIVOS LDL-‐C
EUROASPIRE IV CONTROL FRCV ESPAÑA
Rev Esp Cardiol. 2016;69(4):401–407

UNIDADES LÍPIDOS ESPAÑA
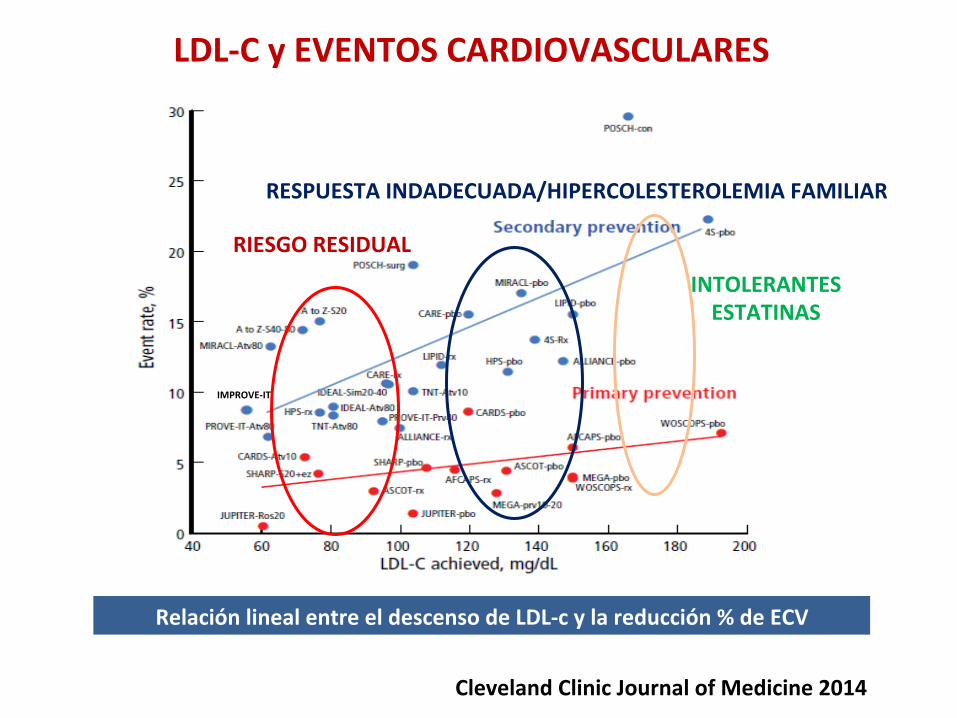
LDL-‐C y EVENTOS CARDIOVASCULARES
Cleveland Clinic Journal of Medicine 2014
Relación lineal entre el descenso de LDL-‐c y la reducción % de ECV
IMPROVE-‐IT
RIESGO RESIDUAL
RESPUESTA INDADECUADA/HIPERCOLESTEROLEMIA FAMILIAR
INTOLERANTES ESTATINAS
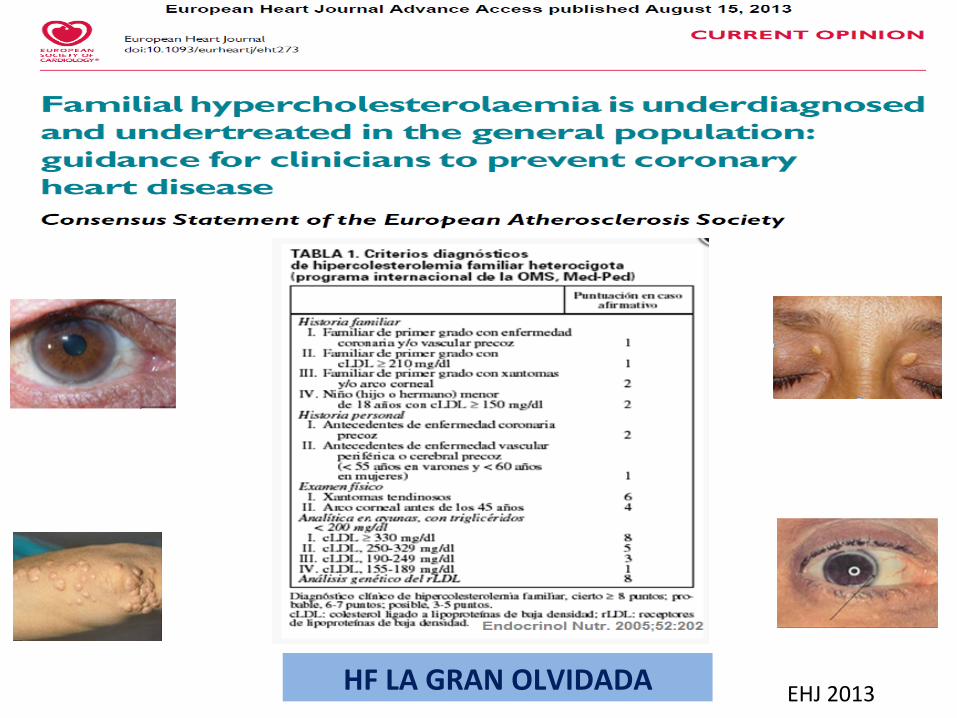
HF LA GRAN OLVIDADA EHJ 2013
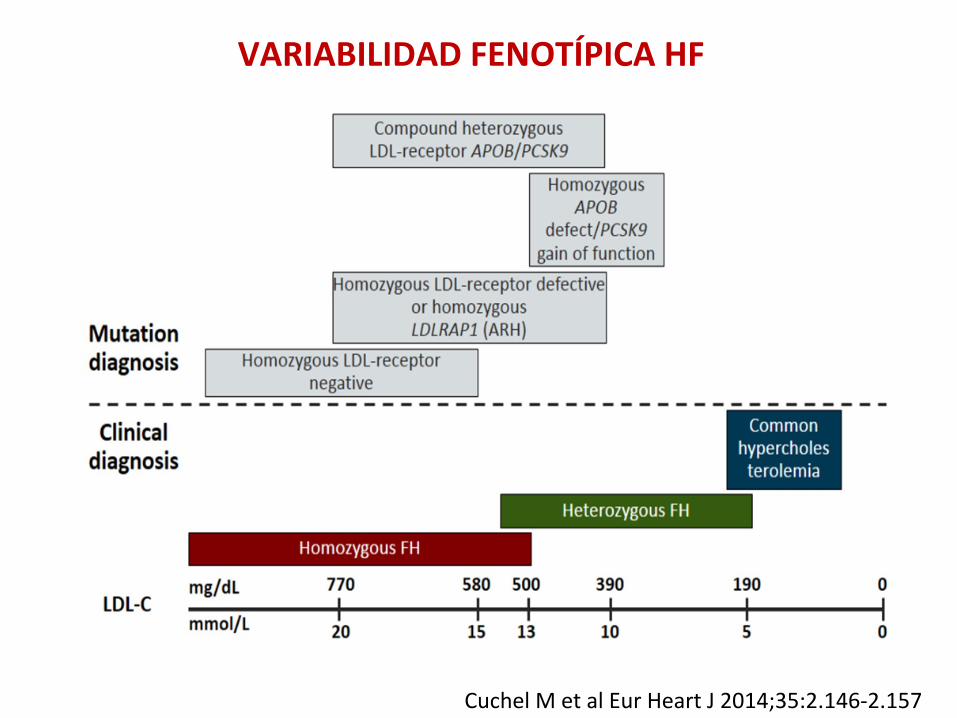
VARIABILIDAD FENOTÍPICA HF
Cuchel M et al Eur Heart J 2014;35:2.146-‐2.157

