Pakistan Journal ofpjnm.net/uploads/3/5/2/5/35254390/pjnm7-draft_14_jan_2018_online_copy.pdf ·...
74
7
Transcript of Pakistan Journal ofpjnm.net/uploads/3/5/2/5/35254390/pjnm7-draft_14_jan_2018_online_copy.pdf ·...

7
Official journal of Pakistan Society of Nuclear Medicine
Qaisar Hussain Siraj
Dr Khalid NawazDr Ahmad QureshyDr Abida RazaDr Shoaib ShahDr Aakif Ullah Khan
Dr Maseeh uz ZamanDr Akhtar AhmedDr M Babar ImranDr Sadiq Hussain Nohario
Pakistan Journal ofNuclear Medicine
Prof Seyed Rasoul Zakavi, IranProf A H Elzaggar, KuwaitProf G T Krishnamurthy, USAProf Hee-Seung Bom, S KoreaDr John R Buscombe, UKDr Frederic Fahey, USAProf Richard Underwood, UK
Prof Giuliano Mariani, ItalyDr G M Shah, Saudi ArabiaDr Thomas Pascal, PhilippinesProf Ali Nawaz Khan, UKDr Michael Masoomi, UKDr Jamshed B Bomanji, UKProf A J B McEwan, Canada
Dr Humayun BashirDr Saima HaiderDr Nasir MahmoodDr H Ghulam AbbasDr Mujahid Khalid AliDr Riffat HussainDr Syed Shahid IqbalDr Shahab Fatimi
Dr Mohsin Saeed SheikhDr Amjad Aziz KhanDr M Numair YounisMr Asdar ul HaqMr Farrukh HameedDr M Adnan SaeedDr Saima Riaz
PJNMMohammad Sohaib
Qaisar Hussain SirajDurr-e-Sabih
Al-Rowaily MH, Dondi D, Chinol M, Munir I, Alasbahi MA. A brief review oftargetted radionuclide therapies. Pak J Nucl Med 2017;7:1-7.
Dong X, Saripan MI, Mahmud R, Mashohor S, Wang A. Determination of theoptimum filter for 99mTc SPECT breast imaging using a wire mesh collimator. PakJ Nucl Med 2017;7:8-17.
Javed M, Saeed-Ur-Rahman, Tanveer I, Asghar G, Fatima S, Fahim M.Measurement of radiation doses to occupational workers in nuclear medicine.Pak J Nucl Med 2017;7:18-23.
Memon SA, Laghari NA, Mangi FH. Behaviour of wedges for different field sizesand depths. Pak J Nucl Med 2017;7:24-33.
Munir I, Javaid A, Nawaz K, Al-Rowaily MH, Al-Asbahi MA. Pre-operative cardiacrisk stratification for non-cardiac surgery in cancer patients using myocardialperfusion scintigraphy. Pak J Nucl Med 2017;7:34-42.
Butt ST, Fatima S, Marwat N, Mir K, Ammar A, Faheem M. Clinical characteristicsand long-term outcome of patients with differentiated carcinoma of thyroid withbone metastases: a retrospective study. Pak J Nucl Med 2017;7:43-47.
Kochetova T, Krylov V. Successful Ra-223 treatment with a long interval betweenthe second and the third cycles: a case report. Pak J Nucl Med 2017;7:48-52.
Siraj QH. Cutaneous flow pattern of primary lymphoedema. Pak J Nucl Med2017;7:53-55.
Siraj QH. Bone scintigraphy in apatite-associated destructive arthritis (Milwaukeeshoulder syndrome). Pak J Nucl Med 2017;7:56-61.
Siraj QH, Javaid A, Rasulova N. A striking case of florid multifacial soft-tissueinfection on an FDG-PET scan. Pak J Nucl Med 2017;7:62-65.
Benameur Y, Guerrouj H, Oueriagli SN, Sahel OA, Ghfir I, Aouad NBR. Unusualbreast radioiodine uptake in a non- breastfeeding woman with papillary thyroidcarcinoma. Pak J Nucl Med 2017;7:66-68.
PJNM Pakistan Journal ofNuclear Medicine
A brief review of targetted radionuclidetherapies
Mohammed Hathaf Al-Rowaily*,1, Daniele Dondi1, MarcoChinol2, Iqbal Munir3, Muaadh Abdualrehman Alasbahi3
1Department of Chemistry, Pavia University, Italy2European Institute of Oncology, Italy
3Department of Nuclear Medicine, Dr. Suleiman Al-HabibMedical Group, Riyadh, KSA
REVIEW ARTICLE
*Correspondence
Mohammed Hathaf Al Rowaily Department of Chemistry Pavia University Italy Email: [email protected]
Abstract
Personalized medicine is an emerging medicalfield. Targetted radionuclide therapies forbenign and malignant diseases have been inuse since 1945. Over the last 20 years due toadvancements in the nanotechnology andtargetting cell receptors, radionuclidetherapies have emerged as a subspecialty ofnuclear medicine. Through this article wewould like to briefly describe the evolution ofradionuclide therapies and their differentclinical applications as personalized medicine.
Key words: Radionuclide therapy, 131I-metaiodobenylguanidine therapy, CD-20targeted therapies, radioembolization,metastatic bone pain palliation
Introduction
Radiotherapy techniques have provedimportant in treating as well as prolonging the
patients' lives depending on the type of cancerin question. However, the success of thesetechniques is limited by their lack of specificityas the anti-cancer agents or cytotoxictechnologies do no distinguish between thecancerous regions and the normal tissues [1].Most of the traditionally used radiotherapytechniques apply a non-discriminatorydestruction of the cells exhibiting uncontrolledgrowth without any degree of selection leadingto the destruction of the healthy cells. Unlikeexternal radiotherapy which damages cells'DNA with the aim of killing those withuncontrolled growth, targetted radionuclidetherapy offers a systemic treatment bydelivering toxic levels of radiolabelledmolecules to the target sites for a highlyselective destruction of the site [2].Radionuclide therapy acts the same way aschemotherapy by targetting specific cells, butit is more advanced in that radionuclides alsokill tumour cells lacking tumour-specificreceptors and thus it has ability for direct aswell as a bystander effect which ultimatelykills the tumour cells. The biological effect oftargetted radionuclide therapy results fromenergy absorption of radiation emitted by theradionuclide. After the first description ofradioimmunotherapy by Korngold andPressman in 1953, numerous radio-pharmaceuticals have been developed byadvanced techniques in genetic engineering
PJNM 2017, 7:1-7 331691 © 2017 Pakistan Society of Nuclear Medicine
www.pjnm.net 2305-1630(201701/01)7:1<01:BROTRT>2.0.TX;2-M

PJNM 2017, Volume 7, Number 1 2
and chelating techniques [3]. Targettedradiotherapy involves the utilization of threeparticulate particles, which are capable ofirradiating tissue volumes with subcellular,cellular and multicellular dimensions. Theseparticles include Auger electrons, alphaparticles, and beta particles.
Auger electrons and Auger-electron-emittingradionuclides
Auger electrons are particles released by someelements in a phenomenon referred to as theAuger effect. In this phenomenon, an atomemits an electron after filling an inner-shellvacancy resulting in energy release. Some ofthe current available or prospective Augerelectron emitters include indium-111, iodine-125, iodine-123, and bromine-77. Theseradionuclides can be used alongside targettingvehicles to localize sub-cellar radiations nearthe cellular DNA leading to an effective and aspecific killing of the tumour cells. Usingauger-emitting radionuclide therapeutics,highly tailored targetted radiotherapeuticscould be engineered to fit the specific needs ofa cancer patient [4].
Beta particles and beta-emitting radionuclides
Beta particles are fast-moving electronsemitted by the nucleus during radioactivedecay. Some of the currently approved beta-emitting radionuclides used in radiotherapyinclude yttrium-90 and iodine-131 (for non-Hodgkin's lymphoma treatment), strontium-89-chloride and samarium-153-EDTMP (forbone metastases). Other potential beta-emitting radionuclides include rhodium-105,gold-199, copper-67, rhenium-186, andlutetium-177 amongst others. The majoradvantage of beta particles is that they haveminimal tissue penetration. These particles areemitted at high speed, but they become rapidlyattenuated by biological tissues. As a result,when administered as a radiopharmaceuticalit does not affect the surrounding tissues as itcannot travel beyond specific range within abiological structure. An additional protection
of the un-targetted tissue is also achieved byradioimmuno targetted therapy [4].
Alpha particles and alpha-emitting radionuclides
Alpha particles comprise of two protons as wellas two neutrons, and they are identical tohelium atom's nucleus. Alpha-emittingradionuclides emit particles of only a few celldiameters in tissue. One of the advantages ofalpha particles is that they have a high linearenergy transfer that makes them morebiologically effective as compared to theconventional radiotherapy techniques. In thisvein, fewer alpha particles are capable of killinghuman cancer cells. Some of the availableradionuclides that emit alpha particles includeradium-223, astatine-211, and bismuth-2013.Alpha particles are preferred for radiotherapyfor their ability to deliver lethal radiation,within a range of 50-90 µm in diameter. Thisallows the emitter to specifically targetcancerous tissue without destroying theadjacent healthy tissues. Alpha particles offera therapeutic benefit by breaking the DNAdouble strand and thus breaking the cell cycle.Also, these particles cause chromosomalinstability in the nearby cells leading to abystander effect as observed in radiotherapy[4].
Radionuclides as therapeutics
Radionuclides used in cancer treatment releaseenergy in the form of beta particles, Augerelectrons or alpha particles to cause thedestruction of cancer cells and result inimprovement of the patient's condition. Theradionuclides applied for the purposes oftreating cancer depend on several factors,including: the nuclear emission properties,mode of radioactive decay, physical half-life,radionuclide production route, pharmacologicalfeatures of the resultant radio-conjugate,radiation type and its energy, and the stabilityof the resultant daughter nuclides. Most of thecancer-destroying radionuclides have aphysical half-life of between 10 hours to 10days allowing them to deposit a large radiation
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:1-7
PJNM 2017, Volume 7, Number 1 3
dose. They also emit high LET radiation nearthe target cancer tissue and their daughternuclides are stable and long-lived to increasethe therapeutic effect of the radionuclide [5].
Clinical Applications
Iodine-131 and thyroid cancer treatment
Iodine-131 is highly radioactive and has ahalf-life of 8.02 days, and when used in smalldoses it is used in cancer treatment. Wheniodine-131 is taken orally, it crosses thegastrointestinal wall, and is concentrated inthe thyroid gland where it decays into xenon-131, with the release of gamma radiations andbeta particles.
On the global scale, the use of radioactiveiodine in differentiated thyroid cancertreatment has been the most common and theoldest targetted radiotherapy. The aim of theuse of iodine-131 in differentiated thyroidcancer treatment is to destroy cancer cells inorder to ablate the remnant thyroid tissue inorder to optimise follow-up and reduce cancerrecurrence rate [6]. The significance ofradioactive iodine treatment in targettedradiotherapy is derived from the ability of boththe follicular and the papillary cancers toexpress sodium iodide symporter forradioactive iodine uptake by cancer cells. Lowdoses of radioactive iodine have high levels ofefficacies as well as high safety profiles makingit the most acceptable thyroid cancermanagement modality across the world.Furthermore, the disintegration of therespective radionuclides results in additionalcytotoxic effects on the target cells [7].
Neuroblastoma/neuroendocrine tumours and131I-metaiodobenylguanidine
Since the 1980s, treatment of neuroendocrinetumours have been treated using 131I-metaiodobenylguanidine (131I-MIBG) becauseof its high efficacy in treating chromaffin celltumours (paraganglioma, pheochromocytoma,and neuroblastoma).
131I-MIBG uptake happens in a similar versionto noradrenaline and increases after catechol-amine excretion or adrenergic innervation.Stage III and IV patients with neuroblastomaare difficult to manage via chemotherapy andsurgery and most cases resort to theadministration of 131I-MIBG to control tumourgrowth as well as for symptom relief [8]. Amanagement plan for neuroblastoma using131I-MIBG involves taking the patient througha series of studies including tissue biopsies,MRI/CT studies, ultrasonography, 123I-MIBGscintigraphy and FDG-PET/CT before thecommencement of 131I-MIBG therapy. Moreover,recommendations point that 131I-MIBG infusionshould last for longer than one hour in orderto avoid metaiodobenylguanidine side effects.131I-MIBG may also be used for the treatmentof other similar tumours such as paraganglioma,pheochromocytoma, medullary thyroid cancer,and carcinoid tumours. These tumours have aresponse rate of 30-75%, indicating highefficacies [9].
Targetted radionuclide therapy and lymphomatreatment
In the 2000s, two major targeted radionuclidetherapeutic agents were introduced forlymphoma treatment to reduce the number ofdeaths resulting from low-grade lymphomathat is difficult to treat with chemotherapytechniques. These agents include I-131tositumomab and Y-90 ibritumomabtiuxetanand they have been demonstrated to yield50-80 percent response rates. I-131tositumomab has an IgG2a murine anti-CD20antibody (tositumomab), while Y-90ibritumomabtiuxetan has murine IgG1 anti-CD20 antibody (ibritumomab), the differencebetween the two agents is their differentiallinkage to the radionuclide [10]. By targetingCD20 antigens, these agents deliver therespective radionuclides mature B-lymphocytes, pre-B lymphocytes, and B-cellnon-Hodgkin's lymphoma, and thus it ends upinducing apoptosis, antibody-dependentcytotoxicity, and complement-dependentcytotoxicity after the formation of theantibody-antigen immune complex [11].
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:1-7
PJNM 2017, Volume 7, Number 1 4
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:1-7
Yttrium-90 and liver tumours treatment
Such metastatic tumours as pancreatic carcinoma,colorectal carcinoma, neuroendocrine tumoursand breast cancers also occur in the liver aftermetastases leading to a fatal pathologicalburden. However, reduction of the burden isachieved through traditional therapies with anadditional administration of Y-90 microspheresfor radioembolization. Radioembolization ofthe liver cancers with Y-90 microspheresgenerate between 27 and 100 percentresponse rates in clinical treatments [12].
Palliation of metastatic bone pain
During advanced stages of cancers, bone painreduces the quality of life of the cancer patientto a significant extent. However, the administrationof radiopharmaceuticals can palliate pain frommetastatic processes. Some of the approvedmetastatic pain palliation radiopharmaceuticalsinclude 186Re-etidronate, 153Sm-lexidronamand 89Sr-chloride; their administrations resultin high concentrations in bones leading toeffective pain management [13].
Application of radionuclide targeted therapy inhaematological malignancies
The type of radionuclide targetted therapyapplied on a specific type of cancer isdependent on the type of malignancy inquestion. As a result, haematologicalmalignancies require a different type oftargetted radionuclide therapy from the oneused for the solid tumours. In haematologicalmalignancies, targetted radionuclide therapyis supported by three major factors. One ofthe reasons for the effectiveness of targettedradionuclide therapy is the expression ofspecific surface antigens by most cancer celllines [14]. These antigens are absent fromother tissues in the organism and thus makingtargetted therapies possible. Another reasonfor the effectiveness of this approach is therich availability of the high-quality antibodiesagainst antigens expressed by haematologicaltissues. Moreover, the effectiveness of thisapproach is also made possible by the high
sensitivity of lymphomas and leukemias toionizing radiation. In addition, theeffectiveness of the targetted radionuclidetherapy is also increased by the availability ofbone marrow transplantation technologies thatallow for the replenishment of thehaematological stem cells after the treatmentof haematological malignancies with high doseradionuclides. Some of the target antigens intargeted radionuclide treatment ofhaematological malignancies include CD45,CD66, CD33, CD5, CD25, and the mostcommonly targeted CD20. 90Y and 131I havethe greatest potential for application asradionuclides in targeted radionuclide therapy.Moreover, some of the commonhaematological tumours treated usingtargetted radionuclide therapy includes T-cellleukemias, chronic lymphocytic leukemia, andHodgkin's lymphoma [15].
Application of radionuclide targeted therapy insolid malignancies
Unlike the treatment of haematologicaltumours with targetted radionuclides which ishighly efficacious, the treatment of solidtumours has low efficacies and is thuschallenging. This challenge is presented by theinability of the ionising particles to penetratethe tumour body leading to their localizationin the periphery as well as low doses in thetumour parenchyma. In targetted radionuclidetherapy of solid tumours, the cells lying onthe surface of the tumour body have the samestructure and function and as a result, theirdestruction does not always result in thecomplete destruction of the tumour. Besides,the conditions inside of the tumour are hypoxicand do not permit the formation of reactiveoxygen species which increases the damagingpotential of the therapeutic agent. However,this problem can be addressed by the use ofmulti-step pre-targetted radionuclide therapy,which enhances exposure to tumour radiationand therapeutic selectivity [16].
Some of the successful applications of targettedradionuclide therapy of solid tumours includecolorectal carcinoma, solid neuroendocrinemalignancies, castration-resistant prostate

PJNM 2017, Volume 7, Number 1 5
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:1-7
cancer, metastasizing melanoma, pancreatictumour and stage-IV melanoma, amongstothers. The treatment of colorectal carcinomainvolves the use of I-131-conjugated anti-CEAantibodies, and it produces up to 68 monthsmedian survival time. The application of anti-PSMA antigen antibodies with Lu-177radionuclides offer a successful treatment ofcastration-resistant prostate cancer producesa successful therapy with a median survivaltime of 10 months, while the application ofanti-NG2 with Bi-213 produces a long-lastingeffect in stage IV melanoma treatment. Forthe metastatic melanoma, the survival timeincreases by nine months after administrationof anti-NG2 antibodies conjugated to Bi-213radionuclide, but the application of DOTATE inconjugation with Lu-177 produces acomplication-free stable disease course in 46percent cases [17].
Advantages and disadvantages of targettedradionuclide therapy
One of the advantages of targettedradionuclide therapy is that Auger electron,alpha particle, and beta particle emitters areeffective therapeutic particles as they canlocalize the delivery of cytotoxic ionizingradiation [18]. By linking the emitters tobiological agents, localized treatment can beachieved because of the high affinity of someelements for some organs and organ systems.As a result, the therapeutic capability of theseagents provides a localized killing of specifictissues and cells. Another advantage of theapplication of targetted radionuclides in cancertherapy is their large-scale availability [19].Once a specific radionuclide is approved foruse as a radiopharmaceutical, it becomessubject to large-scale production in thelaboratory making it readily available for awide scale application. Another advantage oftargetted radionuclide therapy is a highspecificity and selectivity for the target celltypes [20]. Targetted radionuclides are linkedto such biological components as antibodieswhich are specific for certain receptorsexpressed on cancer cells. As a result, whenintroduced into the body they become attachedto the target cells where radionuclides decay
to emit beta particles, alpha particles or Augerelectrons, which kill the antibody-associatedcancer cells. The mechanism leads to aselective killing of the tumour [21].
On the other hand, this therapeutic techniquecarries several significant disadvantages whichlimits its application in treating humans. Oneof the disadvantages of targetted radionuclidetherapy is the shortage of radionuclides. Forexample, iodine-124, zirconium-89, astantine-89, bromine-77 and copper-67 are in shortsupply because of their high requirements ofhigh-energy/complexity accelerators forproduction and this limits their availability incontrast to radionuclides produced by the smallcyclotrons in PET centres. This limitation ofradionuclide supply also limits theadvancement of research and development inradiobiology and radiochemistry. Amongstthose listed above, only yttrium-90 and iodine-131 are available for clinical use, but theiravailability is low. Another disadvantage oftargetted radionuclide therapy is resistance.By being a biologically determined process,targetted radionuclide therapy is limited byresistance because some tumours might lackthe receptor subtype leading to the inability tooffer effective treatment. For example, atumour may exhibit a variant subtype ofsomatostatin receptors leading to resistanceto somatostatin-active radionuclides. Anotherlimitation is a mutation that can lead toresistance as well. For example, mutation ofsomatostatin genes will result in loss of efficacyof somatostatin-targetted radionuclides [22].
Conclusion
Traditionally, radiotherapy has been utilized forcancer treatment to suppress and kill thecancerous cells. There are several disadvantagesof this techniques including the unnecessary sideeffects and killing of the normal cells. Targetedradionuclide therapies are emerging aspersonalized medicine targeting only thereceptor specific defective cells leading tominimize the side effect of the treatment alongwith maximizing the efficacy. This mainadvantage makes this as a treatment of choicefor the patients in which it has proven benefits
PJNM 2017, Volume 7, Number 1 6
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:1-7
benefits over the conventional treatment. Weare hopeful that with upcoming research thismay well be the future direction of medicine.
References
1. Flux G, Bardies M, Monsieurs M, SavolainenS, Strand S-E, Lassmann M. The impact ofPET and SPECT on dosimetry for targetedradionuclide therapy. Z Med Phys.2006;16:47-59.
2. Boyd M, Ross SC, Dorrens J, Fullerton NE,Tan KW, Zalutsky MR, et al. Radiation-induced biological bystander effect elicitedin vitro by targeted radiopharmaceuticalslabelled with ?-, ?-, and Auger electron-emitting radionuclides. J Nucl Med.2006;47:1007-15.
3. Dale R, Carabe-Fernandez A. Theradiobiology of conventional radiotherapyand its application to radionuclide therapy.Cancer Biother Radiopharm. 2005;20:47-51.
4. Larson SM, Krenning EP. A pragmaticperspective on molecular targetedradionuclide therapy. J Nucl Med. 2005;46Suppl 1:1S-3S.
5. Goldenberg DM. Advancing role ofradiolabeled antibodies in the therapy ofcancer. Cancer Immunol Immunother.2003;52:281-296.
6. Schlumberger MJ. Papillary and follicularthyroid carcinoma. N Engl J Med.1998;338:297-306.
7. Mazzaferri EL, Jhiang SM. Long-termimpact of initial surgical and medicaltherapy on papillary and follicular thyroidcancer. Am J Med. 1994;97:418-28.
8. Matthay KK, Tan JC, Villablanca JG, Yanik GA,Veatch J, Franc B, et al. Phase I dose escalationof iodine-131-metaiodobenzylguanidine withmyeloablative chemotherapy and autologousstem-cell transplantation in refractory neuro-
blastoma: a new approaches toNeuroblastoma Therapy Consortium Study.J Clin Oncol 2006;24:500-6.
9. Meller S. Targeted radiotherapy forneuroblastoma. Arch Dis Child.1997;77:389-91.
10. Wiseman GA, White CA, Sparks RB, ErwinWD, Podoloff DA, Lamonica D, et al.Biodistribution and dosimetry results froma phase III prospectively randomizedcontrolled trial of Zevalinradioimmunotherapy for low-grade,follicular, or transformed B-cell non-Hodgkin's lymphoma. Crit Rev OncolHematol. 2001;39:181-94.
11. de Jong M, Krenning EP. New advances inpeptide receptor radionuclide therapy. JNucl Med. 2002;43:617-20.
12. Vogel CA, Galmiche MC, Buchegger F.Radioimmunotherapy and fractionatedradiotherapy of human colon cancer livermetastases in nude mice. Cancer Res.1997;57:447-453.
13. Srivastava SC, Atkins HL, KrishnamurthyGT, et al. Treatment of metastatic bone painwith tin-117m stannicdiethylenetriaminepentaacetic acid: a phaseI/II clinical study. Clin Cancer Res.1998;4:61-68.
14. Faderl S, Coutre S, Byrd JC, Dearden C,Denes A, Dyer MJ, et al. The evolving roleof alemtuzumab in management of patientswith CLL. Leukemia. 2005;19:2147-2152.
15. Linden O, Hindorf C, Cavallin-Stahl E,Wegener WA, Goldenberg DM, Horne H, etal. Dose-fractionated radioimmunotherapyin non-Hodgkin's lymphoma using DOTA-conjugated, 90Y-radiolabeled, humanizedanti-CD22 monoclonal antibody,epratuzumab. Clin Cancer Res.2005;11:5215-22.
16. Brouwers AH, Buijs WC, Mulders PF, de
PJNM 2017, Volume 7, Number 1 7
Pak J Nucl Med 2017;7:1-7 2305-1630(201701/01)7:1<01:BROTRT>2.0.TX;2-M
Mulder PH, van den Broek WJ, Mala C, etal. Radioimmunotherapy with [131I]cG250in patients with metastasized renal cellcancer: dosimetric analysis andimmunologic response. Clin Cancer Res.2005;11:7178s-86s.
17. Brouwers AH, Buijs WC, Mulders PF, deMulder PH, van den Broek WJ, Mala C, etal. Radioimmunotherapy with [131I]cG250in patients with metastasized renal cellcancer: dosimetric analysis andimmunologic response. Clin Cancer Res.2005;11:7178s-86s.
18. Bodei L, Cremonesi M, Grana C, Rocca P,Bartolomei M, Chinol M, et al. Receptorradionuclide therapy with 90Y-[DOTA]0-Tyr3-octreotide (90Y-DOTATOC) inneuroendocrine tumours. Eur J Nucl MedMol Imaging. 2004;31:1038-46.
19. Nicholson S, Gooden CS, Hird V, MaraveyasA, Mason P, Lambert HE, et al.Radioimmunotherapy after chemotherapycompared to chemotherapy alone in thetreatment of advanced ovarian cancer: amatched analysis. Oncol Rep. 1998;5:223-6.
20. Bernhardt P, Forssell-Aronsson E,Jacobsson L, Skarnemark G. Low-energyelectron emitters for targeted radiotherapyof small tumours. Acta Oncol.2001;40:602-608.
21. Sisson JC. Radiopharmaceuticals fornuclear endocrinology at the University ofMichigan. Cancer Biother Radiopharm.2000;15:305-318
22. Forrer F, Uusijarvi H, Waldherr C,Cremonesi M, Bernhardt P, Mueller-BrandJ, et al. A comparison of 111In-DOTATOCand 111In-DOTATATE: biodistribution anddosimetry in the same patients withmetastatic neuroendocrine tumours. Eur JNucl Med Mol Imaging. 2004;31:1257-62.
Determination of the optimum filter for 99mTcSPECT breast imaging using a wire mesh
collimator
Xianling Dong1,2,*, M.I. Saripan3, R. Mahmud4,S. Mashohor3, Aihui Wang5
1Insititute of Advanced Technology, Universiti Putra Malaysia,Serdang, Malaysia
2Department of Biomedical Engineering, ChengdeMedical University, China
3Faculty of Engineering, Universiti Putra Malaysia, Serdang, Malaysia4Faculty of Medicine and Sciences, Universiti Putra Malaysia,
Serdang, Malaysia5Department of Nuclear Medicine, Affiliated Hospital,
Chengde Medical University, China
ORIGINAL ARTICLE
*Correspondence Dong Xianling Insititute of Advanced Technology Universiti Putra Malaysia 43300 Sri Serdang, Selangor, Malaysia Email: [email protected]
Abstract
Aims The development of wire mesh collimator(WMC), has improved the performance ofSingle Photon Emission Computed tomography(SPECT) because of its higher sensitivity whilstmaintaining the same resolution. Consequently,the WMC allows better detection of early-stagecancer. The purpose of this study was to findan optimal filter for image reconstruction forbreast SPECT imaging.
Methods Half-ellipsoidal breast phantom inthe prone position was simulated withdual-head SPECT camera by Monte Carlo
N-Particle Transport Code, version 5 (MCNP5).Six different filters were compared with 17different cutoff frequencies (Fc), ranging from0.2 Nyquist frequency (Nq) to 1.0 Nq, withstep 0.05. For Butterworth filter, order wasfrom 3 to 12 with step 1. A total of 255 centralslices with different parameters werereconstructed by filtered back projection (FBP)to compare the image performance in termsof contrast, noise level and tumour size.
Results The values of tumour size, contrastand noise level were greatly influenced bydifferent filter types and the value of Fc. Rampand Butterworth produced the best value oftumour size and contrast, whilst Parzen, Hannand Hamming filters gave smoother images.Overall, results showed that Butterworth filterwith the highest mean score.
Conclusion Butterworth filter proved to bethe provided the best image quality at a highersensitivity and was found to be the optimumfilter for quantitative analysis.
PJNM 2017, 7:8-17 331691 © 2017 Pakistan Society of Nuclear Medicine
www.pjnm.net 2305-1630(201701/01)7:1<8:DOFTSB>2.0.TX;2-M
PJNM 2017, Volume 7, Number 1 9
Key words: Wire mesh collimator, SPECTbreast imaging, filtering, Cut-off frequency
Introduction
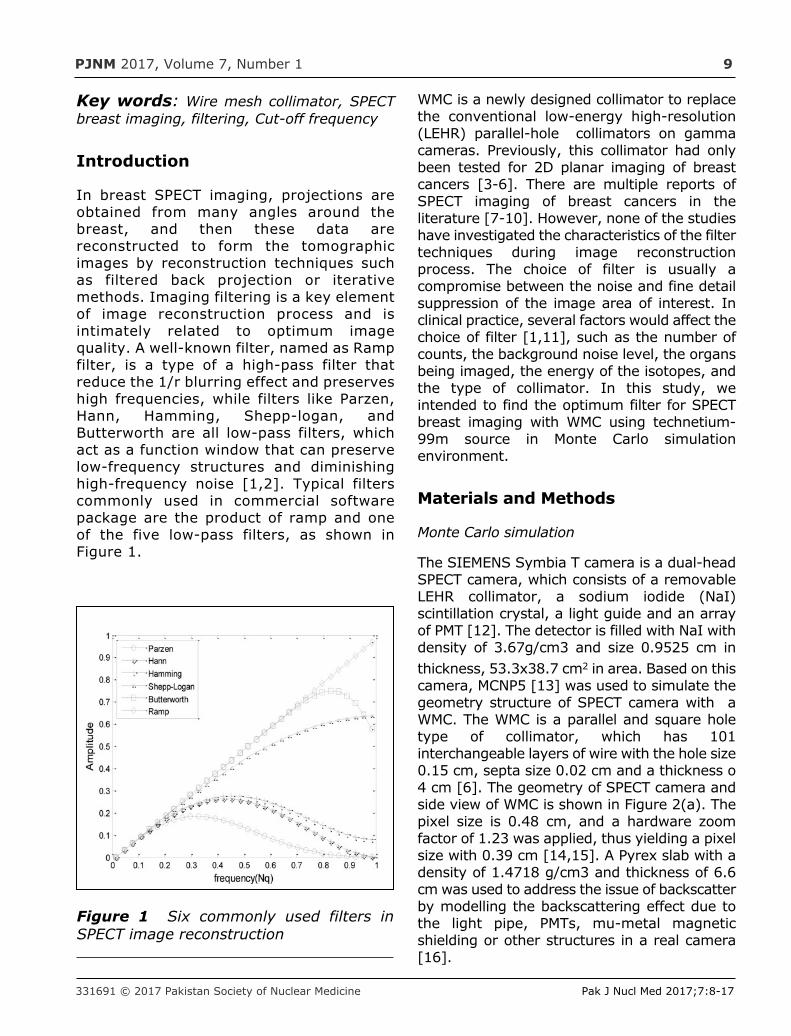
In breast SPECT imaging, projections areobtained from many angles around thebreast, and then these data arereconstructed to form the tomographicimages by reconstruction techniques suchas filtered back projection or iterativemethods. Imaging filtering is a key elementof image reconstruction process and isintimately related to optimum imagequality. A well-known filter, named as Rampfilter, is a type of a high-pass filter thatreduce the 1/r blurring effect and preserveshigh frequencies, while filters like Parzen,Hann, Hamming, Shepp-logan, andButterworth are all low-pass filters, whichact as a function window that can preservelow-frequency structures and diminishinghigh-frequency noise [1,2]. Typical filterscommonly used in commercial softwarepackage are the product of ramp and oneof the five low-pass filters, as shown inFigure 1.
WMC is a newly designed collimator to replacethe conventional low-energy high-resolution(LEHR) parallel-hole collimators on gammacameras. Previously, this collimator had onlybeen tested for 2D planar imaging of breastcancers [3-6]. There are multiple reports ofSPECT imaging of breast cancers in theliterature [7-10]. However, none of the studieshave investigated the characteristics of the filtertechniques during image reconstructionprocess. The choice of filter is usually acompromise between the noise and fine detailsuppression of the image area of interest. Inclinical practice, several factors would affect thechoice of filter [1,11], such as the number ofcounts, the background noise level, the organsbeing imaged, the energy of the isotopes, andthe type of collimator. In this study, weintended to find the optimum filter for SPECTbreast imaging with WMC using technetium-99m source in Monte Carlo simulationenvironment.
Materials and Methods
Monte Carlo simulation
The SIEMENS Symbia T camera is a dual-headSPECT camera, which consists of a removableLEHR collimator, a sodium iodide (NaI)scintillation crystal, a light guide and an arrayof PMT [12]. The detector is filled with NaI withdensity of 3.67g/cm3 and size 0.9525 cm inthickness, 53.3x38.7 cm2 in area. Based on thiscamera, MCNP5 [13] was used to simulate thegeometry structure of SPECT camera with aWMC. The WMC is a parallel and square holetype of collimator, which has 101interchangeable layers of wire with the hole size0.15 cm, septa size 0.02 cm and a thickness o4 cm [6]. The geometry of SPECT camera andside view of WMC is shown in Figure 2(a). Thepixel size is 0.48 cm, and a hardware zoomfactor of 1.23 was applied, thus yielding a pixelsize with 0.39 cm [14,15]. A Pyrex slab with adensity of 1.4718 g/cm3 and thickness of 6.6cm was used to address the issue of backscatterby modelling the backscattering effect due tothe light pipe, PMTs, mu-metal magneticshielding or other structures in a real camera[16].
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
Figure 1 Six commonly used filters inSPECT image reconstruction
PJNM 2016, Volume 6, Number 1 10
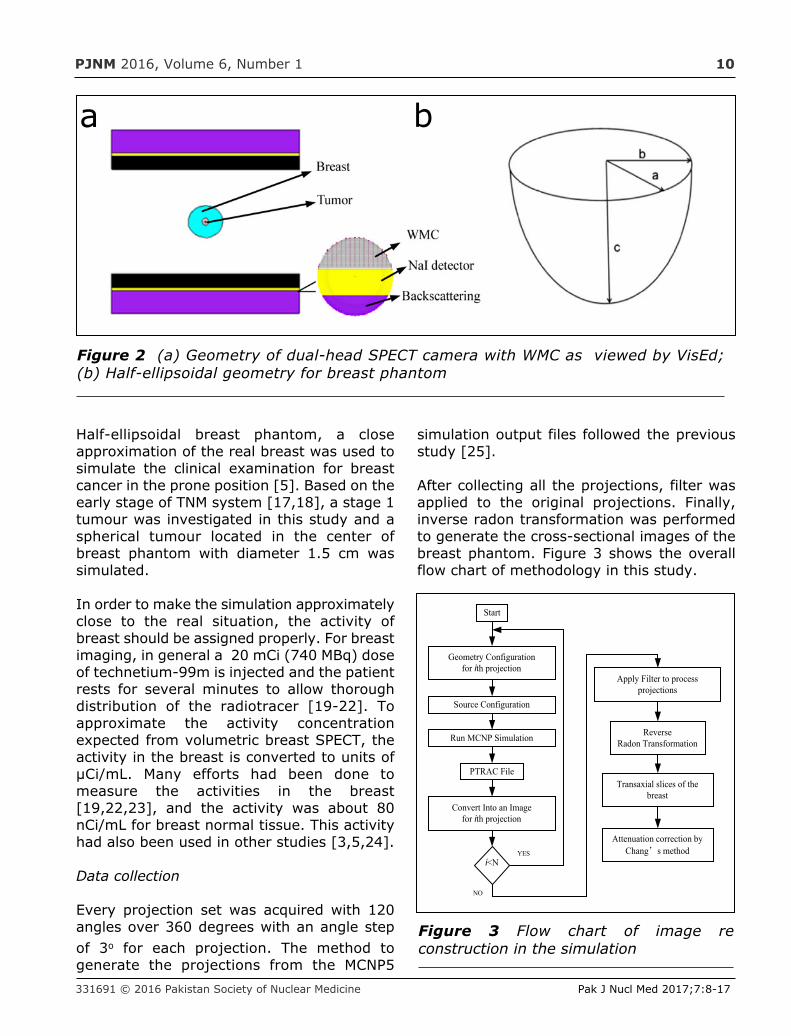
Half-ellipsoidal breast phantom, a closeapproximation of the real breast was used tosimulate the clinical examination for breastcancer in the prone position [5]. Based on theearly stage of TNM system [17,18], a stage 1tumour was investigated in this study and aspherical tumour located in the center ofbreast phantom with diameter 1.5 cm wassimulated.
In order to make the simulation approximatelyclose to the real situation, the activity ofbreast should be assigned properly. For breastimaging, in general a 20 mCi (740 MBq) doseof technetium-99m is injected and the patientrests for several minutes to allow thoroughdistribution of the radiotracer [19-22]. Toapproximate the activity concentrationexpected from volumetric breast SPECT, theactivity in the breast is converted to units ofµCi/mL. Many efforts had been done tomeasure the activities in the breast[19,22,23], and the activity was about 80nCi/mL for breast normal tissue. This activityhad also been used in other studies [3,5,24].
Data collection
Every projection set was acquired with 120angles over 360 degrees with an angle stepof 3o for each projection. The method togenerate the projections from the MCNP5
simulation output files followed the previousstudy [25].
After collecting all the projections, filter wasapplied to the original projections. Finally,inverse radon transformation was performedto generate the cross-sectional images of thebreast phantom. Figure 3 shows the overallflow chart of methodology in this study.
331691 © 2016 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
a b
Figure 2 (a) Geometry of dual-head SPECT camera with WMC as viewed by VisEd;(b) Half-ellipsoidal geometry for breast phantom
Start
YES
Transaxial slices of thebreast
ReverseRadon Transformation
Apply Filter to processprojections
Convert Into an Imagefor ith projection
PTRAC File
Run MCNP Simulation
Source Configuration
Geometry Configurationfor ith projection
i<N
NO
Attenuation correction byChang’s method
Figure 3 Flow chart of image reconstruction in the simulation
PJNM 2016, Volume 6, Number 1 11
The transaxial slices were obtained by imagereconstruction using filtered back projectionwith matrix of 64x64, which yields a voxel sizeof 0.39x0.39x0.39 cm3. Images werecorrected by attenuation correction based onChang's method [26] with a linear attenuationcoefficient of 0.12-1 cm [2,11,27]. No scattercorrection was applied in this study.
Filter Evaluation
Six different filters were compared with 17different Fc, ranging from 0.2 Nq to 1.0 Nq,with step 0.05. For Butterworth filter, orderwas from 3 to 12 with step 1. A total of 255central slices with different filter parameterswere reconstructed to compare theperformance in terms of contrast, noise leveland tumour size.
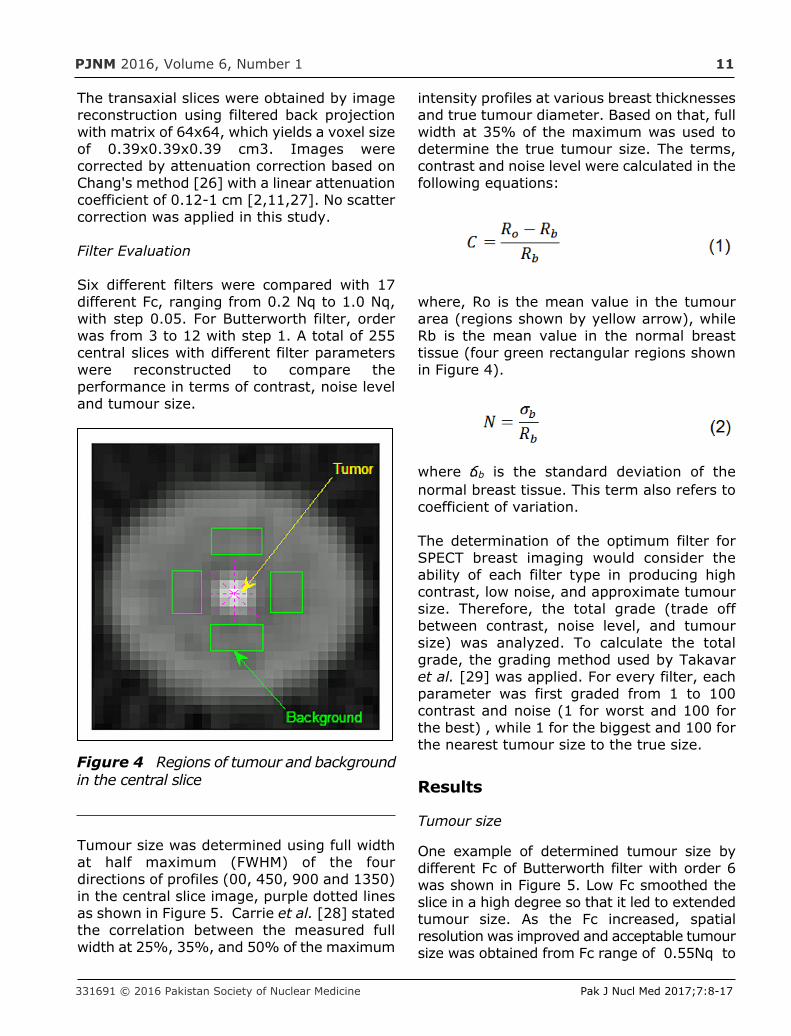
Tumour size was determined using full widthat half maximum (FWHM) of the fourdirections of profiles (00, 450, 900 and 1350)in the central slice image, purple dotted linesas shown in Figure 5. Carrie et al. [28] statedthe correlation between the measured fullwidth at 25%, 35%, and 50% of the maximum
intensity profiles at various breast thicknessesand true tumour diameter. Based on that, fullwidth at 35% of the maximum was used todetermine the true tumour size. The terms,contrast and noise level were calculated in thefollowing equations:
where, Ro is the mean value in the tumourarea (regions shown by yellow arrow), whileRb is the mean value in the normal breasttissue (four green rectangular regions shownin Figure 4).
where ճb is the standard deviation of thenormal breast tissue. This term also refers tocoefficient of variation.
The determination of the optimum filter forSPECT breast imaging would consider theability of each filter type in producing highcontrast, low noise, and approximate tumoursize. Therefore, the total grade (trade offbetween contrast, noise level, and tumoursize) was analyzed. To calculate the totalgrade, the grading method used by Takavaret al. [29] was applied. For every filter, eachparameter was first graded from 1 to 100contrast and noise (1 for worst and 100 forthe best) , while 1 for the biggest and 100 forthe nearest tumour size to the true size.
Results
Tumour size
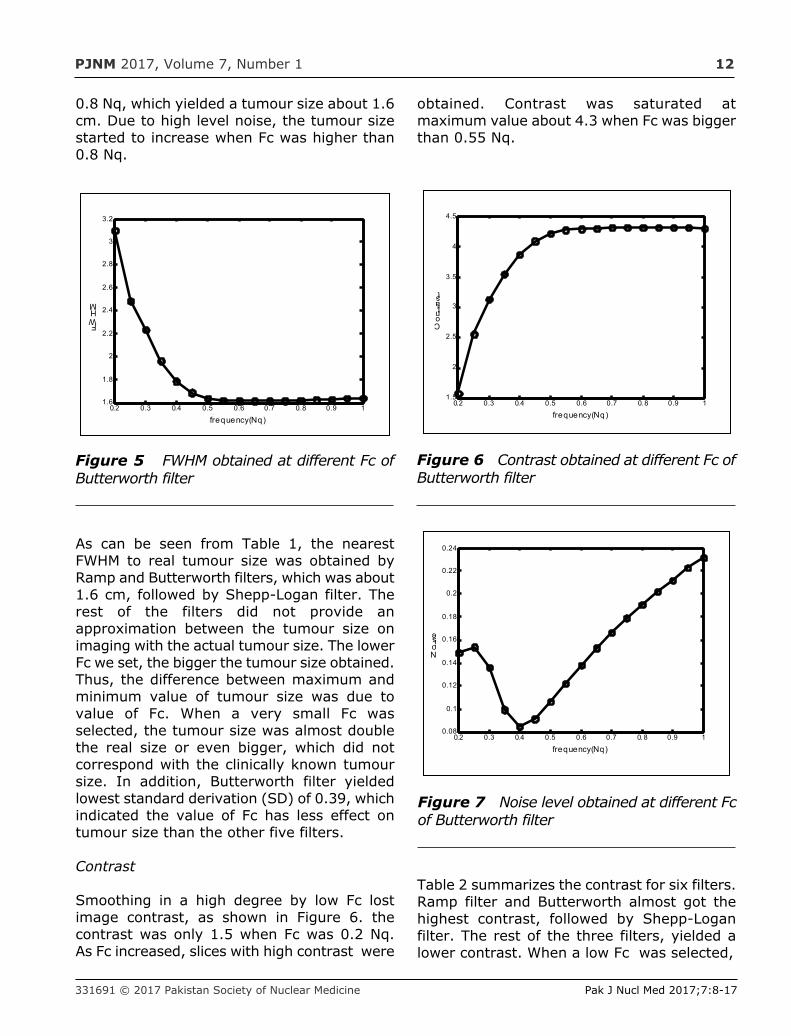
One example of determined tumour size bydifferent Fc of Butterworth filter with order 6was shown in Figure 5. Low Fc smoothed theslice in a high degree so that it led to extendedtumour size. As the Fc increased, spatialresolution was improved and acceptable tumoursize was obtained from Fc range of 0.55Nq to
331691 © 2016 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
Figure 4 Regions of tumour and backgroundin the central slice
PJNM 2017, Volume 7, Number 1 12
0.8 Nq, which yielded a tumour size about 1.6cm. Due to high level noise, the tumour sizestarted to increase when Fc was higher than0.8 Nq.
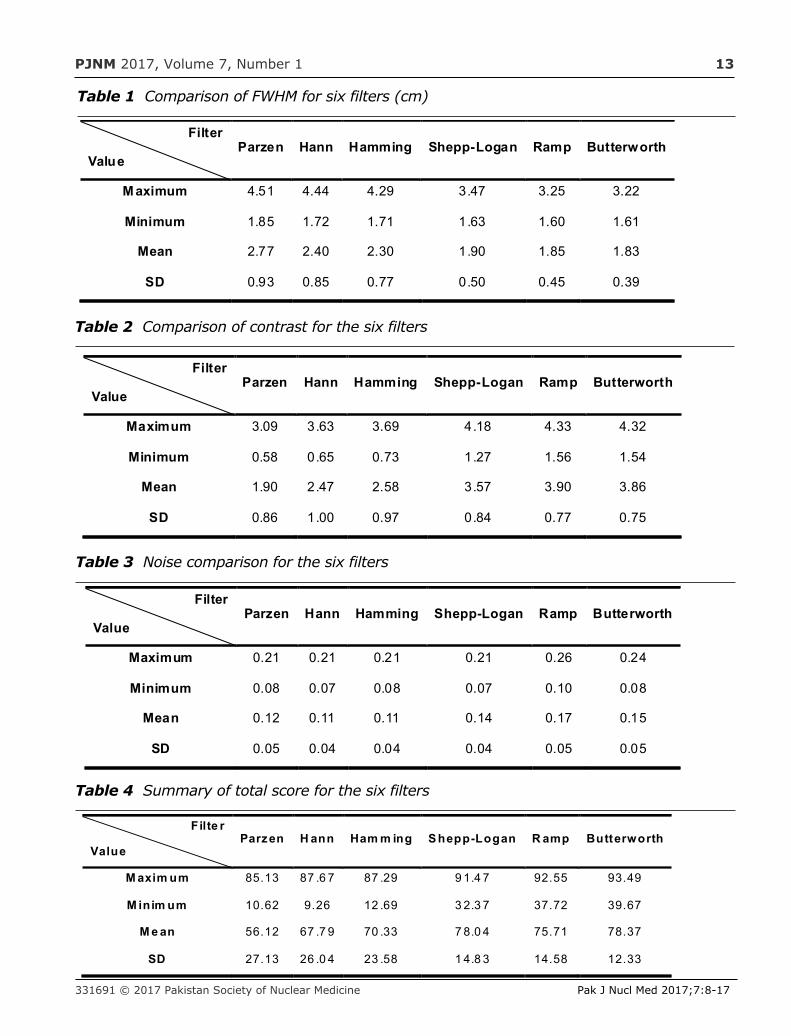
As can be seen from Table 1, the nearestFWHM to real tumour size was obtained byRamp and Butterworth filters, which was about1.6 cm, followed by Shepp-Logan filter. Therest of the filters did not provide anapproximation between the tumour size onimaging with the actual tumour size. The lowerFc we set, the bigger the tumour size obtained.Thus, the difference between maximum andminimum value of tumour size was due tovalue of Fc. When a very small Fc wasselected, the tumour size was almost doublethe real size or even bigger, which did notcorrespond with the clinically known tumoursize. In addition, Butterworth filter yieldedlowest standard derivation (SD) of 0.39, whichindicated the value of Fc has less effect ontumour size than the other five filters.
Contrast
Smoothing in a high degree by low Fc lostimage contrast, as shown in Figure 6. thecontrast was only 1.5 when Fc was 0.2 Nq.As Fc increased, slices with high contrast were
obtained. Contrast was saturated atmaximum value about 4.3 when Fc was biggerthan 0.55 Nq.
Table 2 summarizes the contrast for six filters.Ramp filter and Butterworth almost got thehighest contrast, followed by Shepp-Loganfilter. The rest of the three filters, yielded alower contrast. When a low Fc was selected,
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
0.2 0.3 0.4 0.5 0.6 0.7 0. 8 0.9 11.6
1.8
2
2.2
2.4
2.6
2.8
3
3.2
frequency(Nq)
Figure 5 FWHM obtained at different Fc ofButterworth filter
Figure 6 Contrast obtained at different Fc ofButterworth filter
0.2 0.3 0.4 0.5 0.6 0.7 0. 8 0.9 11.5
2
2.5
3
3.5
4
4.5
frequency(Nq)
0.2 0.3 0.4 0.5 0.6 0.7 0. 8 0.9 10.08
0.1
0.12
0.14
0.16
0.18
0.2
0.22
0.24
frequency(Nq)
Figure 7 Noise level obtained at different Fcof Butterworth filter
PJNM 2017, Volume 7, Number 1 13
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
Filter
ValueParzen Hann Hamming Shepp-Logan Ramp Butterworth
M aximum 4.51 4.44 4.29 3.47 3.25 3.22
Minimum 1.85 1.72 1.71 1.63 1.60 1.61
Mean 2.77 2.40 2.30 1.90 1.85 1.83
SD 0.93 0.85 0.77 0.50 0.45 0.39
Table 1 Comparison of FWHM for six filters (cm)
Table 2 Comparison of contrast for the six filters
Filter
ValueParzen Hann Hamming Shepp-Logan Ramp Butterworth
Maximum 3.09 3.63 3.69 4.18 4.33 4.32
Minimum 0.58 0.65 0.73 1.27 1.56 1.54
Mean 1.90 2.47 2.58 3.57 3.90 3.86
SD 0.86 1.00 0.97 0.84 0.77 0.75
Table 3 Noise comparison for the six filters
Filter
ValueParzen Hann Hamming Shepp-Logan Ramp Butterworth
Maximum 0.21 0.21 0.21 0.21 0.26 0.24
Minimum 0.08 0.07 0.08 0.07 0.10 0.08
Mean 0.12 0.11 0.11 0.14 0.17 0.15
SD 0.05 0.04 0.04 0.04 0.05 0.05
Table 4 Summary of total score for the six filters
Filte r
ValueParzen H ann Ham m ing S hepp-Logan R amp Butterworth
M axim um 85.13 87 .6 7 87 .29 9 1.4 7 92.55 93.49
M inim um 10.62 9.26 12 .69 3 2.3 7 37.72 39.67
M e an 56.12 67 .7 9 70 .33 7 8.0 4 75.71 78.37
SD 27.13 26 .0 4 23 .58 1 4.8 3 14.58 12.33
PJNM 2017, Volume 7, Number 1 14
slice image was dramatically smoothed. As wecan see, the minimum value of contrast forParzen, Hann and Hamming filters was about0.6, which was substantially decreased thetumour visibility. Again, Butterworth obtainedthe lowest value of SD.
Noise
Low Fc generally eliminated noise effectivelyand led to a smoothing of the image. However,as we can see from Figure 7, the minimumnoise level was obtained at Fc 0.4 Nq otherthan 0.2 Nq since we calculated the SD ofbackground to be the noise level. With higherFc, it generated slices with a high level noise.
The noise level for six filters was shown inTable 3. Apparently Parzen, Hann andHamming filters got smoother images. Thisis reasonable because they are designed toreduce noise effectively. While Shepp-Loganand Butterworth filters, especially the Ramp
filter, amplified the high frequencies, whichled to a little noisier image.
Total score
Table 4 summarizes the total score for the sixfilters. Butterworth filter got the highest meanscore among all the six filters, because itobtained high contrast and approximatetumour size, and a little low level of noise. Atthe same time, Butterworth filter obtained thehighest maximum value of 93.49 and smallestSD of 12.33. in other words, Butterworth filterenabled to balance the needs of high contrast,low noise, and accurate tumour size.