MUTACIONES PCSK9 Y RIESGO CARDIOVASCULAR
Benn M et al. J Am Coll Cardiol. 2010;55:2833
Cohen JC et al. N Engl J Med. 2006;354:1264-‐1272
Abifadel M et al. Nat Genet. 2003;34:154-‐15
Haddad L et al. J Lipid Res. 1999;40:1113-‐1122
PCSK9 Proprotein convertase subJlisin / kexin type 9

PCSK9
1. Abifadel et al. Hum Mutat 2009;30:520–529 2. Seidah et al. Proc Natl Acad Sci USA 2003;100:928–933 3. Horton et al. J Lipid Res 2009;50:S172–S177
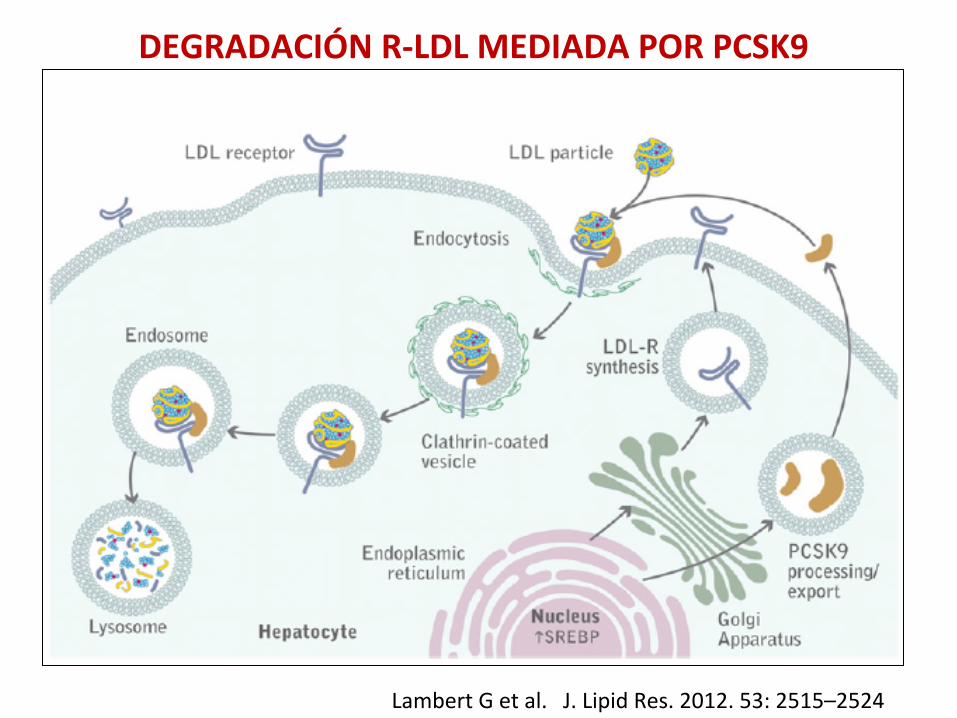
DEGRADACIÓN R-‐LDL MEDIADA POR PCSK9
J. Lipid Res. 2012. 53: 2515–2524 Lambert G et al.