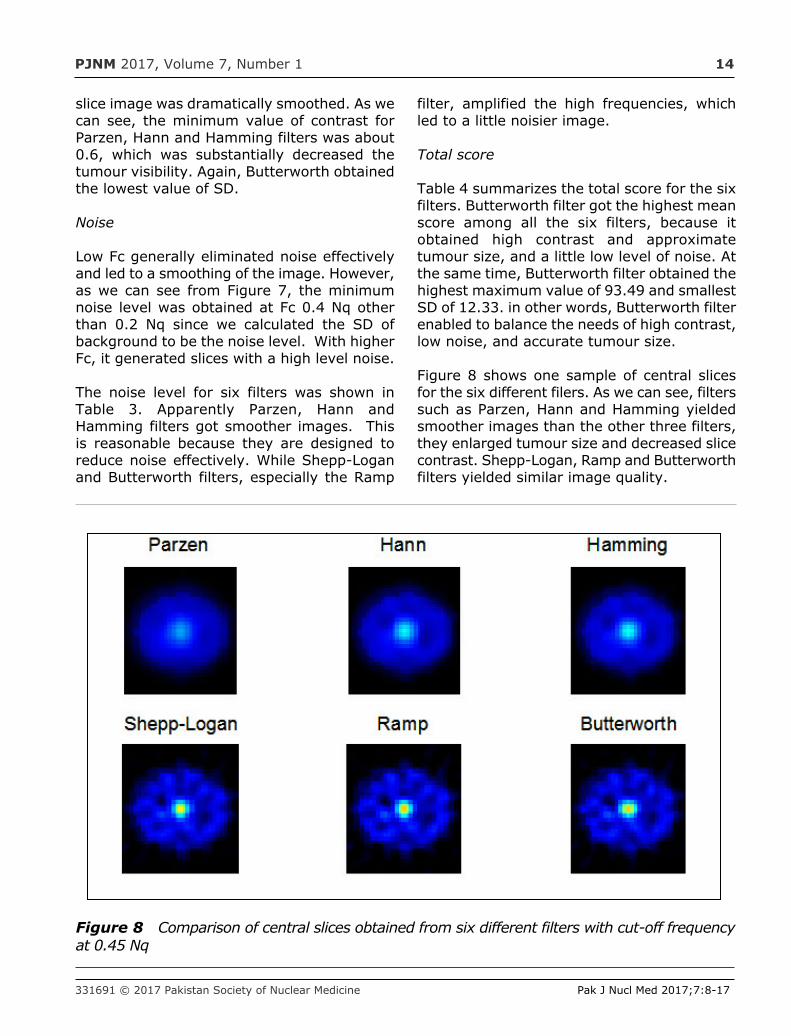
Figure 8 shows one sample of central slicesfor the six different filers. As we can see, filterssuch as Parzen, Hann and Hamming yieldedsmoother images than the other three filters,they enlarged tumour size and decreased slicecontrast. Shepp-Logan, Ramp and Butterworthfilters yielded similar image quality.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
Figure 8 Comparison of central slices obtained from six different filters with cut-off frequencyat 0.45 Nq
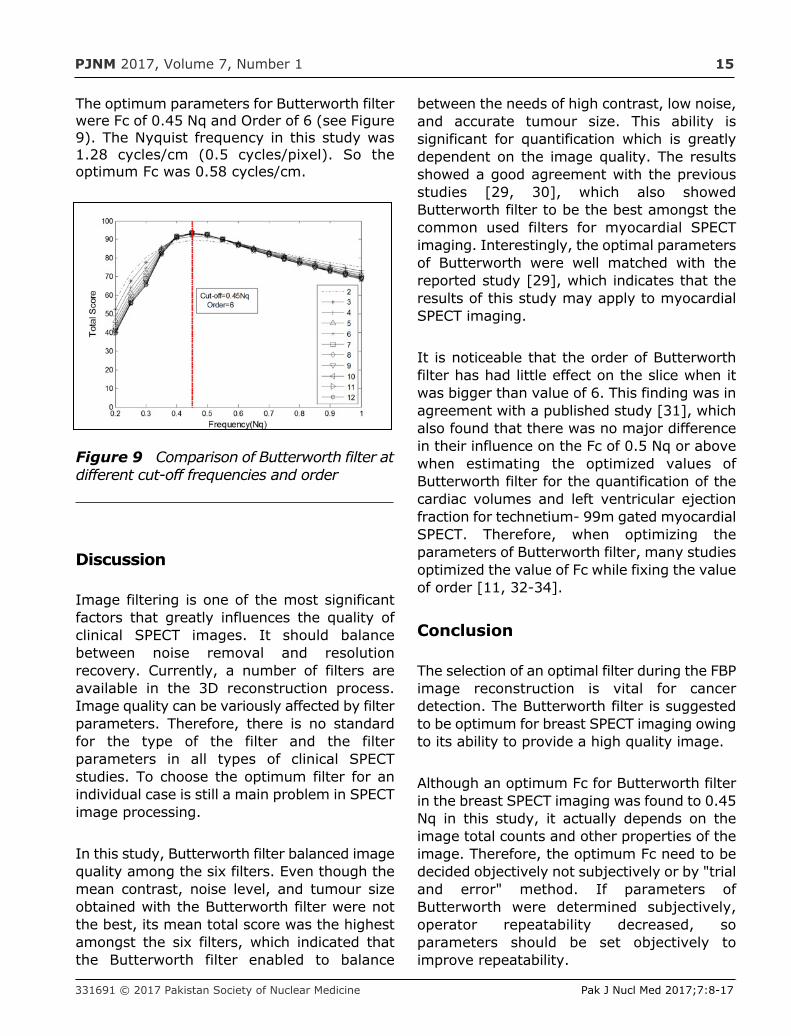
PJNM 2017, Volume 7, Number 1 15
The optimum parameters for Butterworth filterwere Fc of 0.45 Nq and Order of 6 (see Figure9). The Nyquist frequency in this study was1.28 cycles/cm (0.5 cycles/pixel). So theoptimum Fc was 0.58 cycles/cm.
Discussion
Image filtering is one of the most significantfactors that greatly influences the quality ofclinical SPECT images. It should balancebetween noise removal and resolutionrecovery. Currently, a number of filters areavailable in the 3D reconstruction process.Image quality can be variously affected by filterparameters. Therefore, there is no standardfor the type of the filter and the filterparameters in all types of clinical SPECTstudies. To choose the optimum filter for anindividual case is still a main problem in SPECTimage processing.
In this study, Butterworth filter balanced imagequality among the six filters. Even though themean contrast, noise level, and tumour sizeobtained with the Butterworth filter were notthe best, its mean total score was the highestamongst the six filters, which indicated thatthe Butterworth filter enabled to balance
between the needs of high contrast, low noise,and accurate tumour size. This ability issignificant for quantification which is greatlydependent on the image quality. The resultsshowed a good agreement with the previousstudies [29, 30], which also showedButterworth filter to be the best amongst thecommon used filters for myocardial SPECTimaging. Interestingly, the optimal parametersof Butterworth were well matched with thereported study [29], which indicates that theresults of this study may apply to myocardialSPECT imaging.
It is noticeable that the order of Butterworthfilter has had little effect on the slice when itwas bigger than value of 6. This finding was inagreement with a published study [31], whichalso found that there was no major differencein their influence on the Fc of 0.5 Nq or abovewhen estimating the optimized values ofButterworth filter for the quantification of thecardiac volumes and left ventricular ejectionfraction for technetium- 99m gated myocardialSPECT. Therefore, when optimizing theparameters of Butterworth filter, many studiesoptimized the value of Fc while fixing the valueof order [11, 32-34].
Conclusion
The selection of an optimal filter during the FBPimage reconstruction is vital for cancerdetection. The Butterworth filter is suggestedto be optimum for breast SPECT imaging owingto its ability to provide a high quality image.
Although an optimum Fc for Butterworth filterin the breast SPECT imaging was found to 0.45Nq in this study, it actually depends on theimage total counts and other properties of theimage. Therefore, the optimum Fc need to bedecided objectively not subjectively or by "trialand error" method. If parameters ofButterworth were determined subjectively,operator repeatability decreased, soparameters should be set objectively toimprove repeatability.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
Figure 9 Comparison of Butterworth filter atdifferent cut-off frequencies and order
PJNM 2017, Volume 7, Number 1 16
Acknowledgement
The project is funded by the Ministry ofScience, Technology and Innovation (UPM)under Science fund Grant number 5450786(06-01-04-SF2157).
References
1. M. Lyra, A. Ploussi, Filtering in SPECT imagereconstruction, Int. J. Biomed. Imaging. 2011(2011) 1-14.
2. M. Lyra, A. Ploussi, M. Rouchota, S. Synefia,Filters in 2D and 3D Cardiac SPECT ImageProcessing, Cardiol. Res. Pract. 2014 (2014)1-11.
3. W.H.M. Saad, R.E. Roslan, M.A. Mahdi, W.S.Choong, E. Saion, M.I. Saripan, Monte Carlodesign of optimal wire mesh collimator forbreast tumor imaging process, Nucl.Instruments Methods Phys. Res. Sect. A Accel.Spectrometers, Detect. Assoc. Equip. 648(2011) 254-260.
4. M. Saripan, W. Saad, Monte Carlo Simulationon Breast Cancer Detection Using Wire MeshCollimator Gamma Camera, IEEE Trans. Nucl.Sci. 56 (2009) 1321-1324.
5. R.E. Roslan, W.H.M. Saad, M.I. Saripan, S.Hashim, W.-S. Choong, The performance ofa wire mesh collimator SPECT camera fordifferent breast volumes in prone position,Nucl. Instruments Methods Phys. Res. Sect.A Accel. Spectrometers, Detect. Assoc. Equip.619 (2010) 385-387.
6. M.I. Saripan, M. Petrou, K. Wells, Design of awire-mesh collimator for gamma cameras.,IEEE Trans. Biomed. Eng. 54 (2007) 1598-612.
7. Y. Wang, B.M.W. Tsui, S. Member, W.H. Baird,E.C. Frey, D.E. Wessell, Investigation ofAcquisition and Image ReconstructionParameters for Rotating Multi-Segment Slant-Hole SPECT, in: Nucl. Sci. Symp. Conf. Rec.,2001: pp. 2143-2146.
8. W.H. Baird, E.C. Frey, B.M.W. Tsui, Y. Wang,D.E. Wessell, Evaluation of rotating slant-hole
SPECT mammography using Monte CarloSimulation methods, IEEE Trans. Nucl. Sci. 50I (2003) 105-109.
9. S.D. Metzler, J.E. Bowsher, M.P. Tornai, B.C.Pieper, S. Member, J. Peter, R.J. Jaszczak,SPECT Breast Imaging Combining Horizontaland Vertical Axes of Rotation, IEEE Trans.Nucl. Sci. 49 (2002) 31-36.
10. K.L. Perez, S.J. Cutler, Towards Quantificationof Functional Breast Images Using DedicatedSPECT With Non-Traditional AcquisitionTrajectories, IEEE Trans. Nucl. Sci. 58 (2011)2219-2225.
11. H. Onishi, Y. Matsutake, N. Matsutomo, H.Amijima, Validation of optimal cut-offfrequency using a Butterworth filter in singlephoton emission computed tomographyreconstruction for the target organ?: Spatialdomain and frequency domain, J. Fac. Heal.Welf. 10 (2010) 27-36.
12. SIEMENS, SIEMENS SPECT Symbia S and T:system specifications, Germany, 2010.
13. X-5 Monte Carlo Team, MCNP - A GeneralMonte Carlo N-Particle Transport Code,Version 5, 2005.
14. M.T. Bahreyni Toossi, J.P. Islamian, M.Momennezhad, M. Ljungberg, S.H. Naseri,SIMIND Monte Carlo simulation of a singlephoton emission CT, J. Med. Phys. 35 (2010)42-47.
15. Gopal B. Saha, Physics and Radiobiology ofNuclear Medicine, Fourth edi, Springer, NewYork, 2013.
16. D.J. de Vries, S.C. Moore, R.E. Zimmerman,B. Friedland, S.P. Mueller, R.C. Lanza,Development and Validation of a Monte CarloSimulation of Photon Transport in an AngerCamera, IEEE Trans. Med. Imaging. 9 (1990)430-438.
17. Cancer Research, Number Stages of BreastCancer, (n.d.).http://www.cancerresearchuk.org/about-c a n c e r / t y p e / b r e a s t -cancer/treatment/number-stages-of-breast-cancer (accessed September 30, 2014).
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:8-17
PJNM 2017, Volume 7, Number 1 17
18. L.H.Sobin, M.K.Gospodarowicz, Ch.Wittekind,TNM?: classification of malignant tumours,seventh, Willey-Blackwell press, UK, 2009.
19. K.L. Perez, Investigating Functional BreastImage Quality and Quantification with adedicated SPECT-CT System, Duke University,2011.
20. M.K. O'Connor, S.W. Phillips, C.B. Hruska, D.J.Rhodes, D.A. Collins, Molecular breast imaging:advances and limitations of ascintimammographic technique in patients withsmall breast tumors, Clin. Imaging. 31 (2007)295.
21. F.J. Wackers, D.S. Berman, J. Maddahi, D.D.Watson, G.A. Beller, H.W. Strauss, C.A. Boucher,M. Picard, B.L. Holman, R. Fridrich, Technetium-99m hexakis 2-methoxyisobutyl isonitrile:human biodistribution, dosimetry, safety, andpreliminary comparison to thallium-201 formyocardial perfusion imaging., J. Nucl. Med. 30(1989) 301-311.
22. J. Maublant, M. de Latour, D. Mestas, aClemenson, S. Charrier, V. Feillel, G. LeBouedec, P. Kaufmann, J. Dauplat, a Veyre,Technetium-99m-sestamibi uptake in breasttumor and associated lymph nodes., J. Nucl.Med. 37 (1996) 922-925.
23. S.D. Mann, K.L. Perez, E.K.E. McCracken, J.P.Shah, T.Z. Wong, M.P. Tornai, Initial in vivoquantification of Tc-99m Sestamibi uptake as afunction of tissue type in healthy breasts usingdedicated breast SPECT-CT, J. Oncol. 2012(2012) 1-7.
24. G.J. Gruber, W.W. Moses, S.E. Derenzo, MonteCarlo simulation of breast tumor imagingproperties with compact, discrete gammacameras, IEEE Trans. Nucl. Sci. 46 (1999).
25. X. Dong, W.H.M. Saad, W.A.W. Adnan, S.Hashim, N.P. za M. Hassan, A.J. Nordin, M.I.Saripan, Simulation of intrinsic resolution ofscintillation camera in Monte Carlo environment,in: IEEE ICSIPA 2013 - IEEE Int. Conf. SignalImage Process. Appl., 2013: pp. 11-14.
26. L. Chang, A Method for Attenuation Correctionin Radionuclide Computed Tomography, IEEETrans. Nucl. Sci. 25 (1978) 638-643.
27. IAEA, IAEA Quality Control Atlas for ScintillationCamera Systems, 2003.
28. C.B. Hruska, M.K.O. Connor, Quantification oflesion size , depth , and uptake using a dual-head molecular breast imaging system, Med.Phys. 35 (2008) 1365-1377.
29. A. Takavar, G. Shamsipour, M. Sohrabi, M.Eftekhari, Determination of optimum filter inmyocardial SPECT: A phantom study, Iran. J.Radiat. Res. 1 (2004) 205-210.
30. M.N.S. Yusoff, A. Zakaria, Determination of theoptimum filter for qualitative and quantitative99m Tc myocardial SPECT imaging, Iran. J.Radiat. Res. 6 (2009) 173-182.
31. D.D. Duarte, M.S. Monteiro, F.E. Hakmaoui, J.O.Prior, L. Vieira, J. a. Pires-Jorge, Influence ofReconstruction Parameters During FilteredBackprojection and Ordered-Subset ExpectationMaximization in the Measurement of the Left-Ventricular Volumes and Function During GatedSPECT, J. Nucl. Med. Technol. 40 (2012) 29-36.
32. S. Minoshima, H. Maruno, N. Yui, T. Togawa, F.Kinoshita, M. Kubota, K.L. Berger, Y. Uchida, K.Uno, N. Arimizu, Optimization of Butterworthfilter for brain SPECT imaging, Ann. Nucl. Med.7 (1993) 71-77.
33. S. Sankaran, E.C. Frey, K.L. Gilland, B.M.W.Tsui, Optimum compensation method and filtercutoff frequency in myocardial SPECT: a humanobserver study, J. Nucl. Med. 43 (2002) 432-438.
34. T. Shibutani, M. Onoguchi, T. Yamada, H.Kamida, K. Kunishita, Y. Hayashi, T. Nakajima,S. Kinuya, Optimization of the filter parametersin 99mTc myocardial perfusion SPECT studies:the formulation of flowchart, Australas. Phys.Eng. Sci. Med. 39 (2016) 571-581.
Pak J Nucl Med 2017;7:8-17 2305-1630(201701/01)7:1<8:DOFTSB>2.0.TX;2-M
PJNM 2017; 7:18-23 331691 © 2017 Pakistan Society of Nuclear Medicine
Measurement of radiation doses to occupationalworkers in nuclear medicine
Misbah Javed1, Saeed Ur Rahman2, Iqra Tanveer1,Ghulam Asghar1, Shazia Fatima2, Mohammad Fahim2
1Department of Physics, University of Poonch, Rawalakot, Azad Kashmir2Department of Medical Physics, Nuclear Medicine, Oncology and
Radiotherapy Institute (NORI), Islamabad
ORIGINAL ARTICLE
Abstract
Aims The study aimed at measuring theexternal radiation doses to workers frompatients who were administeredradiopharmaceuticals in the nuclear medicinedepartment. The purpose of this study was toevaluate the radiation safety procedures in thedepartment of nuclear medicine.
Methods A total of 80 patients were randomlyselected for the study. These patients wereinjected with either 99mTc-pertechnetate or99mTc-MDP (methylene diphosphonate). Thedose rate was measured in hot lab, waitingroom and in the scanning room at distances of10, 50 and 100 cm from the patient at differenttime intervals by using a radiation surveymeter. The absorbed dose from radioactivepatient to radiation workers was calculated byusing RADAR software and mathematicalformulae from the measured dose rate.
Results The mean dose rate from thyroid scanpatients at a distance of 10, 50 and 100 cm,after administration of injection was found tobe 41 µSv/h, 31 µSv/h and 22 µSv/hrespectively; whereas the dose rate from bonescan patients was calculated at 62 µSv/h, 31µSv/h and 28 µSv/h. The dose rate was alsomeasured after 15 min and 30 min in waitingand scanning room for the same patients. Themean absorbed dose to nuclear medicineoccupational workers calculated both manuallyand using RADAR software came out to be lessthan 1mSv/year.
Conclusion The external doses to radiationworkers were within permissible level. Theresults obtained in the present study arecomparable to the previous studies conductedworld wide. The radiation dose level tooccupational workers in our nuclear medicinedepartment does not exceed the recommendeddose limits for workers.
Key words: Radiation safety, External doserate, absorbed dose from radioactive patient
Introduction
Radionuclides are used in nuclear medicine forvarious kinds of diagnostic and treatment
*Correspondence
Mishbah Javed Department of Physics, University of Poonch, Rawalakot, Azad Kashmir Email: [email protected] Tel: +923323132040
www.pjnm.net 2305-1630(201701/01)7:1<18:MRDOWN>2.0.TX;2-M
PJNM 2017, Volume 7, Number 1 19
Radiopharmaceuticals injected to patients in aspecific amount for a particular test. The mostcommonly used radionuclide in our departmentare 99mTc and 131I. It is obvious from earlierstudies that external ionizing radiation exposureof nuclear medicine workers arises mostly fromradioactive patients rather than thepreparation and injection of radiopharmaceuticals [1]. Many researchers havemeasured the dose rates at different distancesand time intervals from the injected patients tohighlight the exposure to radiation workers [2,3].
Radiation exposure in nuclear medicine iscaused by radioactive sources and patients.Radioactive patients are a source of radiationfor workers and attendants of the patient [4].It is therefore necessary to quantify theradiation exposure from the patients tooccupational workers in the nuclear medicinedepartment. The aim of this study was tomeasure external radiation doses to workersdue to patients who have been administeredradiopharmaceuticals in the nuclear medicinedepartment.
Materials and Methods
In this study, dose rate was measured frominjected patients to quantify the doses tooccupational workers in the nuclear medicinedepartment. For this purpose, 80 patients (45males, 35 females) were randomly selected. Theages of the patients ranged from 20-60 years(mean age 37.5 years).
The selected patients were divided into twogroups: 1) patients who were injected with99mTc-pertechnetate (thyroid scan patients) and2) bone scan patients who were administered99mTc-methylene disphosphonate (99mTc-MDP).The activity injected to each patient wasmeasured using a radioisotope dose calibrator(Capintec CRC®-55tR) installed the hot lab of thenuclear medicine department.
The dose rate was measured by using surveymeter at preselected distances and locations. TheLAMSE RM1001-RD survey meter was used inthe present study. It measures the radiations in
energy range of 50keV to 1.3MeV, and dose ratesin the range 0.1µSv/h to 2mSv/h.
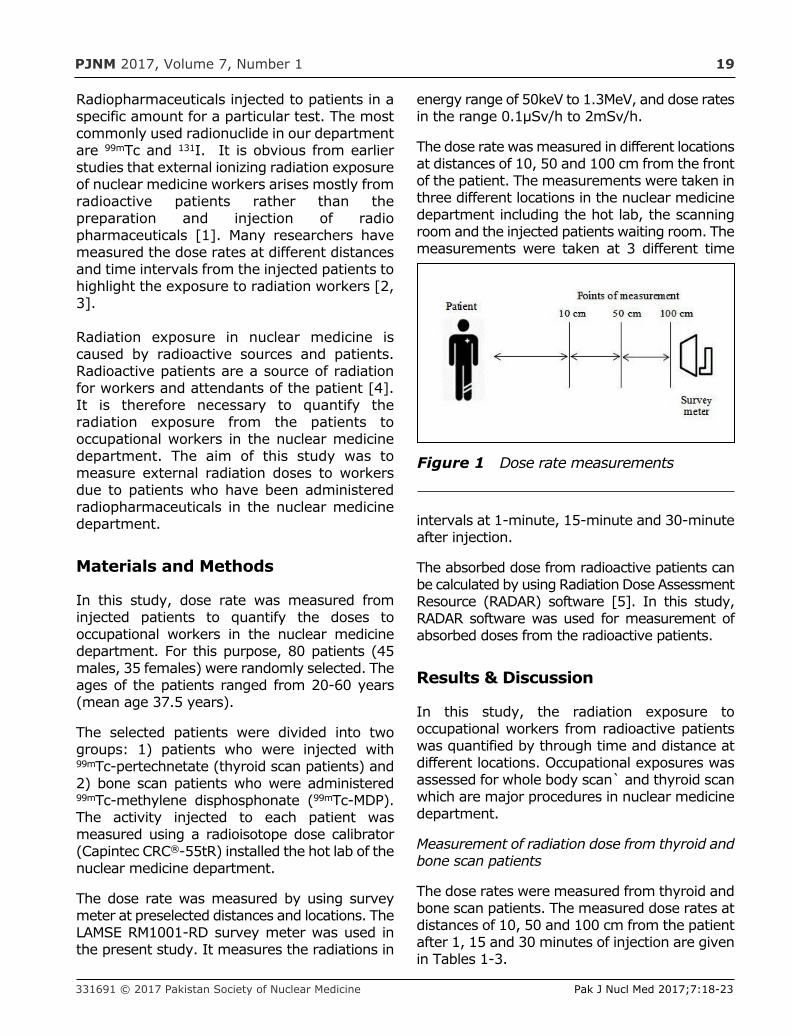
The dose rate was measured in different locationsat distances of 10, 50 and 100 cm from the frontof the patient. The measurements were taken inthree different locations in the nuclear medicinedepartment including the hot lab, the scanningroom and the injected patients waiting room. Themeasurements were taken at 3 different time
intervals at 1-minute, 15-minute and 30-minuteafter injection.
The absorbed dose from radioactive patients canbe calculated by using Radiation Dose AssessmentResource (RADAR) software [5]. In this study,RADAR software was used for measurement ofabsorbed doses from the radioactive patients.
Results & Discussion
In this study, the radiation exposure tooccupational workers from radioactive patientswas quantified by through time and distance atdifferent locations. Occupational exposures wasassessed for whole body scan` and thyroid scanwhich are major procedures in nuclear medicinedepartment.
Measurement of radiation dose from thyroid andbone scan patients
The dose rates were measured from thyroid andbone scan patients. The measured dose rates atdistances of 10, 50 and 100 cm from the patientafter 1, 15 and 30 minutes of injection are givenin Tables 1-3.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:18-23
Figure 1 Dose rate measurements

PJNM 2017, Volume 7, Number 1 20
The measured values in Table 1-3 show thatthe dose rates for bone scan patients are higherthan dose rates from the thyroid scan patientsbecause the average injected activity of 15.76mCi is higher as compared to that given forthyroid scans at 4.85 mCi. The measured valuesalso showed that the dose rates to staff fromradioactive patients depends on distance. As per
the inverse square law, by increasing thedistance from the injected patient, the dose ratedecreases inversely with the square of thedistance: doubling the distance betweenradioactive patient and the radiation source willreduce radiation exposure by a factor of 4.Unnecessary staff exposure is avoided bymaintain a safe distance from the patient.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:18-23
Table 1 Mean dose rate after 1 minute of administrated activity of 99mTc-pertechnetate and99mTc-MDP in the Hot Lab
Distance (cm)Thyroid scan Bone scan
Mean dose rate (μSv/h) ± SD Mean dose rate(μSv/h) ±SD
10 41.5±10.9 62.7±15.9
50 31.7±10.4 44.8±14.1
100 22.7±8.9 28.8±11.7
Table 2 Mean dose rate after 15 minutes of administrated activity of 99mTc-pertechnetate and99mTc-MDP in the waiting room
Distance(cm)
Thyroid scan Bone scan
Mean dose rate(μSv/h)±SD
Mean dose rate(μSv/h)±SD
10 28.69±9.1 41.9±13.1
50 19.36±8.1 26.7±11.2
100 11.48±6.2 20.3±10.5
Table 3 Mean dose rate after 30 minutes of administrated activity of 99mTc-pertechnetate and99mTc-MDP in the scanning room
Distance(cm)
Thyroid scan Bone scan
Mean dose rate(μSv/h)±SD
Mean dose rate (μSv/h)±SD
10 18.29±8.0 23.7±10.8
50 9.6±4.9 14.5±8.8
100 6.27±3.8 8.24±6.2
PJNM 2017, Volume 7, Number 1 21
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:18-23
Absorbed dose to staff
The absorbed dose to nuclear medicine staffwas calculated by using RADAR software. Thedose received to the nuclear medicine staff afteradministration of 99mTc-pertechnetate and99mTc-MDP given in Tables 4-6.
The exposure is directly proportional to timespent near the radioactive patients andinversely proportional to the distance fromradioactive patients as shown in Figures 2 and3.
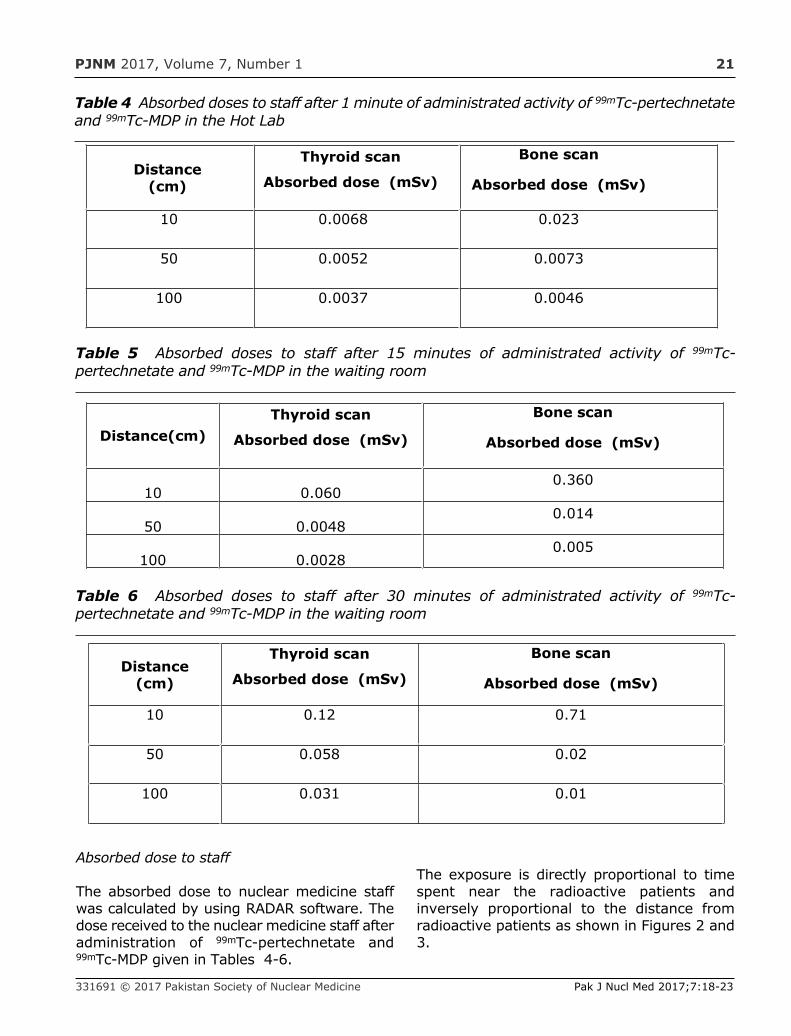
Table 4 Absorbed doses to staff after 1 minute of administrated activity of 99mTc-pertechnetateand 99mTc-MDP in the Hot Lab
Distance(cm)
Thyroid scan
Absorbed dose (mSv)
Bone scan
Absorbed dose (mSv)
10 0.0068 0.023
50 0.0052 0.0073
100 0.0037 0.0046
Table 5 Absorbed doses to staff after 15 minutes of administrated activity of 99mTc-pertechnetate and 99mTc-MDP in the waiting room
Distance(cm)Thyroid scan
Absorbed dose (mSv)
Bone scan
Absorbed dose (mSv)
10 0.0600.360
50 0.00480.014
100 0.00280.005
Table 6 Absorbed doses to staff after 30 minutes of administrated activity of 99mTc-pertechnetate and 99mTc-MDP in the waiting room
Distance(cm)
Thyroid scan
Absorbed dose (mSv)
Bone scan
Absorbed dose (mSv)
10 0.12 0.71
50 0.058 0.02
100 0.031 0.01
PJNM 2017, Volume 7, Number 1 22
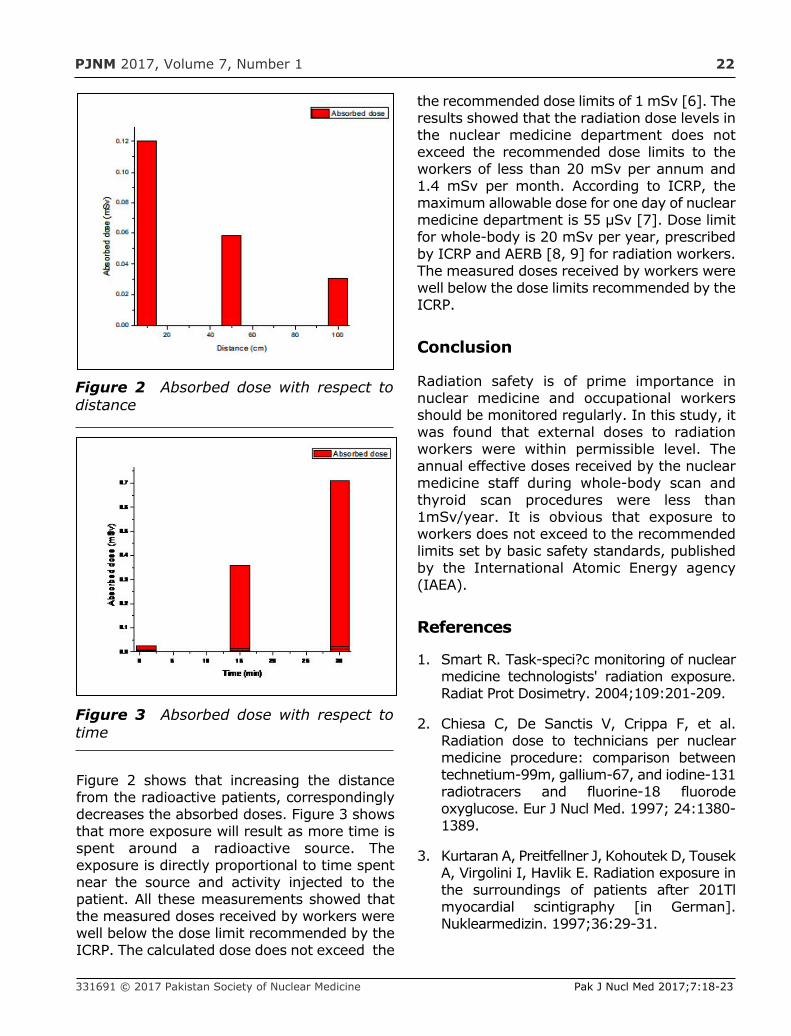
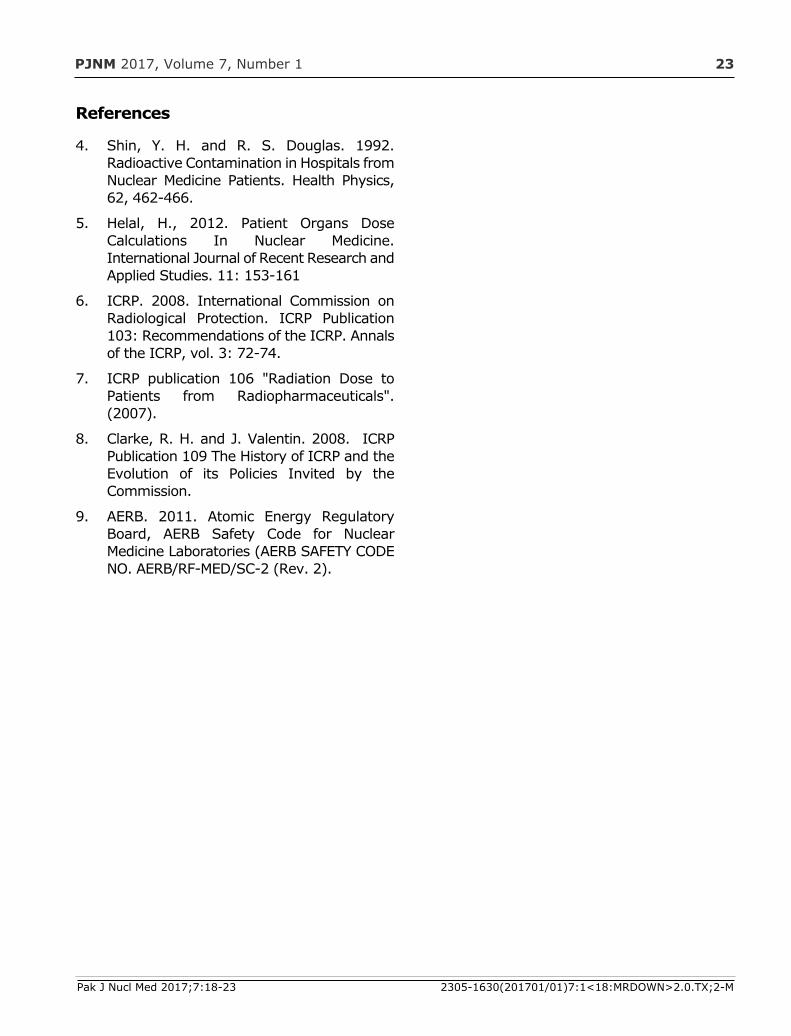
Figure 2 shows that increasing the distancefrom the radioactive patients, correspondinglydecreases the absorbed doses. Figure 3 showsthat more exposure will result as more time isspent around a radioactive source. Theexposure is directly proportional to time spentnear the source and activity injected to thepatient. All these measurements showed thatthe measured doses received by workers werewell below the dose limit recommended by theICRP. The calculated dose does not exceed the
the recommended dose limits of 1 mSv [6]. Theresults showed that the radiation dose levels inthe nuclear medicine department does notexceed the recommended dose limits to theworkers of less than 20 mSv per annum and1.4 mSv per month. According to ICRP, themaximum allowable dose for one day of nuclearmedicine department is 55 µSv [7]. Dose limitfor whole-body is 20 mSv per year, prescribedby ICRP and AERB [8, 9] for radiation workers.The measured doses received by workers werewell below the dose limits recommended by theICRP.
Conclusion
Radiation safety is of prime importance innuclear medicine and occupational workersshould be monitored regularly. In this study, itwas found that external doses to radiationworkers were within permissible level. Theannual effective doses received by the nuclearmedicine staff during whole-body scan andthyroid scan procedures were less than1mSv/year. It is obvious that exposure toworkers does not exceed to the recommendedlimits set by basic safety standards, publishedby the International Atomic Energy agency(IAEA).
References
1. Smart R. Task-speci?c monitoring of nuclearmedicine technologists' radiation exposure.Radiat Prot Dosimetry. 2004;109:201-209.
2. Chiesa C, De Sanctis V, Crippa F, et al.Radiation dose to technicians per nuclearmedicine procedure: comparison betweentechnetium-99m, gallium-67, and iodine-131radiotracers and fluorine-18 fluorodeoxyglucose. Eur J Nucl Med. 1997; 24:1380-1389.
3. Kurtaran A, Preitfellner J, Kohoutek D, TousekA, Virgolini I, Havlik E. Radiation exposure inthe surroundings of patients after 201Tlmyocardial scintigraphy [in German].Nuklearmedizin. 1997;36:29-31.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:18-23
Figure 2 Absorbed dose with respect todistance
Figure 3 Absorbed dose with respect totime
PJNM 2017, Volume 7, Number 1 23
References
4. Shin, Y. H. and R. S. Douglas. 1992.Radioactive Contamination in Hospitals fromNuclear Medicine Patients. Health Physics,62, 462-466.
5. Helal, H., 2012. Patient Organs DoseCalculations In Nuclear Medicine.International Journal of Recent Research andApplied Studies. 11: 153-161
6. ICRP. 2008. International Commission onRadiological Protection. ICRP Publication103: Recommendations of the ICRP. Annalsof the ICRP, vol. 3: 72-74.
7. ICRP publication 106 "Radiation Dose toPatients from Radiopharmaceuticals".(2007).
8. Clarke, R. H. and J. Valentin. 2008. ICRPPublication 109 The History of ICRP and theEvolution of its Policies Invited by theCommission.
9. AERB. 2011. Atomic Energy RegulatoryBoard, AERB Safety Code for NuclearMedicine Laboratories (AERB SAFETY CODENO. AERB/RF-MED/SC-2 (Rev. 2).
Pak J Nucl Med 2017;7:18-23 2305-1630(201701/01)7:1<18:MRDOWN>2.0.TX;2-M
PJNM 2017; 7:24-33 331691 © 2017 Pakistan Society of Nuclear Medicine
Behaviour of wedges for different field sizes anddepths
Sajjad Ahmed Memon*, Naeem Ahmed Laghari,Fayaz Hussain Mangi
Nuclear Institute of Medicine And Radiotherapy (NIMRA),Jamshoro, Pakistan
ORIGINAL ARTICLE
Abstract
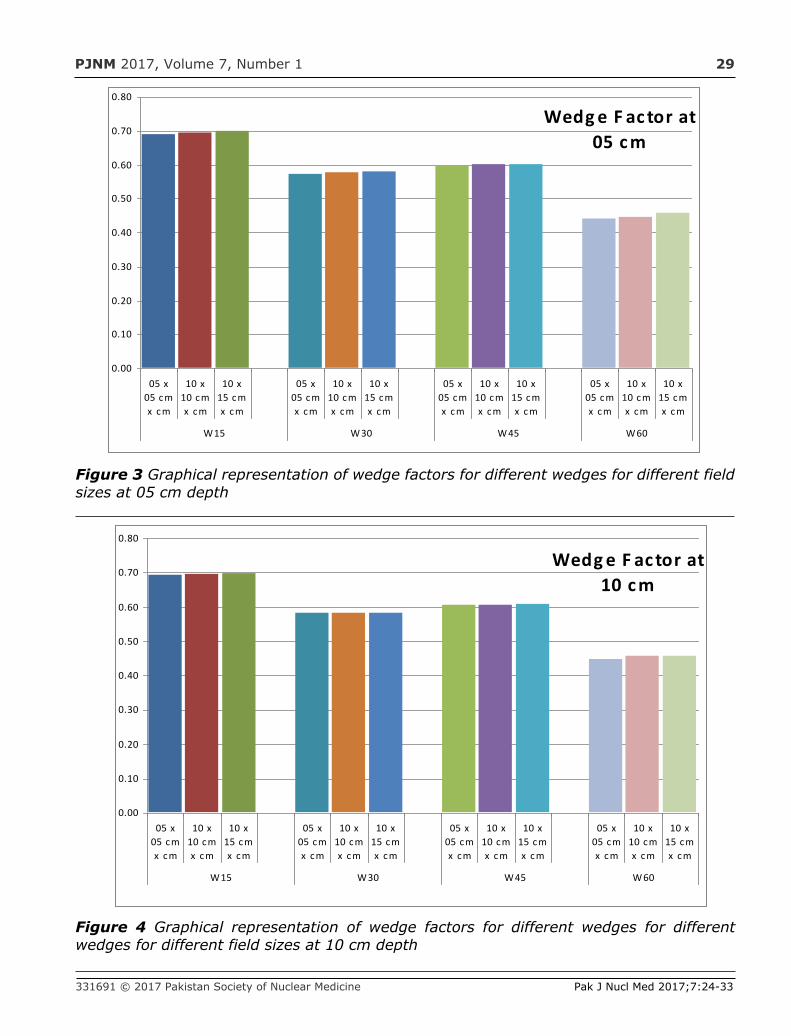
Aims The relative dosimetry plays vital part intreatment planning of patients. Factors such aspercent depth doses, tissue maximum ratios,tray factors, wedge factors, etc., determinedfrom the relative dosimetry, affects the patientdose. The current study intended at measuringand evaluating the wedge factor for different fieldsizes and depths for 60Co teletherapy unitGWXJ80 of NPIC China.
Methods The measurements for 15o, 30o, 45o
and 60o wedges for different field sizes anddepths on 60Co teletherapy unit GWXJ80 ofNPIC China installed at Nuclear Institute ofMedicine and Radiotherapy (NIMRA),Jamshoro, Pakistan, were done in waterphantom of 30x30x30 cm3 dimension at 80cm Source-to-Surface Distance (SSD) byusing calibrated Farmer’s NE 2570electrometer with NE 2571 0.6 cc ionizationchamber.
Results The evaluation of data showed thatthere was no significant difference in factor of
each of wedge being analyzed for differentfield sizes and depths.
Conclusion We The current study suggeststhat wedge factor for a particular wedge isapproximately a constant value irrespective offield size and depth. The measurement for onlyone field size at one depth is sufficient tocalculate the wedge factor for a particularwedge.
Key words: 60Co, Quality assurance,Relative dosimetry, Field size, Depth.
Introduction
In radiotherapy, absolute dosimetry or simplydosimetry, is a systemic procedure formeasuring the absorbed dose (also termed ascalibration) in unit of Gy (Gray) of teletherapymachine directly under reference conditions(same field size at same depth with constantgantry and collimator angles and at a fixedSSD). All further measurements are thencompared to this known dose under specificconditions termed as relative dosimetry [1].From these relative dosimetry variables,wedge filters are one of beam modifyingdevices and are being used to optimize thedose distribution in patients' target tissues[2-5]. Due to the presence of wedge filter inthe path of radiation beam, attenuation occursin the beam intensity which can be expressed
*Correspondence
Sajjad Ahmed Memon Nuclear Institute of Medicine & Radiotherapy (NIMRA) Jamshoro, Pakistan Tel: +92-22-9213381-84 Email: [email protected]
www.pjnm.net 2305-1630(201701/01)7:1<24:BWDFSD>2.0.TX;2-M
PJNM 2017, Volume 7, Number 1 25
in the form of wedge factor (WF) at the centralaxis of the radiation beam [2, 4]. Thisattenuation is taken into consideration forcalculating the patient dose and treatmenttime (TT) or monitor units (MU) [4-6].
Most of the times single WF is used for thepatients’ TT or MUs, with usuallymeasurements made for the reference fieldsize of 10 × 10 cm2 at reference depth of dmax
or d5 or d10 [3]. Various researchers [2-32]have conducted studies on wedge factors forLA (Linear Accelerator), 60Co (cobalt-60) orfor both type of treatment machines (LA, 60Co)as sumarized in Table 1. As seen from Table1, several studies [2, 3, 6-23] have beenconducted for LA only, whereas other studies[24-27] for both (LA and 60Co) and still otherstudies [4, 5, 28-32] for 60Co only. This studyaimed at computing and comparig thedifferences in WFs of different wedges fordifferent field sizes at different depths.
Material and Methods
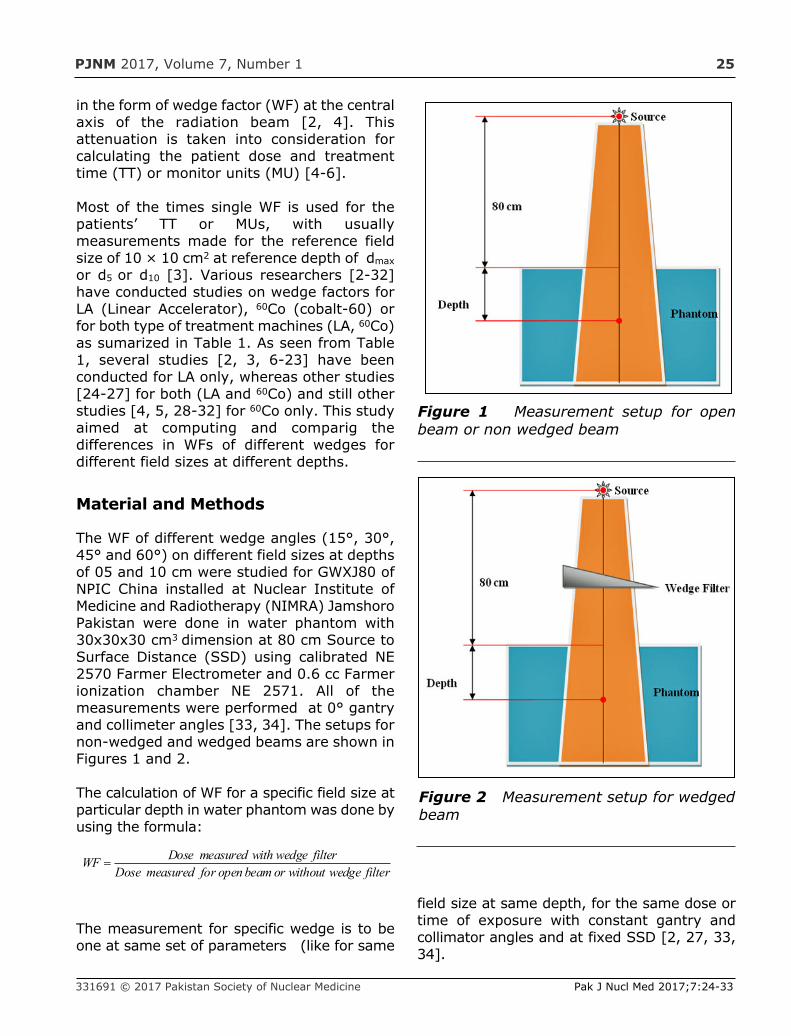
The WF of different wedge angles (15°, 30°,45° and 60°) on different field sizes at depthsof 05 and 10 cm were studied for GWXJ80 ofNPIC China installed at Nuclear Institute ofMedicine and Radiotherapy (NIMRA) JamshoroPakistan were done in water phantom with30x30x30 cm3 dimension at 80 cm Source toSurface Distance (SSD) using calibrated NE2570 Farmer Electrometer and 0.6 cc Farmerionization chamber NE 2571. All of themeasurements were performed at 0° gantryand collimeter angles [33, 34]. The setups fornon-wedged and wedged beams are shown inFigures 1 and 2.
The calculation of WF for a specific field size atparticular depth in water phantom was done byusing the formula:
The measurement for specific wedge is to beone at same set of parameters (like for same
field size at same depth, for the same dose ortime of exposure with constant gantry andcollimator angles and at fixed SSD [2, 27, 33,34].
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
filterwedgewithoutorbeamopenformeasuredDosefilterwedgewithmeasuredDoseWF =
Figure 1 Measurement setup for openbeam or non wedged beam
Figure 2 Measurement setup for wedgedbeam
PJNM 2017, Volume 7, Number 1 26
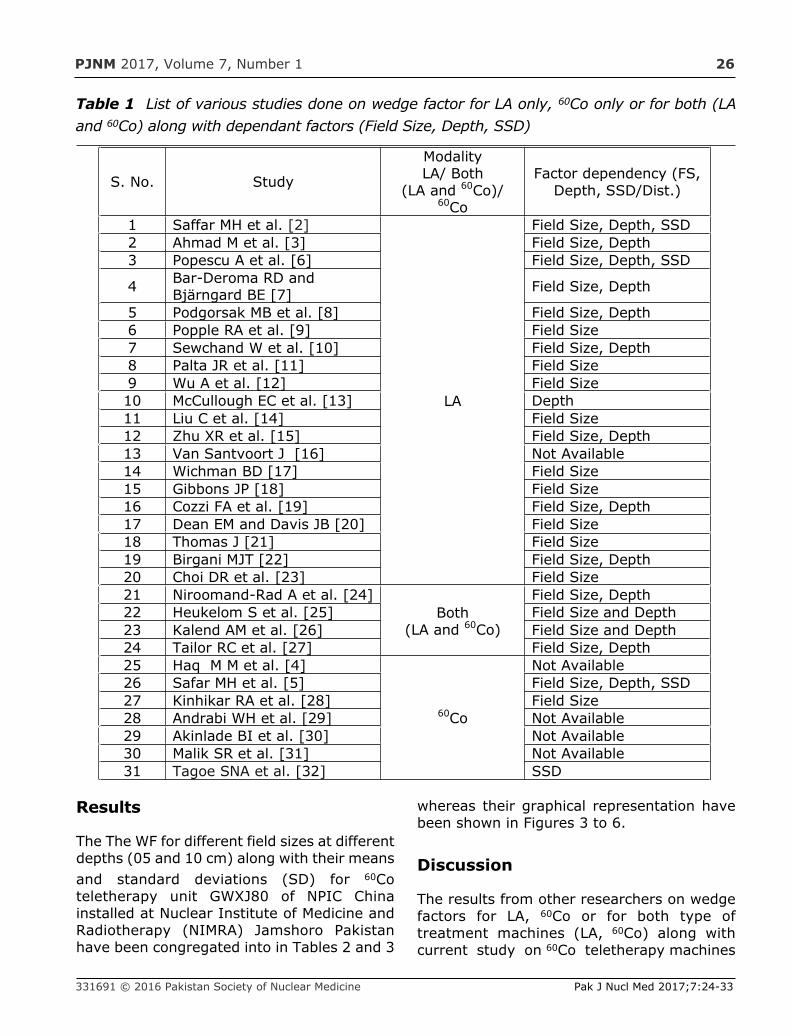
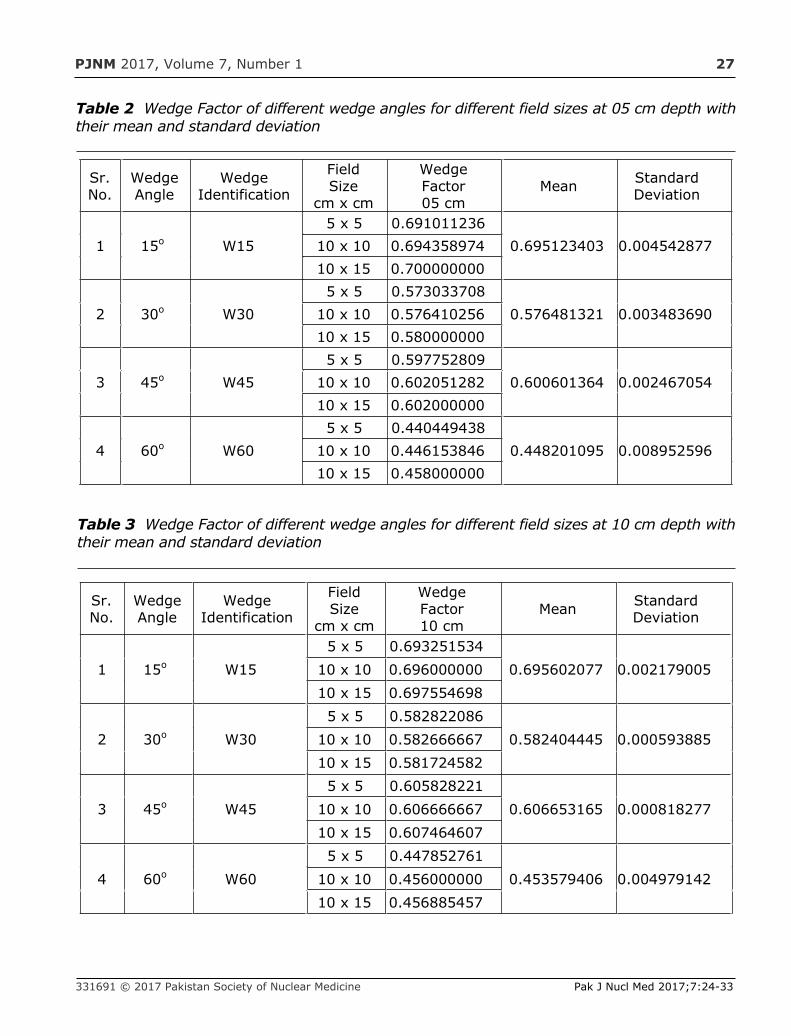
Results
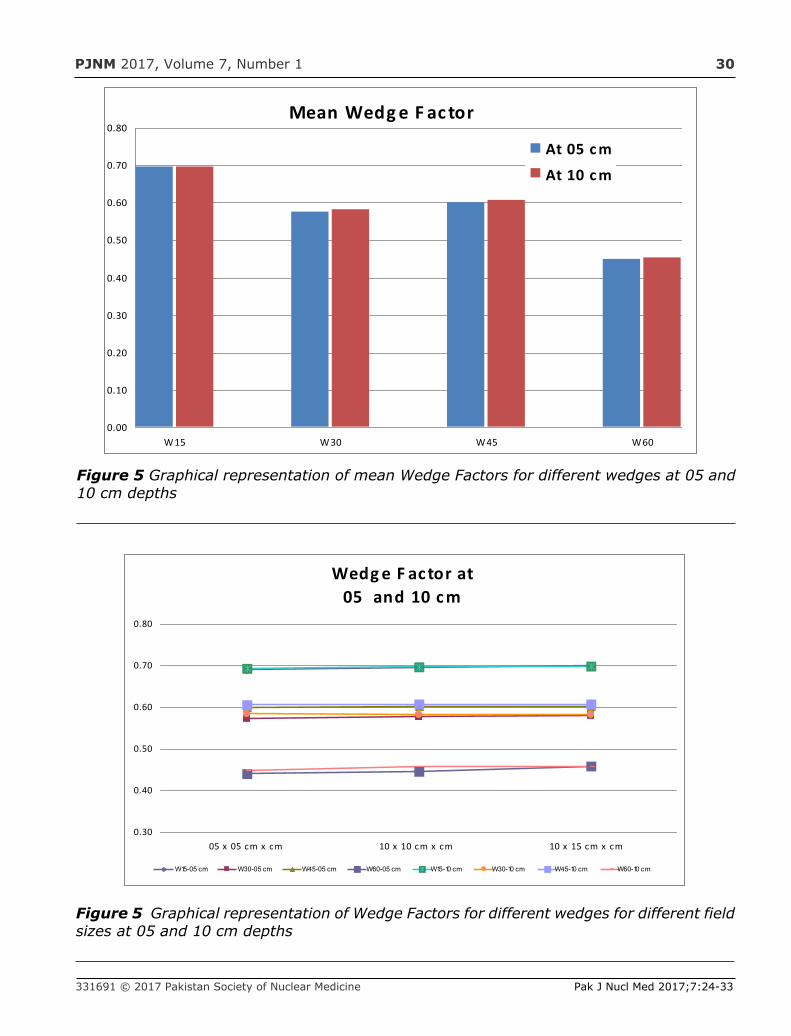
The The WF for different field sizes at differentdepths (05 and 10 cm) along with their meansand standard deviations (SD) for 60Coteletherapy unit GWXJ80 of NPIC Chinainstalled at Nuclear Institute of Medicine andRadiotherapy (NIMRA) Jamshoro Pakistanhave been congregated into in Tables 2 and 3
whereas their graphical representation havebeen shown in Figures 3 to 6.
Discussion
The results from other researchers on wedgefactors for LA, 60Co or for both type oftreatment machines (LA, 60Co) along withcurrent study on 60Co teletherapy machines
331691 © 2016 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
Table 1 List of various studies done on wedge factor for LA only, 60Co only or for both (LAand 60Co) along with dependant factors (Field Size, Depth, SSD)
S. No. Study
ModalityLA/ Both
(LA and 60Co)/60Co
Factor dependency (FS,Depth, SSD/Dist.)
1 Saffar MH et al. [2]
LA
Field Size, Depth, SSD2 Ahmad M et al. [3] Field Size, Depth3 Popescu A et al. [6] Field Size, Depth, SSD
4 Bar-Deroma RD andBjärngard BE [7] Field Size, Depth
5 Podgorsak MB et al. [8] Field Size, Depth6 Popple RA et al. [9] Field Size7 Sewchand W et al. [10] Field Size, Depth8 Palta JR et al. [11] Field Size9 Wu A et al. [12] Field Size10 McCullough EC et al. [13] Depth11 Liu C et al. [14] Field Size12 Zhu XR et al. [15] Field Size, Depth13 Van Santvoort J [16] Not Available14 Wichman BD [17] Field Size15 Gibbons JP [18] Field Size16 Cozzi FA et al. [19] Field Size, Depth17 Dean EM and Davis JB [20] Field Size18 Thomas J [21] Field Size19 Birgani MJT [22] Field Size, Depth20 Choi DR et al. [23] Field Size21 Niroomand-Rad A et al. [24]
Both(LA and 60Co)
Field Size, Depth22 Heukelom S et al. [25] Field Size and Depth23 Kalend AM et al. [26] Field Size and Depth24 Tailor RC et al. [27] Field Size, Depth25 Haq M M et al. [4]
60Co
Not Available26 Safar MH et al. [5] Field Size, Depth, SSD27 Kinhikar RA et al. [28] Field Size28 Andrabi WH et al. [29] Not Available29 Akinlade BI et al. [30] Not Available30 Malik SR et al. [31] Not Available31 Tagoe SNA et al. [32] SSD
PJNM 2017, Volume 7, Number 1 27
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
Table 2 Wedge Factor of different wedge angles for different field sizes at 05 cm depth withtheir mean and standard deviation
Sr.No.