Lambert G et al. J Lipid Res. 2012;53:2515-‐2524
MONOCLONALES ANTI-‐PCSK9

INHIBIDORES DE PCSK9
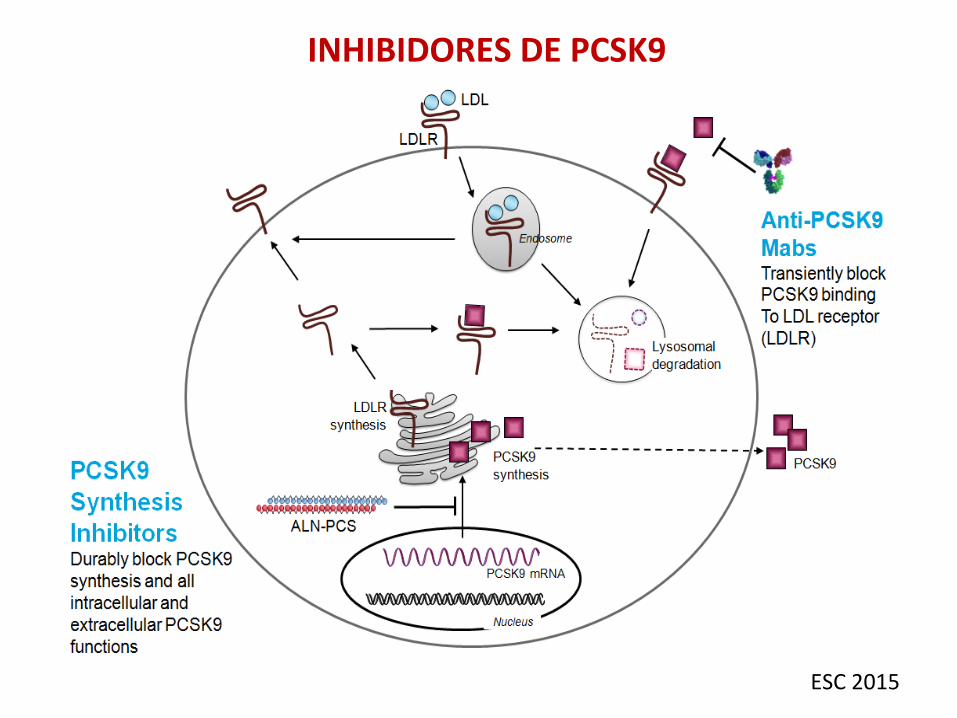
ESC 2015
INHIBIDORES DE PCSK9

ESC 2015

INHIBIDORES PCSK-‐9
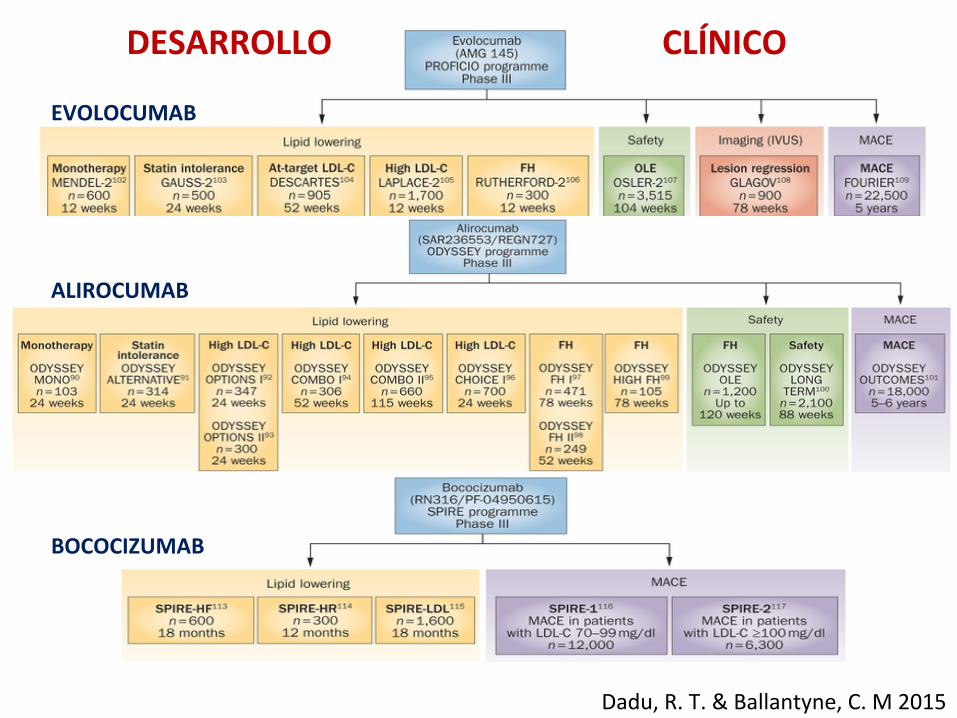
Dadu, R. T. & Ballantyne, C. M 2015
EVOLOCUMAB
ALIROCUMAB
BOCOCIZUMAB
DESARROLLO CLÍNICO