WedgeAngle
WedgeIdentification
FieldSize
cm x cm
WedgeFactor05 cm
Mean StandardDeviation
1 15o W155 x 5 0.691011236
0.695123403 0.00454287710 x 10 0.69435897410 x 15 0.700000000
2 30o W305 x 5 0.573033708
0.576481321 0.00348369010 x 10 0.57641025610 x 15 0.580000000
3 45o W455 x 5 0.597752809
0.600601364 0.00246705410 x 10 0.60205128210 x 15 0.602000000
4 60o W605 x 5 0.440449438
0.448201095 0.00895259610 x 10 0.44615384610 x 15 0.458000000
Table 3 Wedge Factor of different wedge angles for different field sizes at 10 cm depth withtheir mean and standard deviation
Sr.No.
WedgeAngle
WedgeIdentification
FieldSize
cm x cm
WedgeFactor10 cm
Mean StandardDeviation
1 15o W155 x 5 0.693251534
0.695602077 0.00217900510 x 10 0.69600000010 x 15 0.697554698
2 30o W305 x 5 0.582822086
0.582404445 0.00059388510 x 10 0.58266666710 x 15 0.581724582
3 45o W455 x 5 0.605828221
0.606653165 0.00081827710 x 10 0.60666666710 x 15 0.607464607
4 60o W605 x 5 0.447852761
0.453579406 0.00497914210 x 10 0.45600000010 x 15 0.456885457

PJNM 2017, Volume 7, Number 1 28
[2-9, 11,13, 14, 16-19, 22,23,25, 27-32] hasbeen summarized in Table 4. As seen in thetable 4, studies [2, 3, 6-9, 11, 13, 14, 16-19,22] shows WF for LA only, whereas studies [23,25, 27] shows factor for both (LA and 60Co) andstudies [4, 5, 28-32] for 60Co only. For LA, theWF differed is between 1% to 25%, whereasfor both (LA and 60Co) and for 60Co onlyincluding current study, the difference in WFsis between 2%-9% and 0.5%-5.5%respectively.
The current study is comparable and judged toother studies done for WF for 60Co only or with
all other data available for LA, or for both (LAand 60Co). Most of the available data (speciallyfor 60Co only) did not show any significantinfluence on the Wedge factor [2, 16].
Small negligible variations within about ±2.5%for most of WF have been observed which canaffect little bit on dose of the patient. The overallerror in dose delivery to patients should not gobeyond to ±5% [33] on recommendations ofreports of International Commission onRadiation Units and Measurements (ICRU) [35,36] and the Nordic Association Of ClinicalPhysicists (NACO) [37].
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
Table 4 Wedge Factor from different researchers including current study with modality (forLA only, 60Co only or for both (LA and 60Co)
S.No. StudyModalityLA/ Both
(LA and 60Co)/60CoWF
1 Hajizadeh SM et al. [2]
LA
<2%2 Ahmad M et al. [3] <10%3 Popescu A et al. [6] <±1.0%
4 Bar-Deroma RD and Bjärngard BE[7] <±1.5%
5 Podgorsak MB et al. [8] <25%6 Popple RA et al. [9] <2%7 Palta JR et al. [11] (3.5-7)%8 McCullough EC et al. [13] (2-5)%9 Liu C et al. [14] <1%10 Van Santvoort J. [16] <3.5%11 Wichman BD. [17] (1-3)%12 Gibbons JP. [18] (1-4)%13 Cozzi FA et al. [19] <1.5%14 Birgani MJT [22] <5%15 Choi DR et al. [23] Both
(LA and 60Co)
5%16 Heukelom S. et al. [25] <9%17 Tailor RC et al. [27] (2-5)%18 Haq MM et al. [4]
60Co
<3.5%19 Safar MH et al, [5] <1%20 Kinhikar RA et al. [28] <2%21 Andrabi WH. Et al. [29] <2%22 Akinlade BI et al. [30] <5.5%23 Malik SR et al. [31] <1%24 Tagoe SNA et al. [32] <±0.50%25 Current Study <±2.5%
PJNM 2017, Volume 7, Number 1 29
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
Wedg e F ac tor at05 c m
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
05 x05 c mx c m
10 x10 c mx c m
10 x15 c mx c m
05 x05 c mx c m
10 x10 c mx c m
10 x15 c mx c m
05 x05 c mx c m
10 x10 c mx c m
10 x15 c mx c m
05 x05 c mx c m
10 x10 c mx c m
10 x15 c mx c m
W15 W 30 W 45 W 60
Figure 3 Graphical representation of wedge factors for different wedges for different fieldsizes at 05 cm depth
Figure 4 Graphical representation of wedge factors for different wedges for differentwedges for different field sizes at 10 cm depth
Wedg e F ac tor at10 c m
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
05 x05 cmx cm
10 x10 cmx cm
10 x15 cmx cm
05 x05 cmx cm
10 x10 cmx cm
10 x15 cmx cm
05 x05 cmx cm
10 x10 cmx cm
10 x15 cmx cm
05 x05 cmx cm
10 x10 cmx cm
10 x15 cmx cm
W15 W30 W45 W60
PJNM 2017, Volume 7, Number 1 30
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
Figure 5 Graphical representation of mean Wedge Factors for different wedges at 05 and10 cm depths
Mean Wedg e F ac tor
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
W15 W30 W45 W60
At 05 c m
At 10 c m
Figure 5 Graphical representation of Wedge Factors for different wedges for different fieldsizes at 05 and 10 cm depths
Wedg e F ac tor at05 and 10 c m
0.30
0.40
0.50
0.60
0.70
0.80
05 x 05 cm x cm 10 x 10 cm x cm 10 x 15 cm x cm
W15-05 cm W30-05 cm W45-05 cm W60-05 cm W15-10 cm W30-10 cm W45-10 cm W60-10 cm
PJNM 2017, Volume 7, Number 1 31
Conclusion
The current study presents a comparison ofWF for Wedges supplied with the teletherapyunit. The data evaluation showed that nonsignificant difference in WF of each of wedgebeing analyzed for different field sizes atdifferent depths. This study suggested thatWF for a specific wedge is approximately aconstant ratio irrespective of field size anddepth. The measurement for only one fieldsize at one depth is adequate to calculate theWF for a specific wedge.
Acknowledgement
The authors wish to thank Mr. Wajid HussainPT and Mr. Abdul Qadeer SSA for theirassistance and helping in takingmeasurements on teletherapy machine,without their help the current study cannot besuccessfully completed.
References
1. Interntional Atomic Energy Association (IAEA)https://rpop.iaea.org/RPOP/RPoP/Content/Documents/.../RT02_Phys2_Equip_WEB.ppt.
2. Saffar MH, Ghavamnasiri MR, GholamhosseinianH. Assessment of variation of wedge factor withdepth, field size and SSD for Neptun 10PC Linac inMashhad Imam Reza Hospital. Iran J Radiat Res2004; 2(2):53-8.
3. Ahmad M, Hussain A, Muhammad W, Rizvi SQA,Matiullah. Studying wedge factors and beamprofiles for physical and enhanced dynamicwedges. J Med Phys 2010 Jan-Mar; 35(1):33-41.doi:10.4103/0971-6203.57116.
4. Haq MM, Rehman M, Ahmad A, Khan NA, Ayub M,Ahmad S. Installation, commissioning and qualityassurance tests of first Indian made tele-therapyCobalt machine (Bhabhatron- II) at Sher-I-KashmirInstitute Of Medical Sciences, Srinagar, Jammu AndKashmir. JK- Prac 2014; 19(3-4):93-9.
5. Safar MH, Ghavamnasiri MR, GholamhosseinianH. Study of wedge factor dependence with depth,
field size and SSD in 60Co units. Iran J Bas MedSci Spring 2005; 8(1):4-8.
6. Popescu A, Lai K, Singer K, Phillips M. Wedgefactor dependence with depth, field size, andnominal distances: A general computational rule.Med Phys 1999; 26:541-9.Doi:http://dx.doi.org/10.1118/1.598555
7. Bar-Deroma RD and Bjärngard BE. The relationbetween wedge factors in air and water. Med Phys1994; 21:1043-7.Doi:http://dx.doi.org/10.1118/1.597346
8. Podgorsak MB, Kubsand SS, Paliwal BR.Dosimetry of large wedged highenergy photonbeams. Med Phys 1993; 20:369-73.
9. Popple RA, Brezovich IA, Duan J, Shen S, PareekPN and Ye SJ. Determination of field sizedependent wedge factors from a few selectedmeasurements. J App Clin Med Phys Winter 2005;6(1):51
10. Sewchand W, Khan FM, Williamson J. Variationin depth dose data between open and wedgedfields for 4-MV X-rays. Radiol 1978; 127(3):789-92. Doi:http://dx.doi.org/10.1148/127.3.789
11. Palta JR, Daftari I, Suntharalingam N. Field sizedependence of wedge factors. Med Phys 1988;1 5 : 6 2 4 - 6 .Doi:http://dx.doi.org/10.1118/1.596217
12. Wu A, Zwicher RD, Krasin F, Sternick ES.Dosimetry characteristics of large wedges for 4and 6 MV X-rays. Med Phys 1984; 11:186-8.
13. McCullough EC, Gortney J, Blackwell RC. A depthdependence determination of wedge transmissionfactor for 4-10 MV photon beams. Med Phys1988; 15(4):621-3.Doi:http://dx.doi.org/10.1118/1.596216
14. Liu C, Li Z, Palta JR. Characterizing output for theVarian enhanced dynamic wedge field. Med Phys1998; 25:64-70. DOI:10.1118/1.598161
15. Zhu XR, Gillin MT, Jursinic PA, Lopez F, Grimm DF,Rownd JJ. Comparison of dosimetriccharacteristics of siemens virtual and physicalwedges. Med Phys 2000; 26:2267-77.Doi:http://dx.doi.org/10.1118/1.1312813
16. Van Santvoort J. Dosimtric evaluation of theSiemens virtual wedge. Phy Med Biol 1998;43:2651-63.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
PJNM 2017, Volume 7, Number 1 32
17. Wichman BD. A spreadsheet solution for off-axis,noncentral enhanced dynamic wedge factor. JAppl Clin Med Phys 2003; 4(3):217-23.Doi:http://dx.doi.org/10.1120/jacmp.v4i3.2518
18. Gibbons JP. Calculation of enhanced dynamicwedge factors for symmetric and asymmetricphoton fields. Med Phy 1998; 25:1411-8.Doi:http://dx.doi.org/10.1118/1.598313s
19. Cozzi FA, Cozzi L, Garavaglia G..Wedge factors:dependence on depth and field size. RadiotherOncol 1996; 39:31-4. doi:10.10160167-8140(95)01714-3
20. Dean EM and Davis JB. The variation of wedgefactors with field size on a linear accelerator withwedge tray beneath secondary collimator. Br JRadiol 1991; 64:184-5. DOI:10.1259/0007-1285-64-758-184.
21. Thomas J. The variation of wedge factors withfield size on a linear accelerator. Br J Radiol 1990;63:355-6. doi: http://dx.doi.org/10.1259/0007-1285-63-749-355
22. Birgani MJT, Behrooz MA, Zabihzadeh M,Eskandari SR, Khezerloo D. Jundishapur.Analytical Method for Determination of WedgeFactors Dependency of Field Size and Depth for6MV & 18MV Photon Beams In Siemens PrimiusPlus Accelerator. Jundishapur Sci Med J 2013;11(6):597-608.
23. Choi R, Ahn YC, Huh SJ. Clinical application ofwedge factor. Radiat Oncolo J 1995; 13(3):291-6.
24. Niroomand-Rad A, Haleem M, Rodgers J,Obcemea C. Wedge factor dependence on depthand field size for various beam energies usingsymmetric and half collimated asymmetric jawsettings. Med Phys 1992; 19:1445-50.Doi:http://dx.doi.org/1 0.1118/ 1.596800
25. Heukelom ., Lanson J., Mijnheer BJ. Wedgefactor constituents of high energy photonbeams: Head and phantom scatter dosecomponents. Radiother Oncol 1994; 32:73-83.Doi:10.1016/0167-8140(94)90011-6
26. Kalend AM, Wu A, Yoder V, Maitz A. Separationof dose gradient effect from beam hardeningeffect on wedge factors in photon fields. MedPhys 1990; 17:701-4. DOI:10.1118/1.596469
27. Tailor RC, Followill DS, Hanson WF. A first orderapproximation of field size and depthdependence of wedge transmission. Med Phys1998; 25:241-4.Doi:http://dx.doi.org/10.1118/1.598187
28. Kinhikar RA, Sharma S, Upteti R, Tambe CM,Deshpande DD, Shrivastav SK, et al.Commissioning of motorized wedge for the firstEquinox-80 telecobalt unit and implementationin the Eclipse 3D treatment planning system.Australas Phy Eng Sci Med 2007; 30(2):127-37.DOI: 10.1007/BF03178417
29. Andrabi WH, Koul SK, Kharadi MY, Abbas SM,Bhutt MA, Sofi AG, Ashraf M, Maqbool M, AfrozF, Ahmad B. Installation, commissioning andquality assurance of cobalt unit (Theratron 780E)at SKIMS, Soura, Srinagar. JK- Pract 2004;11(2):144-8.
30. Akinlade BI, Oyekunle EO, Adenipekun AA,Elumelu-Kupoluyi TN, Folasire AM. DosimetricVerification of Bhabhatron-II Telecobalt Unit atthe University College Hospital, Ibadan, Nigeria.Cancer Biology 2014; 4(2):16-21
31. Malik SR, Rahman M, Mia M, Bairagi AJAK, RezaS, Ahmed M and Yeasmin N. Comprehensivebenchmark procedures for commissioning,quality assurance and treatment delivery forquality cancer therapy using 60Co teletherapymachine. Bangla J Med Phys 2013; 6(1):3-20.Doi: http://dx.doi.org/10.3329/ bjmp.v6i1.19752
32. Tagoe SNA, Nani EK, Addison EKT, Andam A.Dependence of wedge transmission factor on60Co teletherapy treatment depths andtechniques. J Appl Sci and Techno 2011; 16(1-2):127-35. Doi:http://dx.doi.org/ 10.4314/jast.v16i1-2.64790
33. Memon SA, Cheema AA, Laghari NA, Mangi FH.Dose measurement of Cobalt-60 radiotherapybeams in treatment fields. J Ayub Med CollAbbottabad 2014; 26(3):279-82
34. Memon SA, Laghari NA, Mangi FH, Ahmad F,Hussain MM, Palijo S, Jhatyal N and Adeel A.Analysis and verification of percent depth doseand tissue maximum ratio for 60Co gamma raybeam, World Appl Sci J 2015; 33(1):109-13.Doi:10.5829/idosi.wasj.2015.33.01.9261.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:24-33
PJNM 2017, Volume 7, Number 1 33
35. International Commission on Radiation Unitsand Measurements. Determination ofabsorbed dose in a patient irradiated bybeams of X or gamma-ray radiotherapyprocedures". ICRU Report No. 24, USA:ICRU; 1976.
36. International Commission on Radiation Unitsand Measurements. Prescribing, recordingand reporting photon beam therapy. Report50, USA: ICRU; 1993.
37. Nordic Association of Clinical Physicist.Specification of dose delivery in radiationtherapy. NACP; 1994.
Pak J Nucl Med 2017;7:24-33 2305-1630(201701/01)7:1<24:BWDFSD>2.0.TX;2-M
PJNM 2017; 7:34-42 331691 © 2017 Pakistan Society of Nuclear Medicine
Pre-operative cardiac risk stratification for non-cardiac surgery in cancer patients using myocardial
perfusion scintigraphy
Iqbal Munir*,1, Amrah Javaid2, Khalid Nawaz3, MohammedHathaf Al-Rowaily4, Muaadh Abdualrehman Al-Asbahi1
1Department of Nuclear Medicine, Al Takhassussi Hospital,Dr. Sulaiman Al Habib Medical Group, Riyadh, KSA
2Department of Basic Health Sciences, College of Medicine,Princess Noura Binta Abdulrehman University for Women, Riyadh, KSA3Departemnt of Nuclear Medicine, Shaukat Khanum Memorial Cancer
Hospital and Research Center, Lahore, Pakistan4Department of Chemistry, Pavia University, Italy
ORIGINAL ARTICLE
Abstract
Aims Cancer patients are at a higher risk forany cardiac event during and post surgery, dueto an altered coagulation state and anaemia, andcan have additive effect if the patient hadprevious history of any cardiac event or riskfactor for coronary artery disease such ashypertension and diabetes. The objective of thisstudy was evaluate the usefulness of gatedmyocardial perfusion scintigraphy withpharmacological stress in determining thefrequency of cardiac events associated withnon-cardiac surgery in cancer patients.
Methods 100 consecutive patients, who werebeing planned for the oncological surgery,were enrolled in this study for preoperativegated myocardial perfusion scintigraphy using99mTc-sestamibi with adenosine stress. Afteracquiring the data, perfusion images werereconstructed and analysed using visualassessment as well as QPS program andsummed stress score (SSS) was obtained.Based on visual assessment and SSS, wedivided patients into low- and high-riskgroups. Postoperative follow-up of thepatients was done through internal medicineclinics.
Results Out of 100 patients, 57 were femaleand 43 male with a mean age 61.25 years.Sixty-three (63%) had a history of diabetes,73% hypertension, 34% were known smokerswhile 42% had a family history of coronaryartery disease and 15 patients has CAD. 61%fell into the low-risk group and thirty-nine(39%) in the high-risk group. In the low-risk
*Correspondence
Iqbal Munir Department of Nuclear Medicine Al Takhassussi Hospital Dr. Sulaiman Al Habib Medical Group P.O. Box 2000, Riyadh 11393, KSA Email: [email protected]
www.pjnm.net 2305-1630(201701/01)7:1<34:PCRSNC>2.0.TX;2-M
PJNM 2017, Volume 7, Number 1 35
1 patient (1.63%) needed inotropic supportpostoperatively. In the high-risk group, 6(15.38%) patients had cardiac eventspostoperatively. Subset-analysis of theseshowed; 3 (7.69%) had an episode of anginaprior to discharge, 2 (5.12%) died withcardiac-arrest due to myocardial infraction(MI) and 1 (2.56%) needed inotropic supportpostoperatively and surgery was deferred in4 patients due to their very low LVEF and highSSS. These 4 patients were further evaluatedby cardiologist for future management.
Conclusion In low-risk group patients, stressmyocardial perfusion scintigraphy has a highnegative predictive value for peri- and post-operative cardiac events in cancer patients. Whilepatients with cancer and labelled as high-risk onmyocardial perfusion imaging, whetherdemonstrating scar or ischaemia, should promptappropriate peri- and post-operativemanagement to minimize major cardiac events.
Key words: Myocardial perfusionscintigraphy, Pre-operative risk assessment,99mTc-sestamibi, Pharmacological stress,Adenosine, Coronary artery disease
Introduction
Coronary artery disease (CAD) is the leadingcause of death with no limitation to geographicboundaries accounting for about 16.7 milliondeaths worldwide [1]. Cancer by itself isassociated with coagulation disorders due tohypercoagulable state and can cause coronarythromboemboli. However, there is no definiteevidence that cancer by itself or any particulartumour type predisposes to coronaryatherosclerosis [2]. No single test candiagnose or stratify the risk of having CAD.The evidence that myocardial perfusionimaging (MPI), has a strong prognostic value,is overwhelming [3] because of its higherdiagnostic sensitivity and specificity thanexercise electrocardiography (80% and 92%vs. 64% and 82% respectively) for coronaryartery disease [4]. MPI is also used forassessing the functional importance of known
coronary stenoses risk stratification beforemajor non-cardiac surgery [5].
Gated stress MPS is the most commonly usedand well documented noninvasive method forrisk stratification. It is most cost-effective inpatients with a clinically intermediate risk ofa subsequent cardiac event [6]. According toACC/AHA 2007 Guidelines on perioperativecardiovascular evaluation and care for non-cardiac surgery in patients with known CADor the new onset of signs or symptomssuggestive of CAD, baseline cardiacassessment should be performed [7].
The surgery-specific cardiac risk of non-cardiac surgery is related to two importantfactors. First, the type of surgery by itself, andsecond, the likelihood of underlying heartdisease. Pharmacologic testing with MIBISPECT has been used to assess risk of futurecardiac events in patients in a stable conditionunable to perform an exercise test. Anabnormal MIBI study is reported to be thestrongest independent predictor of increasedrisk of nonfatal MI or cardiac death (oddsratio, 10.0; 95% CI, 2.3 to 43.0) [8]. Severalstudies have assessed the perioperative andlong-term prognostic value of dipyridamoleMIBI imaging in vascular surgery patients.Literature review suggests that dipyridamole,adenosine, and dobutamine testing with MIBIimaging may be effective for perioperative andlong-term risk stratification in some patientsundergoing non-cardiac surgery [9]. However,more studies are needed to better definewhich patients may benefit from testing basedon clinical risk factors and type of surgery etc.The purpose of this study was to evaluate theusefulness of gated myocardial perfusionscintigraphy (G-SPECT) with Adenosinepharmacological stress for determining thefrequency of cardiac event associated withnon-cardiac surgery in cancer patients.
Methods
We conducted a cross sectional observationalstudy at our department. We included 100cancer patients fulfilling the inclusion criteria
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
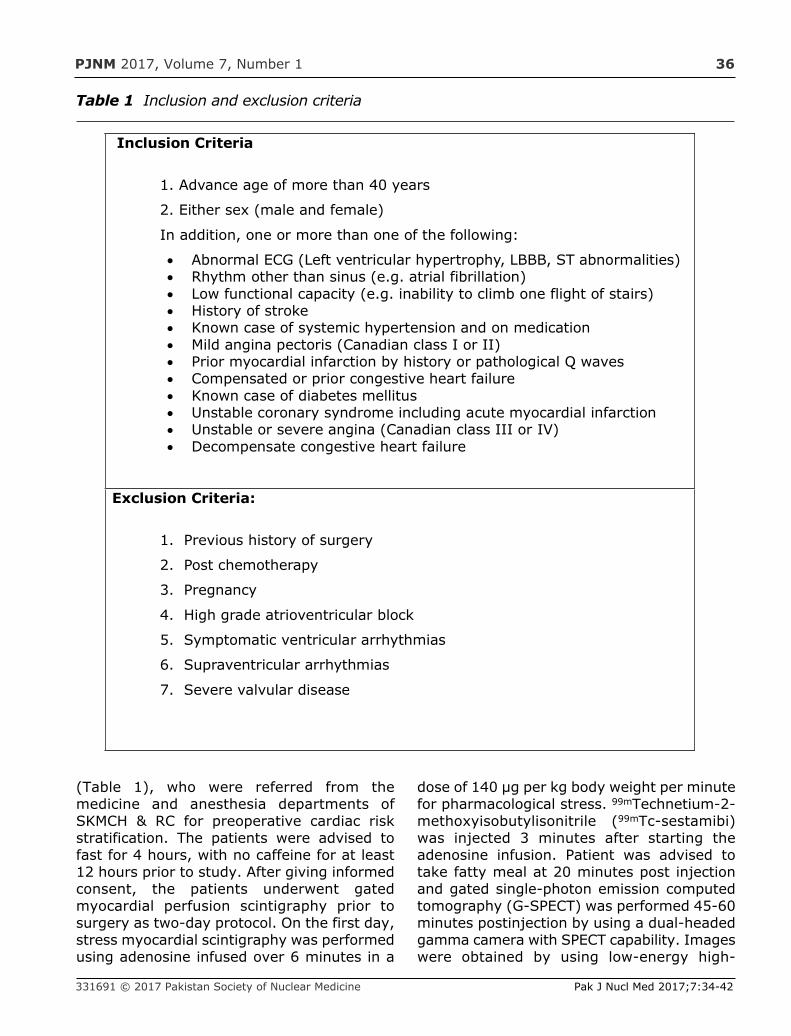
PJNM 2017, Volume 7, Number 1 36
(Table 1), who were referred from themedicine and anesthesia departments ofSKMCH & RC for preoperative cardiac riskstratification. The patients were advised tofast for 4 hours, with no caffeine for at least12 hours prior to study. After giving informedconsent, the patients underwent gatedmyocardial perfusion scintigraphy prior tosurgery as two-day protocol. On the first day,stress myocardial scintigraphy was performedusing adenosine infused over 6 minutes in a
dose of 140 µg per kg body weight per minutefor pharmacological stress. 99mTechnetium-2-methoxyisobutylisonitrile (99mTc-sestamibi)was injected 3 minutes after starting theadenosine infusion. Patient was advised totake fatty meal at 20 minutes post injectionand gated single-photon emission computedtomography (G-SPECT) was performed 45-60minutes postinjection by using a dual-headedgamma camera with SPECT capability. Imageswere obtained by using low-energy high-
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
Table 1 Inclusion and exclusion criteria
Inclusion Criteria
1. Advance age of more than 40 years
2. Either sex (male and female)
In addition, one or more than one of the following:
· Abnormal ECG (Left ventricular hypertrophy, LBBB, ST abnormalities)· Rhythm other than sinus (e.g. atrial fibrillation)· Low functional capacity (e.g. inability to climb one flight of stairs)· History of stroke· Known case of systemic hypertension and on medication· Mild angina pectoris (Canadian class I or II)· Prior myocardial infarction by history or pathological Q waves· Compensated or prior congestive heart failure· Known case of diabetes mellitus· Unstable coronary syndrome including acute myocardial infarction· Unstable or severe angina (Canadian class III or IV)· Decompensate congestive heart failure
Exclusion Criteria:
1. Previous history of surgery
2. Post chemotherapy
3. Pregnancy
4. High grade atrioventricular block
5. Symptomatic ventricular arrhythmias
6. Supraventricular arrhythmias
7. Severe valvular disease

PJNM 2017, Volume 7, Number 1 37
high-resolution collimators. Energy window20% was centered at 140 keV with matrix sizeof 64 X 64.
SPECT was obtained by step and shootmethod, 1800 of motion arc, 450 right anterioroblique (RAO) to 135o left posterior oblique(LPO) with 32 projections, each of 30-secondduration per projection, 8 frame perprojection. Gated SPECT was obtained by ECGsynchronized data collection. Images werereconstructed by using QPS/QGS software.
Stress and rest scan images was sliced intothree planes: short axis (SA), horizontal longaxis (HLA) and vertical long axis (VLA). Polarmap (bull’s eye) was used for quantitativeperfusion defects analysis and 20-segmentsummed stress score (SSS) was calculated.
If there was evidence of a perfusion defect instress scintigraphy, the patient was called infor rest scintigraphy the next day. Both thestress and the rest images were processedtogether to see evidence of reperfusion. Postscintigraphy risk stratification was mentionedin the report on the basis of 20-segmentsummed stress score (SSS).
The patient was followed up and observed forany cardiac related event (e.g., cardiac death,myocardial ischaemia, heart failure, fatalarrhythmia, unstable angina, etc.) peri andpost operatively up to 2 weeks, and thesewere documented.
Statistical Analysis
The data analysis was carried out usingcomputer based Statistical Package for SocialSciences (SPSS) version 14. Quantitativevariables such as age and qualitative variablessuch as sex (male/female), diabetes,hypertension, body mass index, LVEF > 55%and final conclusion, i.e. per-operative cardiacevent (Yes/No) and post-operative cardiacevent (Yes/No) was presented by calculatingthe frequency and percentage. Correlation ofany cardiac event (peri- and post-operatively)was made with the post-scintigraphic riskstratification.
Results
Out of 100 patients, 43 were male and 57female with ages ranging from 41-88 yearswith a the mean age of 61.25 years. Thirty-eight patients were operated on for breastcancer, 10 for colon cancer, 8 for lung cancer,6 stomach cancer, 5 for oesophageal cancer,5 for renal cell carcinoma (RCC), 4 forhepatocellular cancer (HCC), and 24 for othercancers which included cervical, ovarian,tongue, pancreatic and thyroid cancers.
Sixty-three percent of that patients had ahistory of diabetes, 73% were hypertensive,34% were known smokers whilst 42% hadfamily history of coronary artery disease and15% patients has CAD, 59% had body massindex (BMI) more than 25 while 41% had BMIless than 25.
Following data acquistion, QPS software wasused for quantitative analysis includingcalculation of summed stress score (SSS). Outof total 100 patients, 61 had a SSS ≤4 (Figure1), which was considered as normal while 39had SSS ≥5 (Figure 2). On subset analysis ofthese 39 patients, 15 had SSS between 5-8,which was considered as mildly abnormal, 20patient had SSS between 9-13 which wasconsidered as moderately abnormal and 4patients had SSS more than 13 which wasconsidered as severely abnormal. On the samestress MPI, QGS software was used tocalculate the left ventricular ejection fraction(LVEF). Minimum LVEF was 22% andmaximum LVEF was 87%. 18 out of 100patients had LVEF less than 55%. On the basisof SSS and LVEF out of 100, 39 patients fellinto high-risk group for peri- and post-operative cardiac events while 61 patientswere assigned in to the low-risk group forcardiac events. On subset analysis of low-riskgroup, only one patient out of 61 patients(1.63%) needed inotropic support postoperatively (Figure 3). This patient had SSSof 3 and a LVEF 49% on MPI. The patient wasa 73-year-old male with risk factors for CADincluding diabetes, hypertension, smokingwith positive family history for CAD but noprevious history of CAD.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
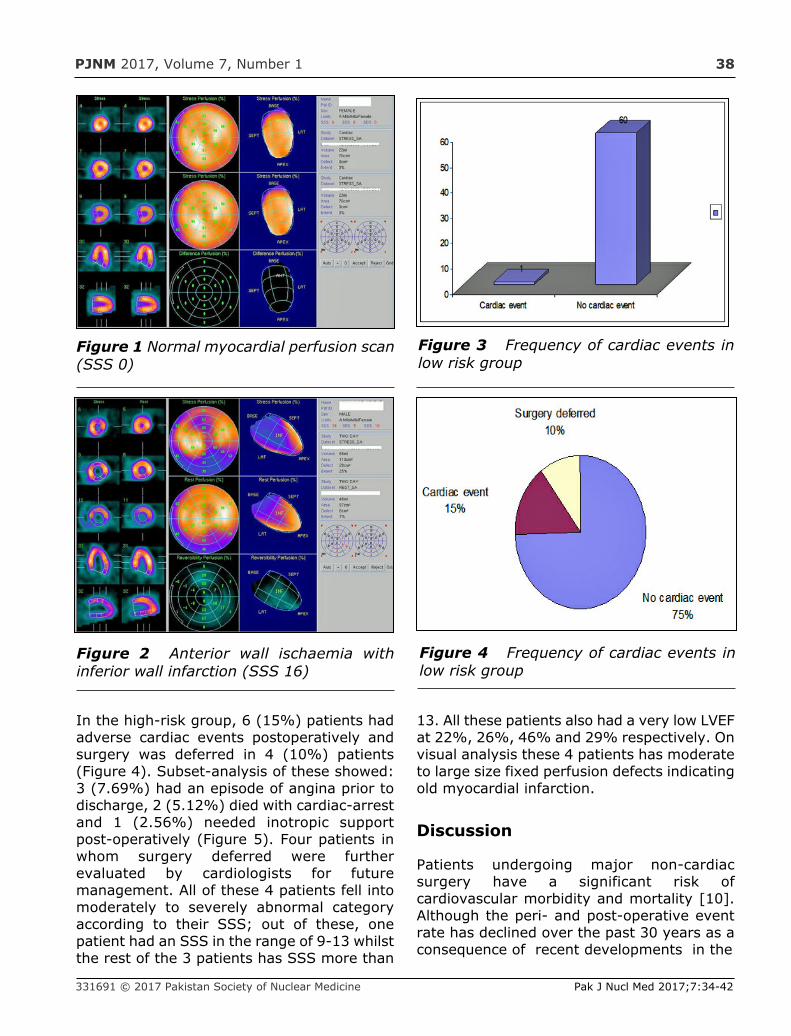
PJNM 2017, Volume 7, Number 1 38
In the high-risk group, 6 (15%) patients hadadverse cardiac events postoperatively andsurgery was deferred in 4 (10%) patients(Figure 4). Subset-analysis of these showed:3 (7.69%) had an episode of angina prior todischarge, 2 (5.12%) died with cardiac-arrestand 1 (2.56%) needed inotropic supportpost-operatively (Figure 5). Four patients inwhom surgery deferred were furtherevaluated by cardiologists for futuremanagement. All of these 4 patients fell intomoderately to severely abnormal categoryaccording to their SSS; out of these, onepatient had an SSS in the range of 9-13 whilstthe rest of the 3 patients has SSS more than
13. All these patients also had a very low LVEFat 22%, 26%, 46% and 29% respectively. Onvisual analysis these 4 patients has moderateto large size fixed perfusion defects indicatingold myocardial infarction.
Discussion
Patients undergoing major non-cardiacsurgery have a significant risk ofcardiovascular morbidity and mortality [10].Although the peri- and post-operative eventrate has declined over the past 30 years as aconsequence of recent developments in the
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
Figure 1 Normal myocardial perfusion scan(SSS 0)
Figure 2 Anterior wall ischaemia withinferior wall infarction (SSS 16)
Figure 3 Frequency of cardiac events inlow risk group
Figure 4 Frequency of cardiac events inlow risk group
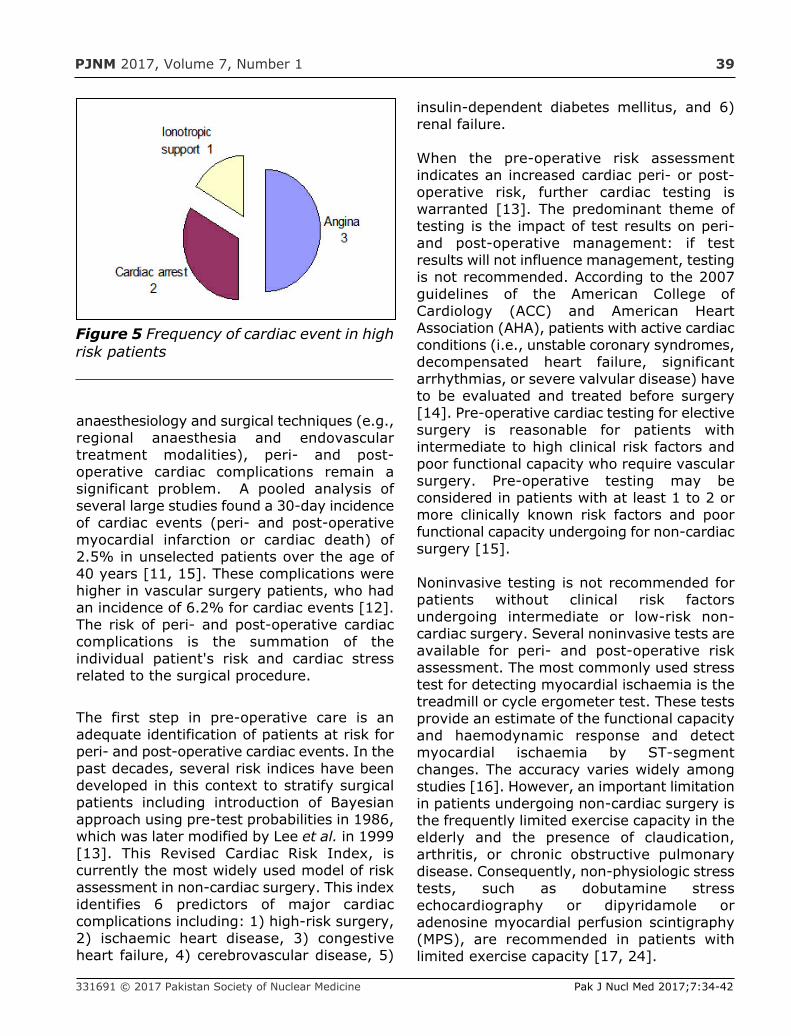
PJNM 2017, Volume 7, Number 1 39
anaesthesiology and surgical techniques (e.g.,regional anaesthesia and endovasculartreatment modalities), peri- and post-operative cardiac complications remain asignificant problem. A pooled analysis ofseveral large studies found a 30-day incidenceof cardiac events (peri- and post-operativemyocardial infarction or cardiac death) of2.5% in unselected patients over the age of40 years [11, 15]. These complications werehigher in vascular surgery patients, who hadan incidence of 6.2% for cardiac events [12].The risk of peri- and post-operative cardiaccomplications is the summation of theindividual patient's risk and cardiac stressrelated to the surgical procedure.
The first step in pre-operative care is anadequate identification of patients at risk forperi- and post-operative cardiac events. In thepast decades, several risk indices have beendeveloped in this context to stratify surgicalpatients including introduction of Bayesianapproach using pre-test probabilities in 1986,which was later modified by Lee et al. in 1999[13]. This Revised Cardiac Risk Index, iscurrently the most widely used model of riskassessment in non-cardiac surgery. This indexidentifies 6 predictors of major cardiaccomplications including: 1) high-risk surgery,2) ischaemic heart disease, 3) congestiveheart failure, 4) cerebrovascular disease, 5)
insulin-dependent diabetes mellitus, and 6)renal failure.
When the pre-operative risk assessmentindicates an increased cardiac peri- or post-operative risk, further cardiac testing iswarranted [13]. The predominant theme oftesting is the impact of test results on peri-and post-operative management: if testresults will not influence management, testingis not recommended. According to the 2007guidelines of the American College ofCardiology (ACC) and American HeartAssociation (AHA), patients with active cardiacconditions (i.e., unstable coronary syndromes,decompensated heart failure, significantarrhythmias, or severe valvular disease) haveto be evaluated and treated before surgery[14]. Pre-operative cardiac testing for electivesurgery is reasonable for patients withintermediate to high clinical risk factors andpoor functional capacity who require vascularsurgery. Pre-operative testing may beconsidered in patients with at least 1 to 2 ormore clinically known risk factors and poorfunctional capacity undergoing for non-cardiacsurgery [15].
Noninvasive testing is not recommended forpatients without clinical risk factorsundergoing intermediate or low-risk non-cardiac surgery. Several noninvasive tests areavailable for peri- and post-operative riskassessment. The most commonly used stresstest for detecting myocardial ischaemia is thetreadmill or cycle ergometer test. These testsprovide an estimate of the functional capacityand haemodynamic response and detectmyocardial ischaemia by ST-segmentchanges. The accuracy varies widely amongstudies [16]. However, an important limitationin patients undergoing non-cardiac surgery isthe frequently limited exercise capacity in theelderly and the presence of claudication,arthritis, or chronic obstructive pulmonarydisease. Consequently, non-physiologic stresstests, such as dobutamine stressechocardiography or dipyridamole oradenosine myocardial perfusion scintigraphy(MPS), are recommended in patients withlimited exercise capacity [17, 24].
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
Figure 5 Frequency of cardiac event in highrisk patients
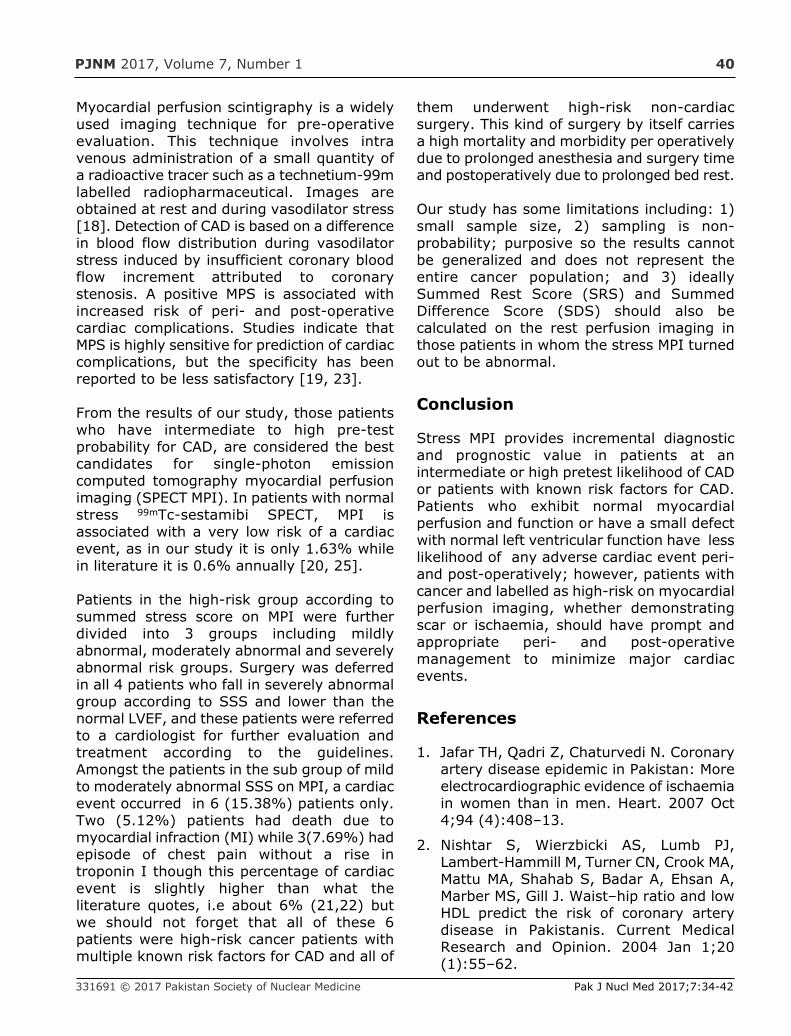
PJNM 2017, Volume 7, Number 1 40
Myocardial perfusion scintigraphy is a widelyused imaging technique for pre-operativeevaluation. This technique involves intravenous administration of a small quantity ofa radioactive tracer such as a technetium-99mlabelled radiopharmaceutical. Images areobtained at rest and during vasodilator stress[18]. Detection of CAD is based on a differencein blood flow distribution during vasodilatorstress induced by insufficient coronary bloodflow increment attributed to coronarystenosis. A positive MPS is associated withincreased risk of peri- and post-operativecardiac complications. Studies indicate thatMPS is highly sensitive for prediction of cardiaccomplications, but the specificity has beenreported to be less satisfactory [19, 23].
From the results of our study, those patientswho have intermediate to high pre-testprobability for CAD, are considered the bestcandidates for single-photon emissioncomputed tomography myocardial perfusionimaging (SPECT MPI). In patients with normalstress 99mTc-sestamibi SPECT, MPI isassociated with a very low risk of a cardiacevent, as in our study it is only 1.63% whilein literature it is 0.6% annually [20, 25].
Patients in the high-risk group according tosummed stress score on MPI were furtherdivided into 3 groups including mildlyabnormal, moderately abnormal and severelyabnormal risk groups. Surgery was deferredin all 4 patients who fall in severely abnormalgroup according to SSS and lower than thenormal LVEF, and these patients were referredto a cardiologist for further evaluation andtreatment according to the guidelines.Amongst the patients in the sub group of mildto moderately abnormal SSS on MPI, a cardiacevent occurred in 6 (15.38%) patients only.Two (5.12%) patients had death due tomyocardial infraction (MI) while 3(7.69%) hadepisode of chest pain without a rise introponin I though this percentage of cardiacevent is slightly higher than what theliterature quotes, i.e about 6% (21,22) butwe should not forget that all of these 6patients were high-risk cancer patients withmultiple known risk factors for CAD and all of
them underwent high-risk non-cardiacsurgery. This kind of surgery by itself carriesa high mortality and morbidity per operativelydue to prolonged anesthesia and surgery timeand postoperatively due to prolonged bed rest.
Our study has some limitations including: 1)small sample size, 2) sampling is non-probability; purposive so the results cannotbe generalized and does not represent theentire cancer population; and 3) ideallySummed Rest Score (SRS) and SummedDifference Score (SDS) should also becalculated on the rest perfusion imaging inthose patients in whom the stress MPI turnedout to be abnormal.
Conclusion
Stress MPI provides incremental diagnosticand prognostic value in patients at anintermediate or high pretest likelihood of CADor patients with known risk factors for CAD.Patients who exhibit normal myocardialperfusion and function or have a small defectwith normal left ventricular function have lesslikelihood of any adverse cardiac event peri-and post-operatively; however, patients withcancer and labelled as high-risk on myocardialperfusion imaging, whether demonstratingscar or ischaemia, should have prompt andappropriate peri- and post-operativemanagement to minimize major cardiacevents.
References
1. Jafar TH, Qadri Z, Chaturvedi N. Coronaryartery disease epidemic in Pakistan: Moreelectrocardiographic evidence of ischaemiain women than in men. Heart. 2007 Oct4;94 (4):408–13.
2. Nishtar S, Wierzbicki AS, Lumb PJ,Lambert-Hammill M, Turner CN, Crook MA,Mattu MA, Shahab S, Badar A, Ehsan A,Marber MS, Gill J. Waist–hip ratio and lowHDL predict the risk of coronary arterydisease in Pakistanis. Current MedicalResearch and Opinion. 2004 Jan 1;20(1):55–62.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
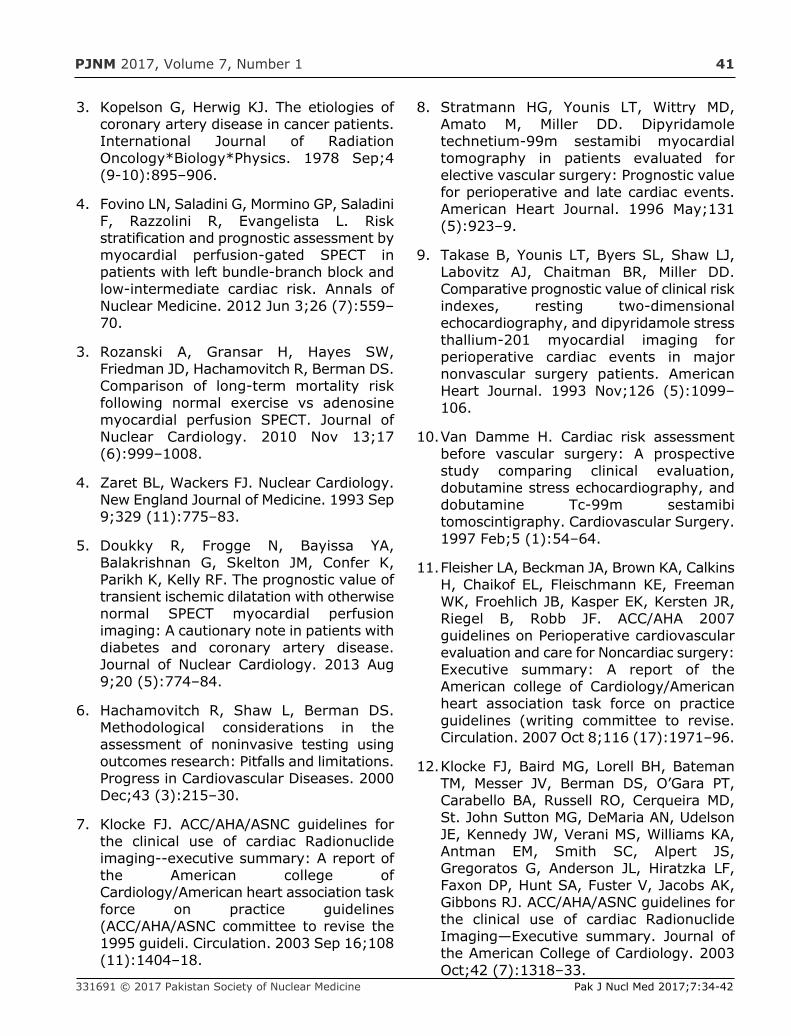
PJNM 2017, Volume 7, Number 1 41
3. Kopelson G, Herwig KJ. The etiologies ofcoronary artery disease in cancer patients.International Journal of RadiationOncology*Biology*Physics. 1978 Sep;4(9-10):895–906.
4. Fovino LN, Saladini G, Mormino GP, SaladiniF, Razzolini R, Evangelista L. Riskstratification and prognostic assessment bymyocardial perfusion-gated SPECT inpatients with left bundle-branch block andlow-intermediate cardiac risk. Annals ofNuclear Medicine. 2012 Jun 3;26 (7):559–70.
3. Rozanski A, Gransar H, Hayes SW,Friedman JD, Hachamovitch R, Berman DS.Comparison of long-term mortality riskfollowing normal exercise vs adenosinemyocardial perfusion SPECT. Journal ofNuclear Cardiology. 2010 Nov 13;17(6):999–1008.
4. Zaret BL, Wackers FJ. Nuclear Cardiology.New England Journal of Medicine. 1993 Sep9;329 (11):775–83.
5. Doukky R, Frogge N, Bayissa YA,Balakrishnan G, Skelton JM, Confer K,Parikh K, Kelly RF. The prognostic value oftransient ischemic dilatation with otherwisenormal SPECT myocardial perfusionimaging: A cautionary note in patients withdiabetes and coronary artery disease.Journal of Nuclear Cardiology. 2013 Aug9;20 (5):774–84.
6. Hachamovitch R, Shaw L, Berman DS.Methodological considerations in theassessment of noninvasive testing usingoutcomes research: Pitfalls and limitations.Progress in Cardiovascular Diseases. 2000Dec;43 (3):215–30.
7. Klocke FJ. ACC/AHA/ASNC guidelines forthe clinical use of cardiac Radionuclideimaging--executive summary: A report ofthe American college ofCardiology/American heart association taskforce on practice guidelines(ACC/AHA/ASNC committee to revise the1995 guideli. Circulation. 2003 Sep 16;108(11):1404–18.
8. Stratmann HG, Younis LT, Wittry MD,Amato M, Miller DD. Dipyridamoletechnetium-99m sestamibi myocardialtomography in patients evaluated forelective vascular surgery: Prognostic valuefor perioperative and late cardiac events.American Heart Journal. 1996 May;131(5):923–9.
9. Takase B, Younis LT, Byers SL, Shaw LJ,Labovitz AJ, Chaitman BR, Miller DD.Comparative prognostic value of clinical riskindexes, resting two-dimensionalechocardiography, and dipyridamole stressthallium-201 myocardial imaging forperioperative cardiac events in majornonvascular surgery patients. AmericanHeart Journal. 1993 Nov;126 (5):1099–106.
10. Van Damme H. Cardiac risk assessmentbefore vascular surgery: A prospectivestudy comparing clinical evaluation,dobutamine stress echocardiography, anddobutamine Tc-99m sestamibitomoscintigraphy. Cardiovascular Surgery.1997 Feb;5 (1):54–64.
11. Fleisher LA, Beckman JA, Brown KA, CalkinsH, Chaikof EL, Fleischmann KE, FreemanWK, Froehlich JB, Kasper EK, Kersten JR,Riegel B, Robb JF. ACC/AHA 2007guidelines on Perioperative cardiovascularevaluation and care for Noncardiac surgery:Executive summary: A report of theAmerican college of Cardiology/Americanheart association task force on practiceguidelines (writing committee to revise.Circulation. 2007 Oct 8;116 (17):1971–96.
12. Klocke FJ, Baird MG, Lorell BH, BatemanTM, Messer JV, Berman DS, O’Gara PT,Carabello BA, Russell RO, Cerqueira MD,St. John Sutton MG, DeMaria AN, UdelsonJE, Kennedy JW, Verani MS, Williams KA,Antman EM, Smith SC, Alpert JS,Gregoratos G, Anderson JL, Hiratzka LF,Faxon DP, Hunt SA, Fuster V, Jacobs AK,Gibbons RJ. ACC/AHA/ASNC guidelines forthe clinical use of cardiac RadionuclideImaging—Executive summary. Journal ofthe American College of Cardiology. 2003Oct;42 (7):1318–33.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:34-42
PJNM 2017, Volume 7, Number 1 42
13. Kopelson G, Herwig KJ. The etiologies ofcoronary artery disease in cancer patients.International Journal of RadiationOncology*Biology*Physics. 1978 Sep;4 (9-10):895–906.
14. Fleisher LA, Beckman JA, Brown KA, CalkinsH, Chaikof EL, Fleischmann KE, FreemanWK, Froehlich JB, Kasper EK, Kersten JR,Riegel B, Robb JF. ACC/AHA 2007 guidelineson Perioperative cardiovascular evaluationand care for Noncardiac surgery: Executivesummary: A report of the American collegeof Cardiology/American heart associationtask force on practice guidelines (writingcommittee to revise. Circulation. 2007 Oct8;116 (17):1971–96.
15. Klocke FJ, Baird MG, Lorell BH, Bateman TM,Messer JV, Berman DS, O’Gara PT,Carabello BA, Russell RO, Cerqueira MD, St.John Sutton MG, DeMaria AN, Udelson JE,Kennedy JW, Verani MS, Williams KA,Antman EM, Smith SC, Alpert JS,Gregoratos G, Anderson JL, Hiratzka LF,Faxon DP, Hunt SA, Fuster V, Jacobs AK,Gibbons RJ. ACC/AHA/ASNC guidelines forthe clinical use of cardiac RadionuclideImaging—Executive summary. Journal ofthe American College of Cardiology. 2003Oct;42 (7):1318–33.
16. Zellweger M. Risk stratification in patientswith remote prior myocardial infarctionusing rest-stress myocardial perfusionSPECT: Prognostic value and impact onreferral to early catheterization. Journal ofNuclear Cardiology. 2002 Jan;9 (1):23–32.
17. Bai J, Hashimoto J, Nakahara T, Suzuki T,Kubo A. Influence of ageing on perioperativecardiac risk in non-cardiac surgery}{Ageingand perioperative cardiac risk. Age andAgeing. 2006 Nov 17;36 (1):68–72.
18. Mangano DT, London MJ, Tubau JF, BrownerWS, Hollenberg M, Krupski W, Layug EL,Massie B. Dipyridamole thallium-201scintigraphy as a preoperative screeningtest. A reexamination of its predictivepotential. Study of Perioperative Ischemiaresearch group. Circulation. 1991 Aug 1;84
(2):493–502.
19. Mangano DT. Adverse outcomes aftersurgery in the year 2001-A continuingodyssey. Anesthesiology. 1998 Mar;88(3):561–4.
20. Younis L, Stratmann H, Takase B, Byers S,Chaitman BR, Miller DD. Preoperativeclinical assessment and Dipyridamolethallium-201 Scintigraphy for prediction andprevention of cardiac events in patientshaving Major Noncardiovascular surgeryand known or suspected coronary arterydisease. Survey of Anesthesiology1995;39(3):167-168.
21. Marwick TH, Underwood DA. Dipyridamolethallium imaging may not be a reliablescreening test for coronary artery diseasein patients undergoing vascular surgery.Clinical Cardiology. 1990 Jan;13(1):14–8.
22. Lee TH, Marcantonio ER, Mangione CM,Thomas EJ, Polanczyk CA, Cook EF,Sugarbaker DJ, Donaldson MC, Poss R, HoKKL, Ludwig LE, Pedan A, Goldman L.Derivation and prospective validation of asimple index for prediction of cardiac risk ofMajor Noncardiac surgery. Circulation. 1999Sep 7;100(10):1043–9.
23. Kertai MD. A meta-analysis comparing theprognostic accuracy of six diagnostic testsfor predicting perioperative cardiac risk inpatients undergoing major vascularsurgery. Heart. 2003 Nov 1;89(11):1327–34.