EVOLOCUMAB ASOCIADO A ESTATINAS
European Heart Journal doi:10.1093/eurheartj/ehv174

estudios abiertos aleatorizados fase 2 y 3 con 4.465 pacientes
140 mg every 2 w or 420 mg plus standard therapy or standard therapy alone
OSLER TRIALS
N Engl J Med 2015;372:1500-‐9

N Engl J Med 2015;372:1500-‐9
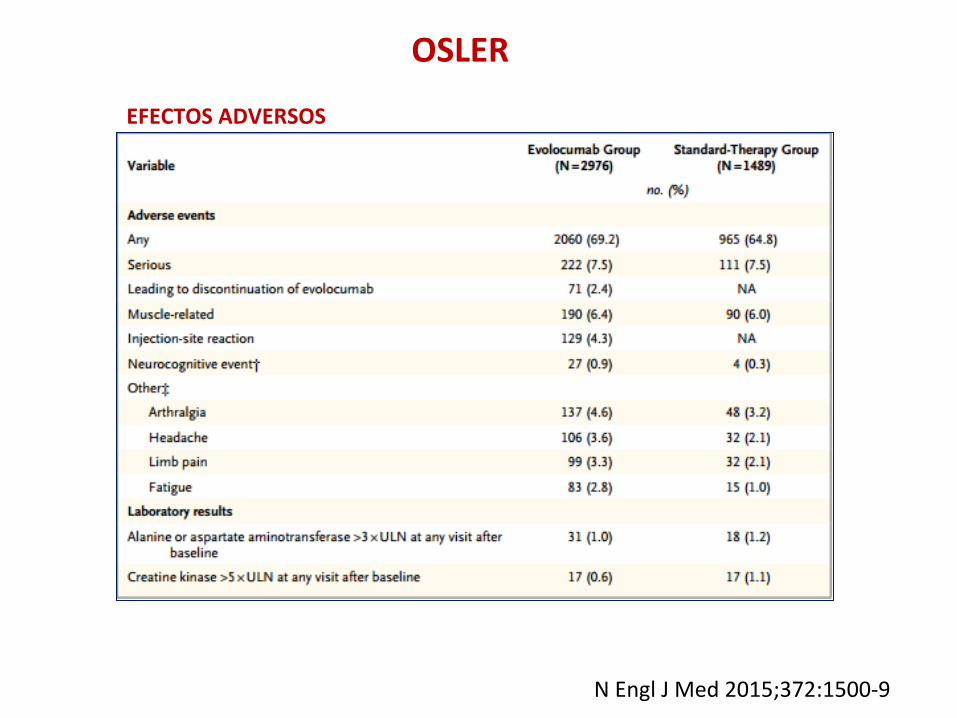
EFECTOS ADVERSOS
OSLER
N Engl J Med 2015;372:1500-‐9

EVOLOCUMAB:LAPLACE-‐TIMI57
Giugliano RP et al JACC 2015;65:2638-‐2651

ALIROCUMAB: CAMBIOS LDL-‐c CON DIFERENTES DOSIS
European Heart Journal doi:10.1093/eurheartj/ehv174

2.341 PACIENTES DE ALTO RIESGO LDL-‐c>70 mg/dl y tratamiento con estaJnas a la más alta dosis tolerada con ó sin otros hipolipemiantes, aleatorizados 2:1
Alirocumab 150 mg cada 15 días durante 78 semanas ó placebo. ObjeJvo primario de eficacia porcentaje de cambio en el nivel de LDL-‐c calculado
desde el nivel basal hasta la semana 24
ODYSSEY LONG TERM
N Engl J Med 2015;372:1489-‐99