24. Etchells E, Meade M, Tomlinson G, Cook D.Semiquantitative dipyridamole myocardialstress perfusion imaging for cardiac riskassessment before noncardiac vascularsurgery: A metaanalysis. Journal ofVascular Surgery. 2002 Sep;36(3):534–40.
25. Stratmann HG, Younis LT, Wittry MD, AmatoM, Miller DD. Dipyridamole technetium-99msestamibi myocardial tomography inpatients evaluated for elective vascularsurgery: Prognostic value for perioperativeand late cardiac events. American HeartJournal. 1996 May;131(5):923–9.
Pak J Nucl Med 2017;7:34-42 2305-1630(201701/01)7:1<33:PCRSNC>2.0.TX;2-M
PJNM 2017; 7:43-47 331691 © 2017 Pakistan Society of Nuclear Medicine
Clinical characteristics and long-term outcome ofpatients with differentiated carcinoma of thyroid
with bone metastases: a retrospective study
Sadaf Tufail Butt*, Shazia Fatima, Noreen Marwat,Kahkashan Mir, Ayesha Ammar, Mohammad Faheem
Nuclear Medicine, Oncology and Radiotherapy Institute (NORI), Islamabad
ORIGINAL ARTICLE
Abstract
Aims Bone is the second most frequent targetof distant metastases in patients withdifferentiated thyroid cancer (DTC). However,there is a controversy regarding the long-termoutcome of the breast cancer patients wtih bonemetastases. This study therefore was designedwith the objective of assessing the clinicalcharacteristics related to the long-termoutcome and prognosis of patients with bonemetastases.
Methods We reviewed the medical records of360 patients of differentiated thyroid cancerfollowed at our institute from 2007 to 2012. Atotal of 57 patients were found to have bonemetastases, who we analyzed with regard totheir basic demographic data, clinicalcharacteristics, treatment and clinical outcomes.
Results The incidence of bone metastases fromthyroid carcinoma was 15.8%. The mean ageat the diagnosis of bone metastases was 47±18years (range 16 to 80 years); 46% patients
were below 40 years of age and 53.8% of thepatients were above 40 years of age. 15.3%were males and 84.6% were females.Histopathologic subtypes included papillary(38%), and follicular (45.6%). Multiple bonesites were involved in 50% of the patients with29% of the patients with single bone siteinvolvement; and 20.8% of the patients hadmetastases to other body organs. All patientsunderwent near-total thyroidectomy followedby aggressive radioiodine therapy. Number of131I doses received ranged from 3 to 12 with amean of 6.6. Mean dose of 131I per patient was48914 MBq ± 20424 (Range: 18130 - 76960).Baseline thyroglobulin (TG) level ranged from380ng/ml to 17300ng/ml with a mean value of2250±5644 ng/ml. 60% of the patients showeda declining trend in TG over time, whilst 23%of the patients showed a rising trend; 6.2% ofthe patients had normal TG/ATG(antithyroglobulin) values throughout thecourse of disease. 10.4% of the patients hadstatic TG levels. 64% of the patients with bonemetastases showed 5-year survival.
Conclusion Multiple bone metastases representa frequent complication of DTC especially offollicular thyroid cancer. In our population it ismore common in females and in patients above40 years of age. Overall survival rate is verygood in the patients with bone metastasis ifthey are managed aggressively with totalthyroidectomy and repeated radioactive iodine.
*Correspondence
Sadaf Tufail Butt Nuclear Medicine Oncology & Radiotherapy Institute (NORI) Hanna road, G-8/3, Islamabad, Pakistan Tel: +923005270408
www.pjnm.net 2305-1630(201701/01)7:1<43:CCLTPO>2.0.TX;2-M
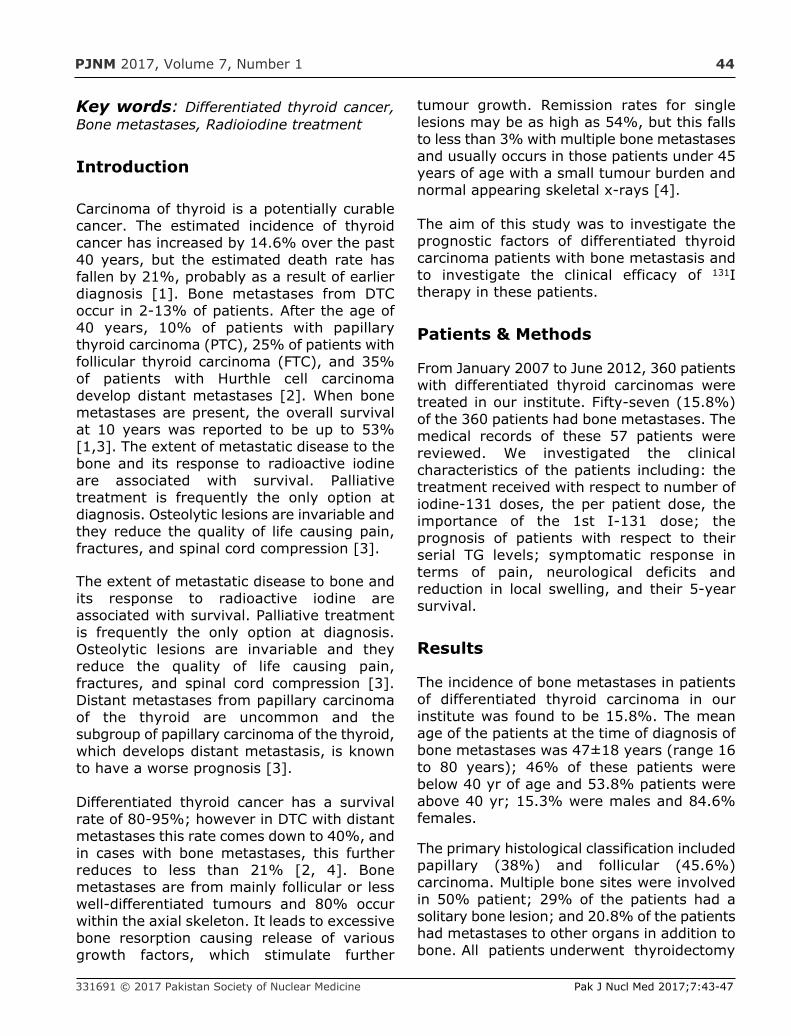
PJNM 2017, Volume 7, Number 1 44
Key words: Differentiated thyroid cancer,Bone metastases, Radioiodine treatment
Introduction
Carcinoma of thyroid is a potentially curablecancer. The estimated incidence of thyroidcancer has increased by 14.6% over the past40 years, but the estimated death rate hasfallen by 21%, probably as a result of earlierdiagnosis [1]. Bone metastases from DTCoccur in 2-13% of patients. After the age of40 years, 10% of patients with papillarythyroid carcinoma (PTC), 25% of patients withfollicular thyroid carcinoma (FTC), and 35%of patients with Hurthle cell carcinomadevelop distant metastases [2]. When bonemetastases are present, the overall survivalat 10 years was reported to be up to 53%[1,3]. The extent of metastatic disease to thebone and its response to radioactive iodineare associated with survival. Palliativetreatment is frequently the only option atdiagnosis. Osteolytic lesions are invariable andthey reduce the quality of life causing pain,fractures, and spinal cord compression [3].
The extent of metastatic disease to bone andits response to radioactive iodine areassociated with survival. Palliative treatmentis frequently the only option at diagnosis.Osteolytic lesions are invariable and theyreduce the quality of life causing pain,fractures, and spinal cord compression [3].Distant metastases from papillary carcinomaof the thyroid are uncommon and thesubgroup of papillary carcinoma of the thyroid,which develops distant metastasis, is knownto have a worse prognosis [3].
Differentiated thyroid cancer has a survivalrate of 80-95%; however in DTC with distantmetastases this rate comes down to 40%, andin cases with bone metastases, this furtherreduces to less than 21% [2, 4]. Bonemetastases are from mainly follicular or lesswell-differentiated tumours and 80% occurwithin the axial skeleton. It leads to excessivebone resorption causing release of variousgrowth factors, which stimulate further
tumour growth. Remission rates for singlelesions may be as high as 54%, but this fallsto less than 3% with multiple bone metastasesand usually occurs in those patients under 45years of age with a small tumour burden andnormal appearing skeletal x-rays [4].
The aim of this study was to investigate theprognostic factors of differentiated thyroidcarcinoma patients with bone metastasis andto investigate the clinical efficacy of 131Itherapy in these patients.
Patients & Methods
From January 2007 to June 2012, 360 patientswith differentiated thyroid carcinomas weretreated in our institute. Fifty-seven (15.8%)of the 360 patients had bone metastases. Themedical records of these 57 patients werereviewed. We investigated the clinicalcharacteristics of the patients including: thetreatment received with respect to number ofiodine-131 doses, the per patient dose, theimportance of the 1st I-131 dose; theprognosis of patients with respect to theirserial TG levels; symptomatic response interms of pain, neurological deficits andreduction in local swelling, and their 5-yearsurvival.
Results
The incidence of bone metastases in patientsof differentiated thyroid carcinoma in ourinstitute was found to be 15.8%. The meanage of the patients at the time of diagnosis ofbone metastases was 47±18 years (range 16to 80 years); 46% of these patients werebelow 40 yr of age and 53.8% patients wereabove 40 yr; 15.3% were males and 84.6%females.
The primary histological classification includedpapillary (38%) and follicular (45.6%)carcinoma. Multiple bone sites were involvedin 50% patient; 29% of the patients had asolitary bone lesion; and 20.8% of the patientshad metastases to other organs in addition tobone. All patients underwent thyroidectomy
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:43-47
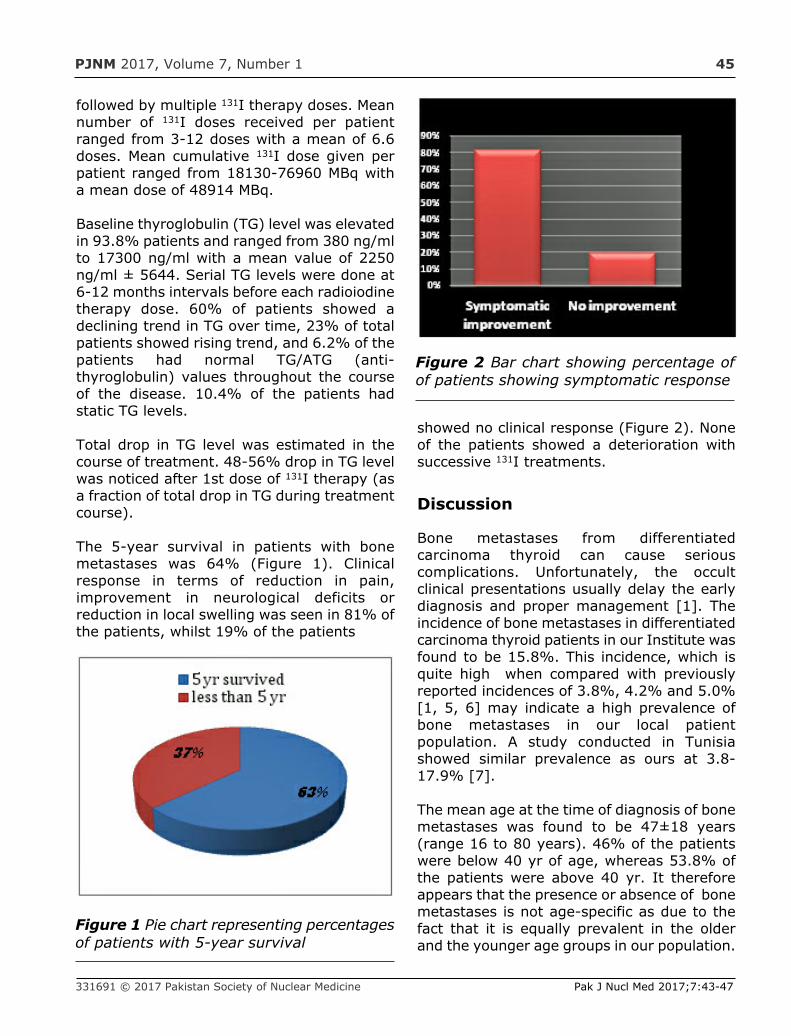
PJNM 2017, Volume 7, Number 1 45
followed by multiple 131I therapy doses. Meannumber of 131I doses received per patientranged from 3-12 doses with a mean of 6.6doses. Mean cumulative 131I dose given perpatient ranged from 18130-76960 MBq witha mean dose of 48914 MBq.
Baseline thyroglobulin (TG) level was elevatedin 93.8% patients and ranged from 380 ng/mlto 17300 ng/ml with a mean value of 2250ng/ml ± 5644. Serial TG levels were done at6-12 months intervals before each radioiodinetherapy dose. 60% of patients showed adeclining trend in TG over time, 23% of totalpatients showed rising trend, and 6.2% of thepatients had normal TG/ATG (anti-thyroglobulin) values throughout the courseof the disease. 10.4% of the patients hadstatic TG levels.
Total drop in TG level was estimated in thecourse of treatment. 48-56% drop in TG levelwas noticed after 1st dose of 131I therapy (asa fraction of total drop in TG during treatmentcourse).
The 5-year survival in patients with bonemetastases was 64% (Figure 1). Clinicalresponse in terms of reduction in pain,improvement in neurological deficits orreduction in local swelling was seen in 81% ofthe patients, whilst 19% of the patients
showed no clinical response (Figure 2). Noneof the patients showed a deterioration withsuccessive 131I treatments.
Discussion
Bone metastases from differentiatedcarcinoma thyroid can cause seriouscomplications. Unfortunately, the occultclinical presentations usually delay the earlydiagnosis and proper management [1]. Theincidence of bone metastases in differentiatedcarcinoma thyroid patients in our Institute wasfound to be 15.8%. This incidence, which isquite high when compared with previouslyreported incidences of 3.8%, 4.2% and 5.0%[1, 5, 6] may indicate a high prevalence ofbone metastases in our local patientpopulation. A study conducted in Tunisiashowed similar prevalence as ours at 3.8-17.9% [7].
The mean age at the time of diagnosis of bonemetastases was found to be 47±18 years(range 16 to 80 years). 46% of the patientswere below 40 yr of age, whereas 53.8% ofthe patients were above 40 yr. It thereforeappears that the presence or absence of bonemetastases is not age-specific as due to thefact that it is equally prevalent in the olderand the younger age groups in our population.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:43-47
Figure 1 Pie chart representing percentagesof patients with 5-year survival
Figure 2 Bar chart showing percentage ofof patients showing symptomatic response
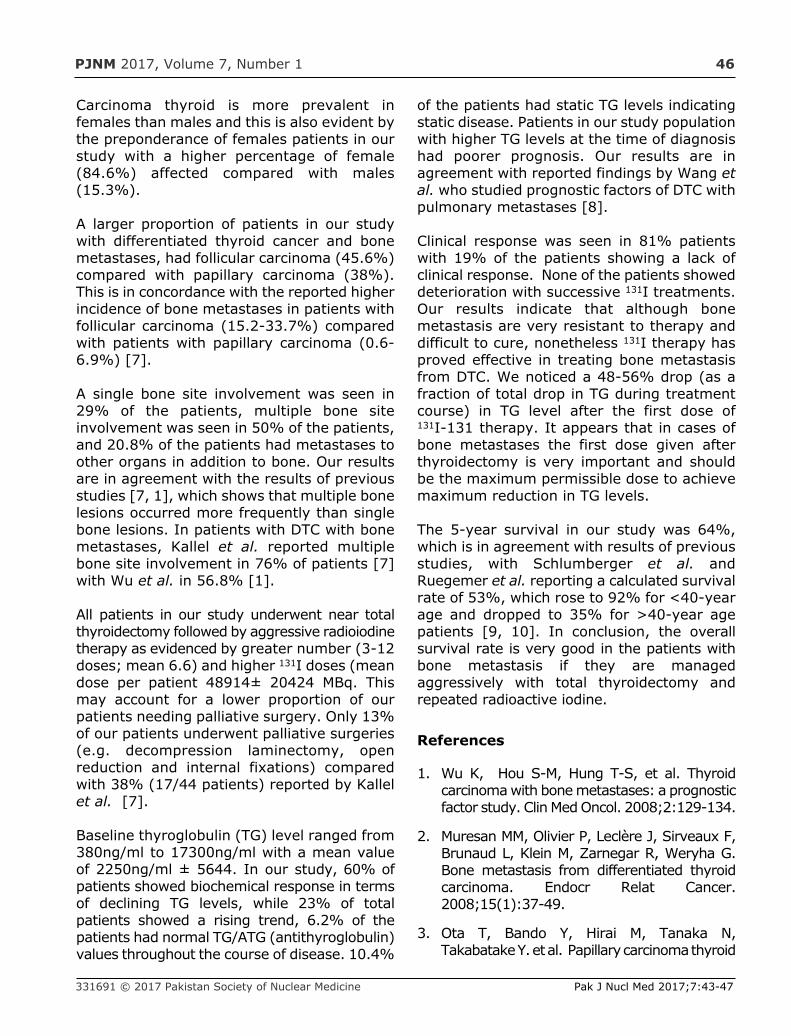
PJNM 2017, Volume 7, Number 1 46
Carcinoma thyroid is more prevalent infemales than males and this is also evident bythe preponderance of females patients in ourstudy with a higher percentage of female(84.6%) affected compared with males(15.3%).
A larger proportion of patients in our studywith differentiated thyroid cancer and bonemetastases, had follicular carcinoma (45.6%)compared with papillary carcinoma (38%).This is in concordance with the reported higherincidence of bone metastases in patients withfollicular carcinoma (15.2-33.7%) comparedwith patients with papillary carcinoma (0.6-6.9%) [7].
A single bone site involvement was seen in29% of the patients, multiple bone siteinvolvement was seen in 50% of the patients,and 20.8% of the patients had metastases toother organs in addition to bone. Our resultsare in agreement with the results of previousstudies [7, 1], which shows that multiple bonelesions occurred more frequently than singlebone lesions. In patients with DTC with bonemetastases, Kallel et al. reported multiplebone site involvement in 76% of patients [7]with Wu et al. in 56.8% [1].
All patients in our study underwent near totalthyroidectomy followed by aggressive radioiodinetherapy as evidenced by greater number (3-12doses; mean 6.6) and higher 131I doses (meandose per patient 48914± 20424 MBq. Thismay account for a lower proportion of ourpatients needing palliative surgery. Only 13%of our patients underwent palliative surgeries(e.g. decompression laminectomy, openreduction and internal fixations) comparedwith 38% (17/44 patients) reported by Kallelet al. [7].
Baseline thyroglobulin (TG) level ranged from380ng/ml to 17300ng/ml with a mean valueof 2250ng/ml ± 5644. In our study, 60% ofpatients showed biochemical response in termsof declining TG levels, while 23% of totalpatients showed a rising trend, 6.2% of thepatients had normal TG/ATG (antithyroglobulin)values throughout the course of disease. 10.4%
of the patients had static TG levels indicatingstatic disease. Patients in our study populationwith higher TG levels at the time of diagnosishad poorer prognosis. Our results are inagreement with reported findings by Wang etal. who studied prognostic factors of DTC withpulmonary metastases [8].
Clinical response was seen in 81% patientswith 19% of the patients showing a lack ofclinical response. None of the patients showeddeterioration with successive 131I treatments.Our results indicate that although bonemetastasis are very resistant to therapy anddifficult to cure, nonetheless 131I therapy hasproved effective in treating bone metastasisfrom DTC. We noticed a 48-56% drop (as afraction of total drop in TG during treatmentcourse) in TG level after the first dose of131I-131 therapy. It appears that in cases ofbone metastases the first dose given afterthyroidectomy is very important and shouldbe the maximum permissible dose to achievemaximum reduction in TG levels.
The 5-year survival in our study was 64%,which is in agreement with results of previousstudies, with Schlumberger et al. andRuegemer et al. reporting a calculated survivalrate of 53%, which rose to 92% for <40-yearage and dropped to 35% for >40-year agepatients [9, 10]. In conclusion, the overallsurvival rate is very good in the patients withbone metastasis if they are managedaggressively with total thyroidectomy andrepeated radioactive iodine.
References
1. Wu K, Hou S-M, Hung T-S, et al. Thyroidcarcinoma with bone metastases: a prognosticfactor study. Clin Med Oncol. 2008;2:129-134.
2. Muresan MM, Olivier P, Leclère J, Sirveaux F,Brunaud L, Klein M, Zarnegar R, Weryha G.Bone metastasis from differentiated thyroidcarcinoma. Endocr Relat Cancer.2008;15(1):37-49.
3. Ota T, Bando Y, Hirai M, Tanaka N,Takabatake Y. et al. Papillary carcinoma thyroid
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:43-47
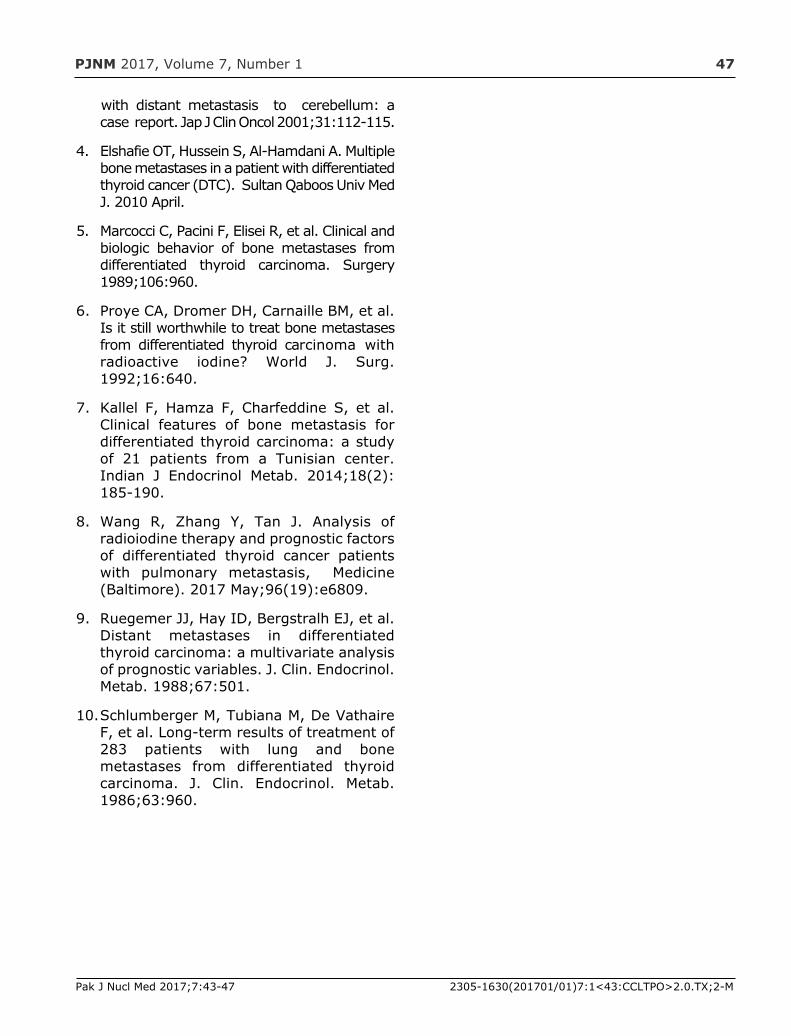
PJNM 2017, Volume 7, Number 1 47
with distant metastasis to cerebellum: acase report. Jap J Clin Oncol 2001;31:112-115.
4. Elshafie OT, Hussein S, Al-Hamdani A. Multiplebone metastases in a patient with differentiatedthyroid cancer (DTC). Sultan Qaboos Univ MedJ. 2010 April.
5. Marcocci C, Pacini F, Elisei R, et al. Clinical andbiologic behavior of bone metastases fromdifferentiated thyroid carcinoma. Surgery1989;106:960.
6. Proye CA, Dromer DH, Carnaille BM, et al.Is it still worthwhile to treat bone metastasesfrom differentiated thyroid carcinoma withradioactive iodine? World J. Surg.1992;16:640.
7. Kallel F, Hamza F, Charfeddine S, et al.Clinical features of bone metastasis fordifferentiated thyroid carcinoma: a studyof 21 patients from a Tunisian center.Indian J Endocrinol Metab. 2014;18(2):185-190.
8. Wang R, Zhang Y, Tan J. Analysis ofradioiodine therapy and prognostic factorsof differentiated thyroid cancer patientswith pulmonary metastasis, Medicine(Baltimore). 2017 May;96(19):e6809.
9. Ruegemer JJ, Hay ID, Bergstralh EJ, et al.Distant metastases in differentiatedthyroid carcinoma: a multivariate analysisof prognostic variables. J. Clin. Endocrinol.Metab. 1988;67:501.
10. Schlumberger M, Tubiana M, De VathaireF, et al. Long-term results of treatment of283 patients with lung and bonemetastases from differentiated thyroidcarcinoma. J. Clin. Endocrinol. Metab.1986;63:960.
Pak J Nucl Med 2017;7:43-47 2305-1630(201701/01)7:1<43:CCLTPO>2.0.TX;2-M

PJNM 2017, 7:48-52 331691 © 2017 Pakistan Society of Nuclear Medicine
Successful Ra-223 treatment with a longinterval between the second and the third
cycles: a case report
Tatiana Kochetova*, Valeriy Krylov
Nuclear Therapy Department,A Tsyb Medical Radiological Research Center,National Medical Research Radiological CenterMinistry of Health of the Russian Federation
CASE REPORT
Abstract
Ra-223 therapy is recommended for CastrationResistant Prostate Cancer (CRPC) patients withbone metastases. The standard protocol is 5-6cycles of therapy with 4 weeks intervals to gainsurvival benefit.
We report a case of a chemo-naïve CRPC patientwho after 1.5 years of androgen-deprivationtherapy had widespread bone metastases, PSAof 4186 ng/ml, alkaline phosphatase (ALP) at2982 U/l, bone marrow involvement with anaemiaand thrombocytopaenia. 223RaCl2 therapy wasstarted in August 2014. After the first two cyclesof 223RaCl2 PSA dropped to 70 ng/ml, ALP to 877U/l. The third cycle was delayed for 5.5 monthsdue to technical reasons. Unexpectedly, duringRa-223 therapy interruption the positive changes
were still ongoing. PSA-level decreasedfurther, to 0.28 ng/l and ALP to 254 U/l. Hblevel increased from 101 to 125 g/l, PLT from105 to 180x109/l. After the interruption thepatient received 4 planned cycles. Control bonescan after the 4th cycle revealed pathologicaluptake only in shoulder joints and sternum. Inthe follow-up period the patient demonstratedminimal disease signs: with normal ALP level,PSA 0.11 ng/ml.
Ra-223 Therapy can give anti-tumour effect,as can be seen from the significant decreasein the PSA level. Breaks in Ra-223 Therapy arenot dramatic. After interruption, it can becontinued again. This fact can be taken intoaccount while planning therapy. As shownhere, clinical cases such the one we havereported, may allow a degree of flexibility tothe standard recommendations on a case tocase basis.