N Engl J Med 2015;372:1489-‐99
61% 57.9%
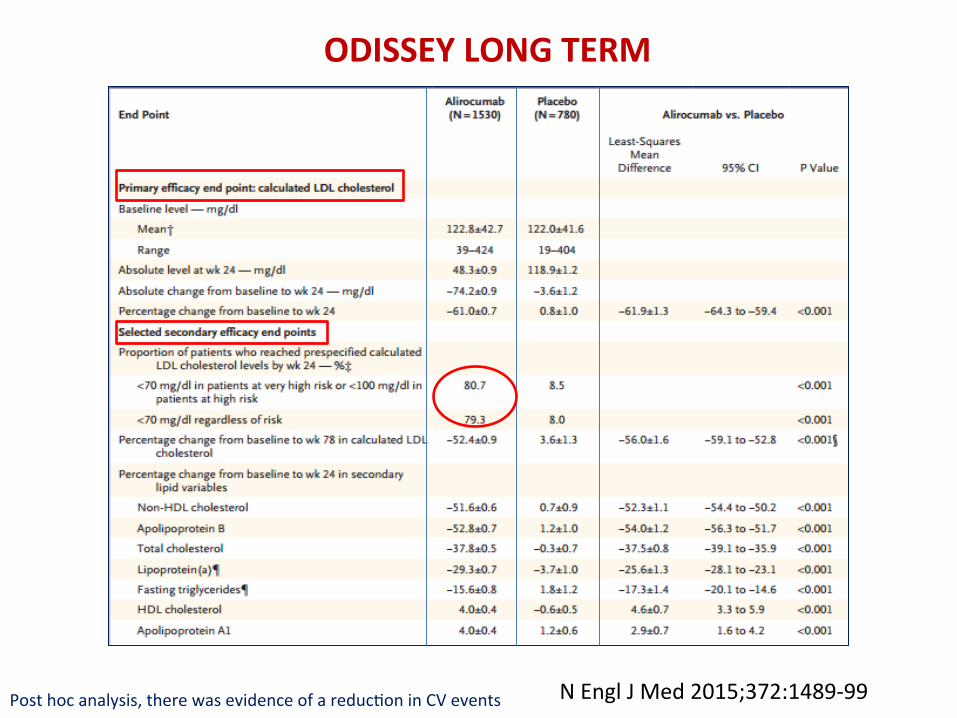
ODISSEY LONG TERM
Post hoc analysis, there was evidence of a reducJon in CV events N Engl J Med 2015;372:1489-‐99

ODISSEY LONG TERM
Post hoc analysis, there was evidence of a reducJon in CV events N Engl J Med 2015;372:1489-‐99

METANÁLISIS ANTI-‐PCSK9
Ann Intern Med. 2015;163(1):40-‐51
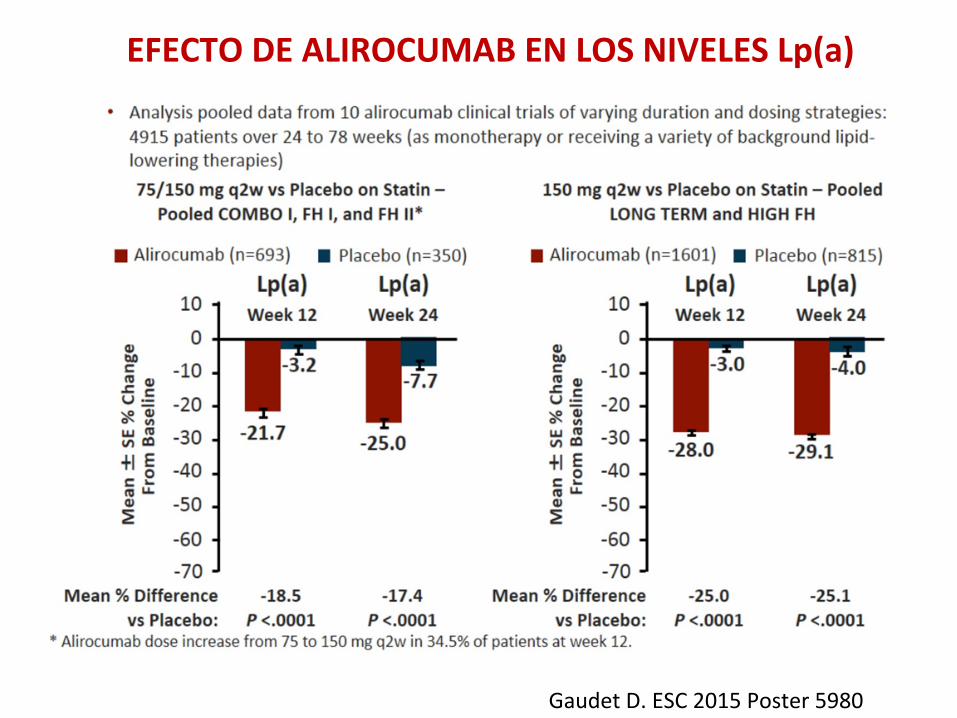
EFECTO DE ALIROCUMAB EN LOS NIVELES Lp(a)
Gaudet D. ESC 2015 Poster 5980
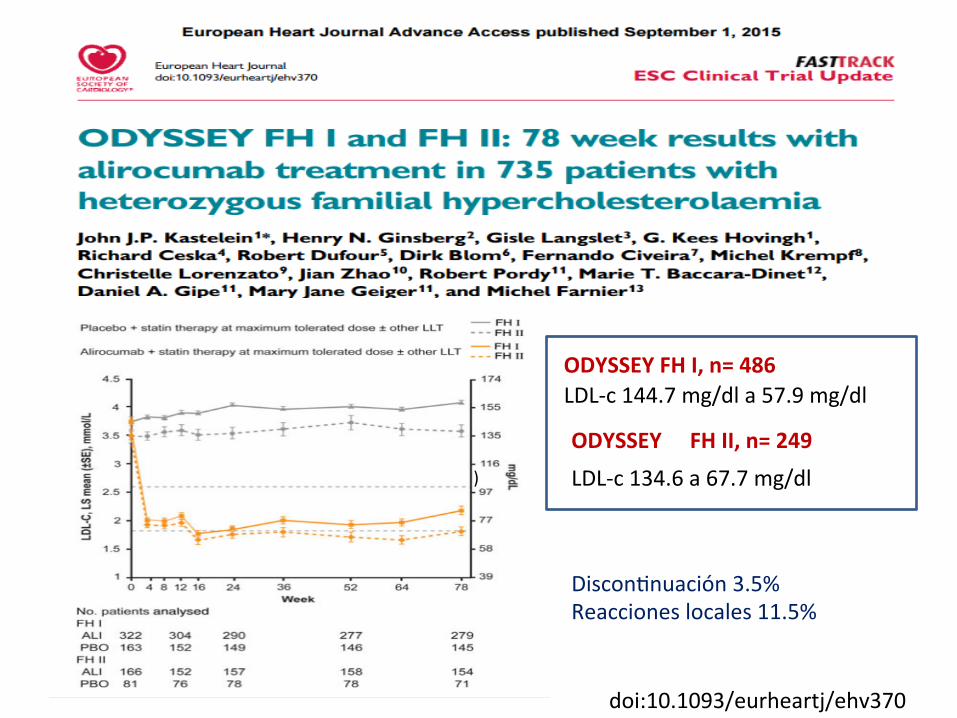
)
ODYSSEY FH I, n= 486 LDL-‐c 144.7 mg/dl a 57.9 mg/dl
FH II, n= 249 ODYSSEY LDL-‐c 134.6 a 67.7 mg/dl
DisconJnuación 3.5% Reacciones locales 11.5%
doi:10.1093/eurheartj/ehv370

INHIBIDORES PCSK9 OBJETIVOS CV
PARA DEMOSTRAR SI REDUCEN O NO LA MORBIMORTALIDAD CV

MONOTERAPIA
AÑADIDO A LA ESTATINA
INTOLERANTES A ESTATINAS
HIPERCOLESTEROLEMIA FAMILIAR
POSIBLES USOS CLÍNICOS INHIBIDORES PCSK9
EFICAC
ES
SEGURO
S A CORTO
PLAZO
INHIBIDORES PCSK9


RETOS INHIBIDORES PCSK9
Coste-‐efec@vidad Adherencia a las inyecciones
Seguridad a largo plazo Reducción de eventos CV


Robinson J et al InternaJonal Symposium on Atherosclerosis, Amsterdam 2015
LDL-‐C EXTREMADAMENTE BAJO

EVOLOCUMAB (Repatha, Amgen) ALIROCUMAB (Praluent, Sanofi /Regeneron), Both of which were approved by the US Food and Drug AdministraJon this summer, cost $14,100 and $14,600,
In Europe, evolocumab, the only agent approved by the European Commission, costs $6800 per year in the UK and $8200 and $8800 per year in Austria and Finland, respecJvely.
InsJtute for Clinical and Economic(ICER) Review. PCSK9 inhibitors for treatment of high cholesterol: effecJveness, value, and value-‐based price benchmarks drak report. Published September 8, 2015
COSTE EFECTIVIDAD
NO COSTE EFECTIVO AL PRECIO DE SALIDA

0
4
8
12
16
40 80 120 160
91.5 36 LDL-‐C mg/dl
10.2
7.5
26%
61%
Riesgo CV absoluto %
55%
iPCSK9 ESPECULANDO Disminución ECV

SEA 2016
Documento de consenso de la SEA (Sociedad Española de Arteriosclerosis) sobre las indicaciones de los
Inhibidores de PCSK9
MINISTERIO
>100
>100

FINANCIACIÓN I-‐PCSK9 EN ESPAÑA
IPT MS 2016
a) Pacientes con Hipercolesterolemia familiar homocigota (HFHo) no controlados (definido como C-‐LDL superior a 100 mg/dl) con la dosis máxima tolerada de estaJnas b) Pacientes con Hipercolesterolemia familiar heterocigota (HFHe) no controlados (definido como C-‐LDL superior a 100 mg/dl) con la dosis máxima tolerada de estaJnas c) Pacientes con enfermedad cardiovascular establecida (cardiopaya isquémica, enfermedad cerebrovascular isquémica y enfermedad arterial periférica) no controlados (definido como C-‐LDL superior a 100 mg/dl) con la dosis máxima tolerada de estaJnas d) Cualquiera de los pacientes de los grupos anteriores que sean intolerantes a las estaJnas o en los que las estaJnas están contraindicadas y cuyo C-‐LDL sea superior a 100 mg/dl.
INDICACIONES FINANCIADAS

PREVENCIÓN PRIMARIA
Perfil Clínico Nivel LDL-‐c(mg/dl) HF >130 Muy elevado >130 RCV
PREVENCIÓN SECUNDARIA
HF + CI >70 CI reciente >100 >12 meses CI estable >100 SCA/Reincidente >70 CI estable +SCA CI/Intolerantes En todos los EstaJnas/ pacientes con Contraindicación necesidad
Perfil Clínico Nivel LDL-‐c(mg/dl)
iPCSK-‐9 en PREVENCIÓN PRIMARIA Y SECUNDARIA
*TMO: EstaJna alta dosis/Alta potencia + EzeJmiba
*
Rev Esp Cardiol 2016 en prensa

J Am Coll Cardiol. Published online April 1, 2016.
2016 ACC EXPERT CONSENSUS DECISION PATHWAY FOR THE ROLE OF NON-‐STATIN THERAPIES FOR LDL-‐C LOWERING IN THE MANAGEMENT OF ASCVD RISK
Lloyd-‐Jones DM et al 2016 Lipid Pathway

2016 ACC Expert Consensus Decision Pathway Patient Populations Addressed: 4 Statin Benefit Groups
Adults ≥ 21 years of age with clinical ASCVD, on statin for secondary prevention
Adults ≥ 21 years of age with LDL-C ≥ 190 mg/dL (not due to secondary modifiable causes), on statin for primary prevention
Adults aged 40-75 years without ASCVD but with diabetes and LDL-C 70-189 mg/dL, on statin for primary prevention
Adults aged 40-75 years without clinical ASCVD or diabetes, with LDL-C 70-189 mg/dL and an estimated 10-year risk for ASCVD of ≥ 7.5%, on statin for primary prevention
Factors to Consider • Adherence and Lifestyle • Sta@n Intolerance • Control of other risk factors • Clinician-‐pa@ent discussion regarding poten@al benefits, poten@al harms, and pa@ent preferences regarding
addi@on of non-‐sta@n medica@ons • Percentage of LDL-‐C reduc@on (may consider absolute LDL-‐C level achieved) • Monitoring of response to therapy, adherence and lifestyle
Op@onal Interven@ons to Consider • Referral to lipid specialist • Eze@mibe • Bile Acid Sequestrants • PCSK9 inhibitors • Mipomersen, lomitapide, LDL apheresis may be considered by lipid specialist for pa@ents
with familial hypercholesterolemia
Special populaJons not included in 1 of the 4 staJn benefit groups were considered separately (e.g. heart failure, maintenance hemodialysis, women considering pregnancy or already pregnant)

EFECTOS LIPÍDICOS DE LOS INHIBIDORES/MODULADORES CETP
Cannon C et al. JAMA. 2011;306:2153-‐2155 Nicholls SJ et al. JAMA. 2011;306:2099-‐2109
TA 8995

LDL-‐c HDL-‐c
Lancet 2015; 385: 2153–61
204 p Anacetrapib vs 102p Placebo
52 semanas de seguimiento

LDL-‐c HDL-‐c
LDL-‐c disminuye 45·∙3% , apoB 33·∙7%, HDL-‐c aumenta 179·∙1%, apoA-‐I 63·∙4%. La capacidad de eflujo de colesterol se incrementa en 36·∙7% en pacientes asignados a 10 mg TA-‐8995
Lancet 2015; 386: 452–60
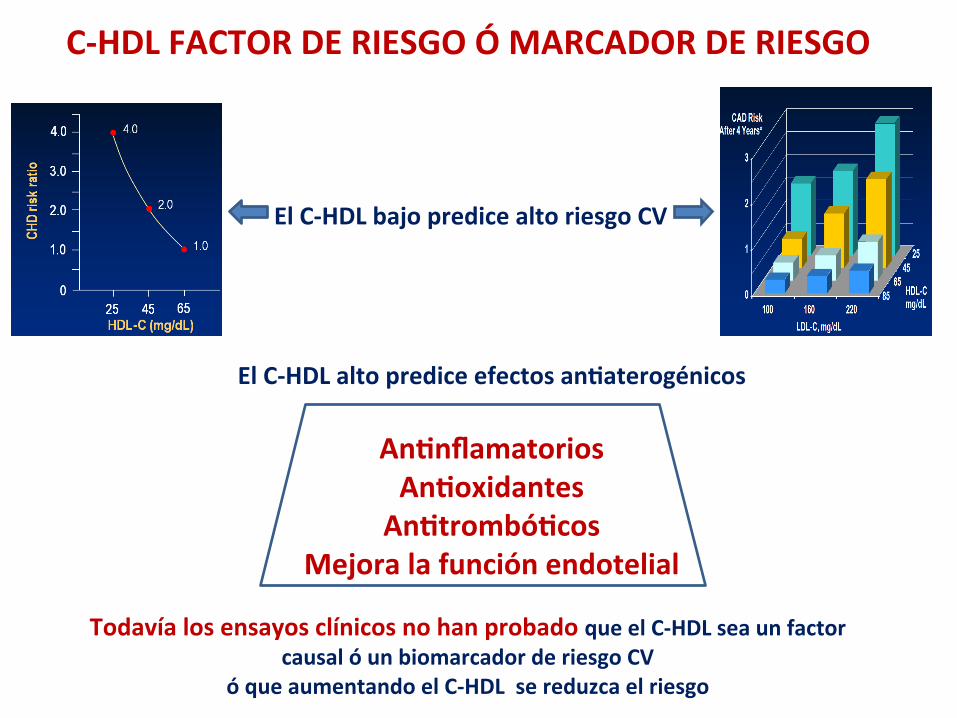
El C-‐HDL bajo predice alto riesgo CV
El C-‐HDL alto predice efectos an@aterogénicos
An@nflamatorios An@oxidantes An@trombó@cos
Mejora la función endotelial
Todavía los ensayos clínicos no han probado que el C-‐HDL sea un factor causal ó un biomarcador de riesgo CV
ó que aumentando el C-‐HDL se reduzca el riesgo
C-‐HDL FACTOR DE RIESGO Ó MARCADOR DE RIESGO

El C-‐HDL bajo predice alto riesgo CV :
El C-‐HDL alto predice efectos an@aterogénicos
An@nflamatorios An@oxidantes An@trombó@cos
Mejora la función endotelial
Todavía los ensayos clínicos no han probado que el C-‐HDL sea un factor causal ó un biomarcador de riesgo CV
ó que aumentando el C-‐HDL se reduzca el riesgo
C-‐HDL FACTOR DE RIESGO Ó MARCADOR DE RIESGO
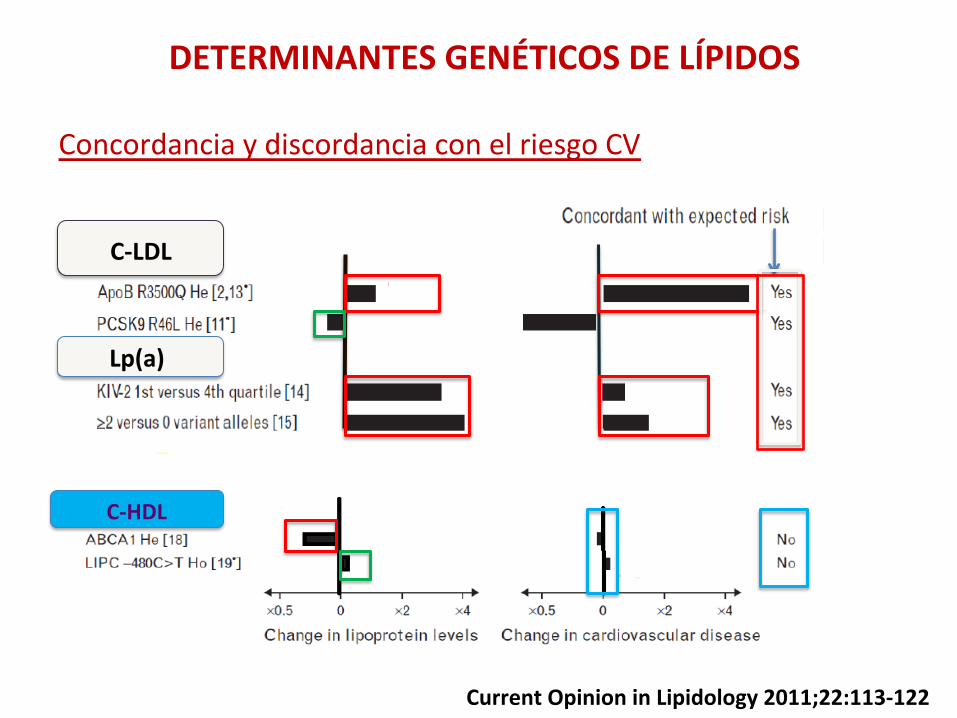
DETERMINANTES GENÉTICOS DE LÍPIDOS
Concordancia y discordancia con el riesgo CV
C-‐LDL
Lp(a)
C-‐HDL
Current Opinion in Lipidology 2011;22:113-‐122

CONCLUSIONES
1.-‐ ESTATINAS: Inmenso avance con limitaciones: potencia limitada, efectos secundarios, intolerancia, no alcance de objeJvos, pero seguirán siendo la base del tratamiento junto con ezeJmiba 2.-‐OBJETIVOS de LDL-‐c, la dura realidad: estamos lejos de alcanzar objeJvos en prácJca clínica de LDL-‐c en pacientes de alto riesgo, intolerantes a estaJnas y en HF 3.-‐INHIBIDORES DE PCSK9 la gran esperanza y ya realidad para alcanzar objeJvos : disminuyen con seguridad LDL-‐c hasta niveles desconocidos hasta ahora y permiten a alcanzar objeJvos y muy probablemente mejoren la morbimortalidad CV 4.-‐NIVELES bajos de LDL-‐c alcanzados con la combinación estaJna –ezeJmiba son seguros a medio-‐largo plazo y niveles muy bajos de LDL-‐c con inhibidores de PCSK9 son seguros a corto plazo y no se asocian a mayores efectos secundarios

CUANTO MÁS BAJO MEJOR
REDUCIR MORBIMORTALIDAD CV CON SEGURIDAD
Con todo Jpo de medidas y tratamientos que demuestren
CUANTO ANTES MEJOR
LDL-‐COLESTEROL


