Key words: Radium-223, Castrationresistant prostate cancer, Bone metastases
Introduction
Ra-223 chloride became a gold standard oftreatment of Castration Resistant Prostate Cancer
www.pjnm.net 2305-1630(201701/01)7:1<48:SRTWLI>2.0.TX;2-M
*Correspondence
Tatiana Kochetova249034 Koroleva 4Obninsk, Kaluga region,Russian FederationTel: +7 (919) 0345838,Fax: +7 (484) 3993344Email: [email protected]
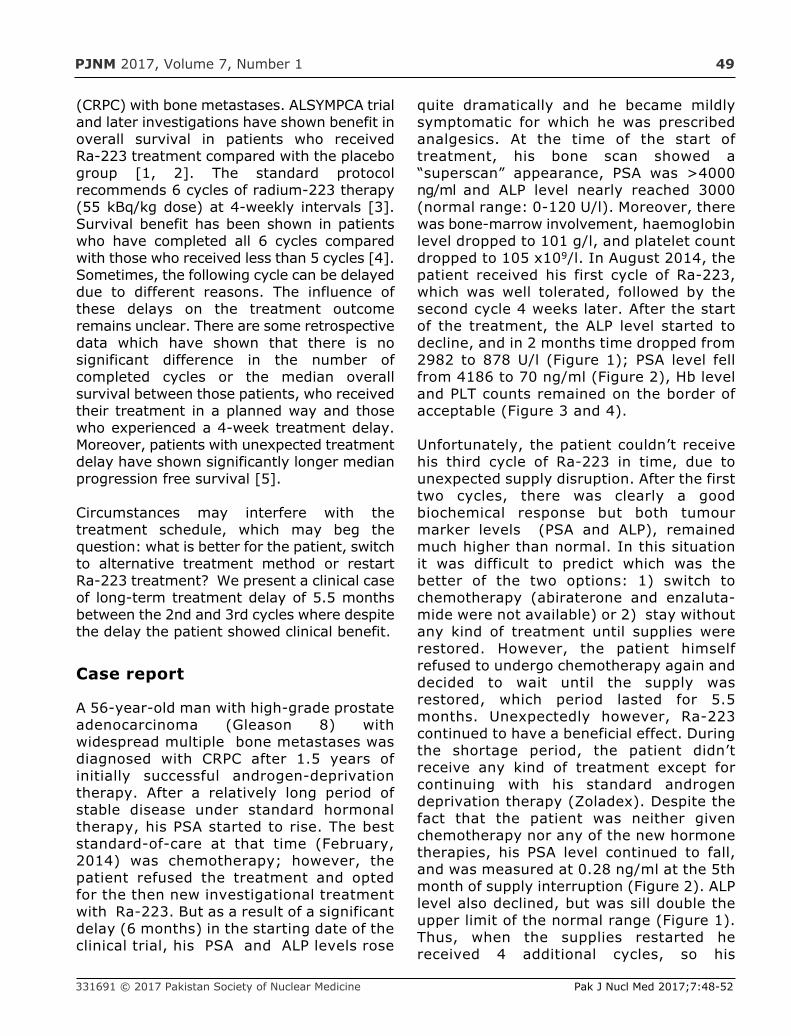
PJNM 2017, Volume 7, Number 1 49
(CRPC) with bone metastases. ALSYMPCA trialand later investigations have shown benefit inoverall survival in patients who receivedRa-223 treatment compared with the placebogroup [1, 2]. The standard protocolrecommends 6 cycles of radium-223 therapy(55 kBq/kg dose) at 4-weekly intervals [3].Survival benefit has been shown in patientswho have completed all 6 cycles comparedwith those who received less than 5 cycles [4].Sometimes, the following cycle can be delayeddue to different reasons. The influence ofthese delays on the treatment outcomeremains unclear. There are some retrospectivedata which have shown that there is nosignificant difference in the number ofcompleted cycles or the median overallsurvival between those patients, who receivedtheir treatment in a planned way and thosewho experienced a 4-week treatment delay.Moreover, patients with unexpected treatmentdelay have shown significantly longer medianprogression free survival [5].
Circumstances may interfere with thetreatment schedule, which may beg thequestion: what is better for the patient, switchto alternative treatment method or restartRa-223 treatment? We present a clinical caseof long-term treatment delay of 5.5 monthsbetween the 2nd and 3rd cycles where despitethe delay the patient showed clinical benefit.
Case report
A 56-year-old man with high-grade prostateadenocarcinoma (Gleason 8) withwidespread multiple bone metastases wasdiagnosed with CRPC after 1.5 years ofinitially successful androgen-deprivationtherapy. After a relatively long period ofstable disease under standard hormonaltherapy, his PSA started to rise. The beststandard-of-care at that time (February,2014) was chemotherapy; however, thepatient refused the treatment and optedfor the then new investigational treatmentwith Ra-223. But as a result of a significantdelay (6 months) in the starting date of theclinical trial, his PSA and ALP levels rose
quite dramatically and he became mildlysymptomatic for which he was prescribedanalgesics. At the time of the start oftreatment, his bone scan showed a“superscan” appearance, PSA was >4000ng/ml and ALP level nearly reached 3000(normal range: 0-120 U/l). Moreover, therewas bone-marrow involvement, haemoglobinlevel dropped to 101 g/l, and platelet countdropped to 105 x109/l. In August 2014, thepatient received his first cycle of Ra-223,which was well tolerated, followed by thesecond cycle 4 weeks later. After the startof the treatment, the ALP level started todecline, and in 2 months time dropped from2982 to 878 U/l (Figure 1); PSA level fellfrom 4186 to 70 ng/ml (Figure 2), Hb leveland PLT counts remained on the border ofacceptable (Figure 3 and 4).
Unfortunately, the patient couldn’t receivehis third cycle of Ra-223 in time, due tounexpected supply disruption. After the firsttwo cycles, there was clearly a goodbiochemical response but both tumourmarker levels (PSA and ALP), remainedmuch higher than normal. In this situationit was difficult to predict which was thebetter of the two options: 1) switch tochemotherapy (abiraterone and enzaluta-mide were not available) or 2) stay withoutany kind of treatment until supplies wererestored. However, the patient himselfrefused to undergo chemotherapy again anddecided to wait until the supply wasrestored, which period lasted for 5.5months. Unexpectedly however, Ra-223continued to have a beneficial effect. Duringthe shortage period, the patient didn’treceive any kind of treatment except forcontinuing with his standard androgendeprivation therapy (Zoladex). Despite thefact that the patient was neither givenchemotherapy nor any of the new hormonetherapies, his PSA level continued to fall,and was measured at 0.28 ng/ml at the 5thmonth of supply interruption (Figure 2). ALPlevel also declined, but was sill double theupper limit of the normal range (Figure 1).Thus, when the supplies restarted hereceived 4 additional cycles, so his
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:48-52
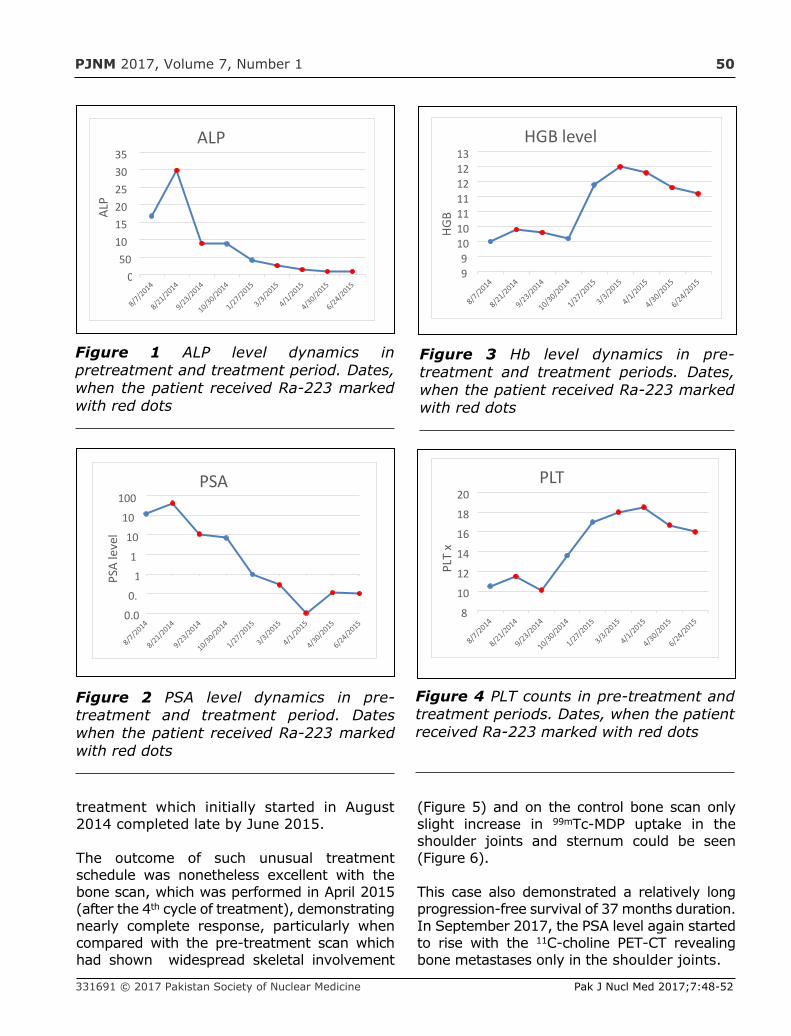
PJNM 2017, Volume 7, Number 1 50
treatment which initially started in August2014 completed late by June 2015.
The outcome of such unusual treatmentschedule was nonetheless excellent with thebone scan, which was performed in April 2015(after the 4th cycle of treatment), demonstratingnearly complete response, particularly whencompared with the pre-treatment scan whichhad shown widespread skeletal involvement
(Figure 5) and on the control bone scan onlyslight increase in 99mTc-MDP uptake in theshoulder joints and sternum could be seen(Figure 6).
This case also demonstrated a relatively longprogression-free survival of 37 months duration.In September 2017, the PSA level again startedto rise with the 11C-choline PET-CT revealingbone metastases only in the shoulder joints.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:48-52
Figure 1 ALP level dynamics inpretreatment and treatment period. Dates,when the patient received Ra-223 markedwith red dots
050
101520253035
ALP
ALP
0.0
0.
1
1
10
10
100
PSA
leve
l
PSA
Figure 2 PSA level dynamics in pre-treatment and treatment period. Dateswhen the patient received Ra-223 markedwith red dots
Figure 3 Hb level dynamics in pre-treatment and treatment periods. Dates,when the patient received Ra-223 markedwith red dots
Figure 4 PLT counts in pre-treatment andtreatment periods. Dates, when the patientreceived Ra-223 marked with red dots
99
10101111121213
HGB
HGB level
8
10
12
14
16
18
20
PLT
x
PLT
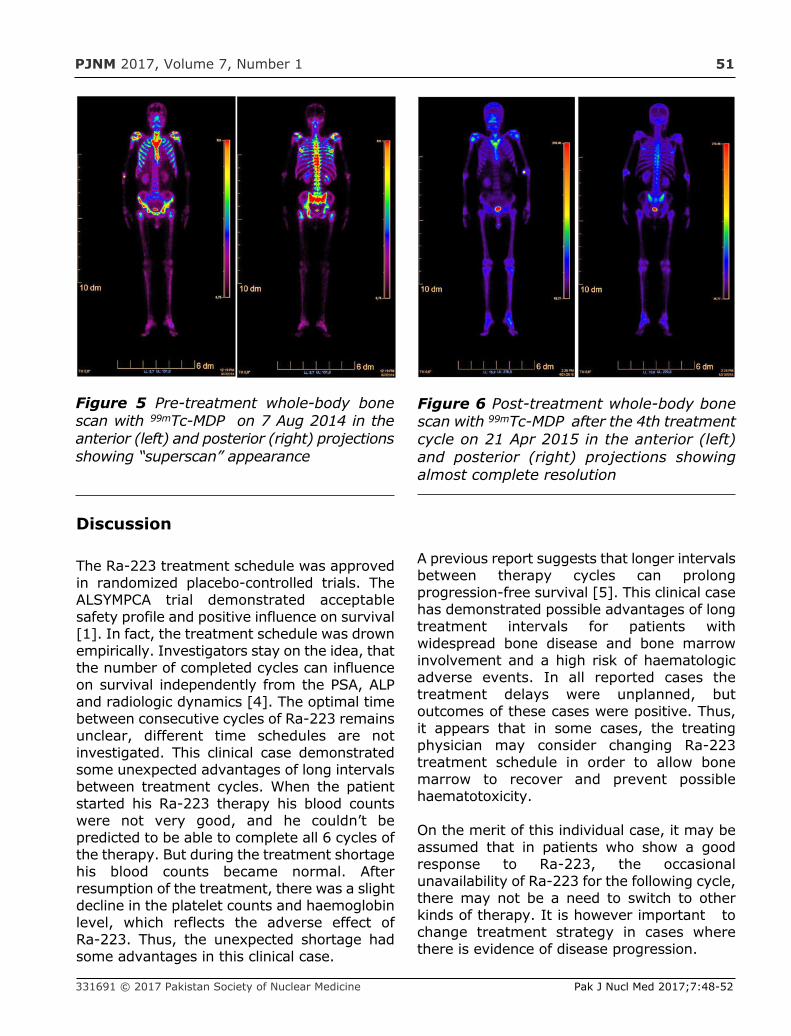
PJNM 2017, Volume 7, Number 1 51
Discussion
The Ra-223 treatment schedule was approvedin randomized placebo-controlled trials. TheALSYMPCA trial demonstrated acceptablesafety profile and positive influence on survival[1]. In fact, the treatment schedule was drownempirically. Investigators stay on the idea, thatthe number of completed cycles can influenceon survival independently from the PSA, ALPand radiologic dynamics [4]. The optimal timebetween consecutive cycles of Ra-223 remainsunclear, different time schedules are notinvestigated. This clinical case demonstratedsome unexpected advantages of long intervalsbetween treatment cycles. When the patientstarted his Ra-223 therapy his blood countswere not very good, and he couldn’t bepredicted to be able to complete all 6 cycles ofthe therapy. But during the treatment shortagehis blood counts became normal. Afterresumption of the treatment, there was a slightdecline in the platelet counts and haemoglobinlevel, which reflects the adverse effect ofRa-223. Thus, the unexpected shortage hadsome advantages in this clinical case.
A previous report suggests that longer intervalsbetween therapy cycles can prolongprogression-free survival [5]. This clinical casehas demonstrated possible advantages of longtreatment intervals for patients withwidespread bone disease and bone marrowinvolvement and a high risk of haematologicadverse events. In all reported cases thetreatment delays were unplanned, butoutcomes of these cases were positive. Thus,it appears that in some cases, the treatingphysician may consider changing Ra-223treatment schedule in order to allow bonemarrow to recover and prevent possiblehaematotoxicity.
On the merit of this individual case, it may beassumed that in patients who show a goodresponse to Ra-223, the occasionalunavailability of Ra-223 for the following cycle,there may not be a need to switch to otherkinds of therapy. It is however important tochange treatment strategy in cases wherethere is evidence of disease progression.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:48-52
Figure 5 Pre-treatment whole-body bonescan with 99mTc-MDP on 7 Aug 2014 in theanterior (left) and posterior (right) projectionsshowing “superscan” appearance
Figure 6 Post-treatment whole-body bonescan with 99mTc-MDP after the 4th treatmentcycle on 21 Apr 2015 in the anterior (left)and posterior (right) projections showingalmost complete resolution
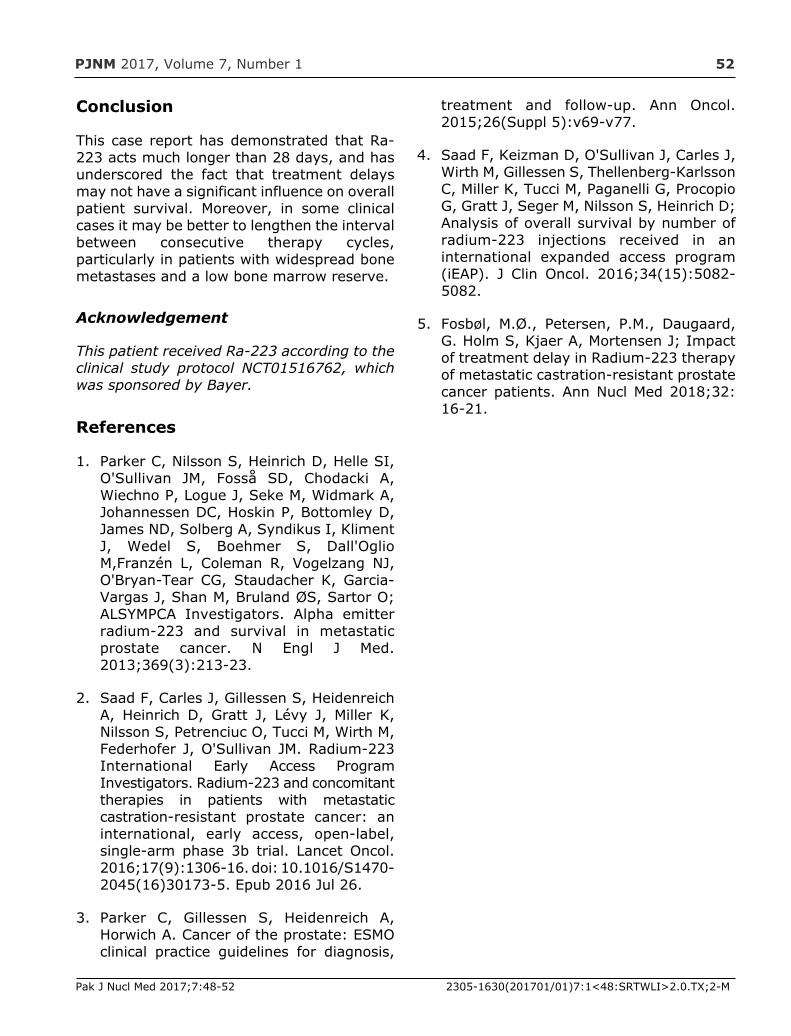
PJNM 2017, Volume 7, Number 1 52
Conclusion
This case report has demonstrated that Ra-223 acts much longer than 28 days, and hasunderscored the fact that treatment delaysmay not have a significant influence on overallpatient survival. Moreover, in some clinicalcases it may be better to lengthen the intervalbetween consecutive therapy cycles,particularly in patients with widespread bonemetastases and a low bone marrow reserve.
Acknowledgement
This patient received Ra-223 according to theclinical study protocol NCT01516762, whichwas sponsored by Bayer.
References
1. Parker C, Nilsson S, Heinrich D, Helle SI,O'Sullivan JM, Fosså SD, Chodacki A,Wiechno P, Logue J, Seke M, Widmark A,Johannessen DC, Hoskin P, Bottomley D,James ND, Solberg A, Syndikus I, KlimentJ, Wedel S, Boehmer S, Dall'OglioM,Franzén L, Coleman R, Vogelzang NJ,O'Bryan-Tear CG, Staudacher K, Garcia-Vargas J, Shan M, Bruland ØS, Sartor O;ALSYMPCA Investigators. Alpha emitterradium-223 and survival in metastaticprostate cancer. N Engl J Med.2013;369(3):213-23.
2. Saad F, Carles J, Gillessen S, HeidenreichA, Heinrich D, Gratt J, Lévy J, Miller K,Nilsson S, Petrenciuc O, Tucci M, Wirth M,Federhofer J, O'Sullivan JM. Radium-223International Early Access ProgramInvestigators. Radium-223 and concomitanttherapies in patients with metastaticcastration-resistant prostate cancer: aninternational, early access, open-label,single-arm phase 3b trial. Lancet Oncol.2016;17(9):1306-16. doi: 10.1016/S1470-2045(16)30173-5. Epub 2016 Jul 26.
3. Parker C, Gillessen S, Heidenreich A,Horwich A. Cancer of the prostate: ESMOclinical practice guidelines for diagnosis,
treatment and follow-up. Ann Oncol.2015;26(Suppl 5):v69-v77.
4. Saad F, Keizman D, O'Sullivan J, Carles J,Wirth M, Gillessen S, Thellenberg-KarlssonC, Miller K, Tucci M, Paganelli G, ProcopioG, Gratt J, Seger M, Nilsson S, Heinrich D;Analysis of overall survival by number ofradium-223 injections received in aninternational expanded access program(iEAP). J Clin Oncol. 2016;34(15):5082-5082.
5. Fosbøl, M.Ø., Petersen, P.M., Daugaard,G. Holm S, Kjaer A, Mortensen J; Impactof treatment delay in Radium-223 therapyof metastatic castration-resistant prostatecancer patients. Ann Nucl Med 2018;32:16-21.
Pak J Nucl Med 2017;7:48-52 2305-1630(201701/01)7:1<48:SRTWLI>2.0.TX;2-M

PJNM 2017, 7:53-55 331691 © 2017 Pakistan Society of Nuclear Medicine
Cutaneous flow pattern of primarylymphoedema
Qaisar Hussain Siraj
Department of Nuclear Medicine,Farwania Hospital Kuwait
CASE REPORT
Abstract
A case of a patient with primary lymphoedemawhere the scan pattern could have easily beenconfused with that of secondary lymphoedemais presented. This image pattern thoughoccasionally seen has not previously beenreported.
Key words: Lymphoscintigraphy, 99mTc-Nanocolloid, Primary lymphoedema
Introduction
Qualitative lymphoscintigraphic imageevaluation and interpretation yields specificimage patterns associated with primarylymphoedema (e.g. aplasia or hypoplasia)or secondary lymphoedema (e.g. postsurgical or post traumatic). An awarenessof these patterns is crucial to makingcorrect scan interpretation and accuratediagnosis. We present a case of a patientwith primary lymphoedema where the scanpattern could have easily been confused
with that of secondary lymphoedema. Thisimage pattern though occasionally seen hasnot previously been reported.
Case report
A 26-year-old female with left lower limboedema of 16-month duration was referred tothe nuclear medicine department at theFarwania Hospital Kuwait, for lymphoscintigraphyto determine the underlying cause of her lowerlimb swelling.
Dynamic lymphoscintigraphy was performedfor 45 min following bipedal injections of99mTc-Nanocolloid into the first interdigital webspaces of the feet. Next, pre- and post-exercisestatic lower half-body scans were acquired. Theearly flow images did not show inguinal lymphnodes on either side, nor any activity in thelymphatic channels (Figure 1). The delayedpost-exercise images showed appearancessuggestive of dermal backflow in the left midthigh (Figure 2). On the right, there was noactivity seen above the mid calf level withapparent patchy dermal back flow only to thislevel. On careful review of the images, thepattern of the pooling of activity in the skin wasseen to be significantly different than theclassic dermal backflow pattern (Figure 3) andthe appearances were in keeping withcutaneous lymphatic microcirculatory flowthrough the lymphatic to flow through dilated
www.pjnm.net 2305-1630(201701/01)7:1<53:FECPAC>2.0.TX;2-M
*Correspondence
Qaisar Hussain SirajNuclear Medicine DepartmentFarwania HospitalPO Box 18373Kuwait 81004Email: [email protected]
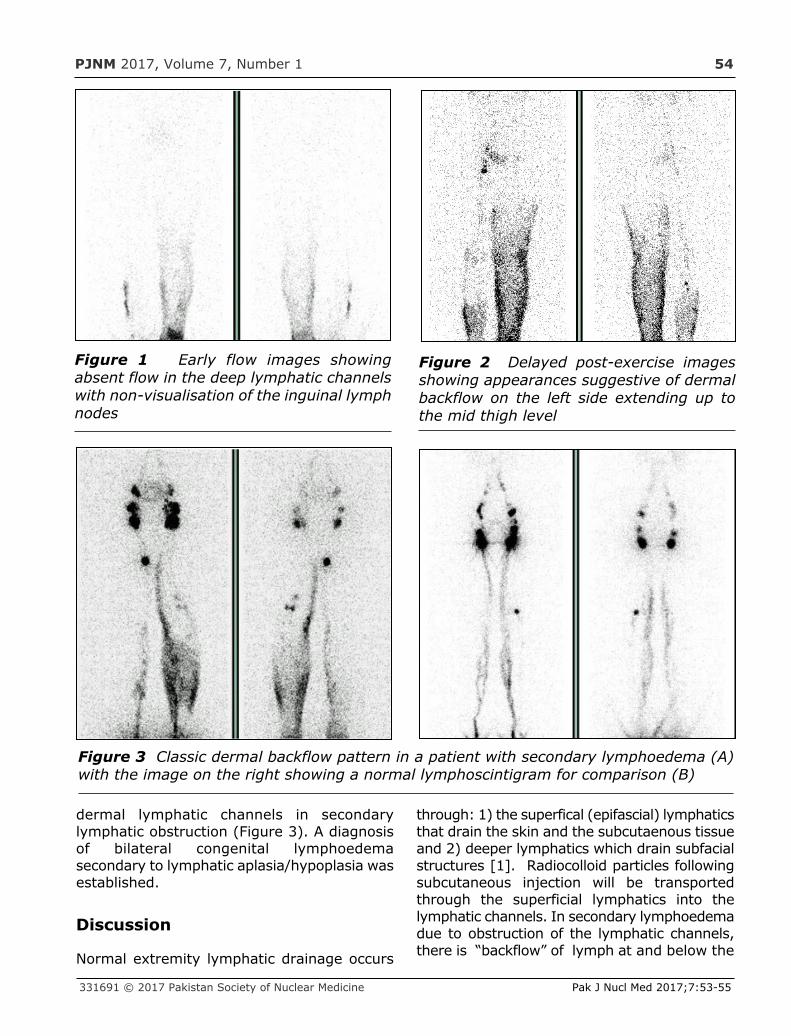
PJNM 2017, Volume 7, Number 1 54
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:53-55
dermal lymphatic channels in secondarylymphatic obstruction (Figure 3). A diagnosisof bilateral congenital lymphoedemasecondary to lymphatic aplasia/hypoplasia wasestablished.
Discussion
Normal extremity lymphatic drainage occurs
through: 1) the superfical (epifascial) lymphaticsthat drain the skin and the subcutaenous tissueand 2) deeper lymphatics which drain subfacialstructures [1]. Radiocolloid particles followingsubcutaneous injection will be transportedthrough the superficial lymphatics into thelymphatic channels. In secondary lymphoedemadue to obstruction of the lymphatic channels,there is “backflow” of lymph at and below the
Figure 1 Early flow images showingabsent flow in the deep lymphatic channelswith non-visualisation of the inguinal lymphnodes
Figure 2 Delayed post-exercise imagesshowing appearances suggestive of dermalbackflow on the left side extending up tothe mid thigh level
Figure 3 Classic dermal backflow pattern in a patient with secondary lymphoedema (A)with the image on the right showing a normal lymphoscintigram for comparison (B)

PJNM 2017, Volume 7, Number 1 55
Pak J Nucl Med 2017;7:53-55 2305-1630(201701/01)7:1<53:FECPAC>2.0.TX;2-M
level of the obstruction, from the lymphaticchannels into the dermal lymphatics, givingrise the pathognomic “dermal backflow” sign,which is typically seen as increased uptake inthe skin with dilated dermal lymphatics andan abrupt or “spirit level” type cut-off (Figure3 shows the typical “dermal backflow” in apatient with secondary lymphoedema).However, in primary lymphoedma, wherethere is aplasia or hypoplasia of the primarylymphatic channels, the lymphatic flow isreversed with predominant preferential flowthrough the dilated cutaneous epifasciallymphatics. This cutaneous lymphatic flow ischaracterised by diffuse increased superficialuptake ascending upwards toward the thighwithout any cut-off as can be seen in Figure2. In the absence of obstruction the normalphysiological flow through the superficial andthe deeper lymphatic networks remainseparate; however, there is preferential flowthrough one or the other lymphatic networkdepending on the nature of the obstruction(primary vs. secondary).
Conclusion
Dermal backflow is a feature of secondarylymphoedema and is absent in primarylymphoedema. This new image pattern of“cutaneous flow” on delayed imaging inprimary lymphoedema that mimics the“dermal backflow” pattern in secondarylymphoedema has to date not been reported.
An awareness of this “cutaneous” flow patternis important for correctly diagnosing primaryand secondary lymphoedema cases throughqualitative image evaluation and interpretationof lymphoscintigrams.
References
1. Szuba A, Shin WS, Strauss W, Rockson S.The third circulation: radionuclidelymphoscintigraphy in the evaluation oflymphedema. J Nucl Med 2003; 44(1):43-54.
PJNM 2017, 7:56-61 331691 © 2017 Pakistan Society of Nuclear Medicine
Bone scintigraphy in apatite-associateddestructive arthritis (Milwaukee
shoulder syndrome)
Qaisar Hussain Siraj
Departments of Nuclear Medicine,Charing Cross Hospital, London & Royal Hospital Haslar, Gosport, UK
CASE REPORT
Abstract
We report a case established of Milwaukeeshoulder syndrome (apatite-associated destructivearthritis) and describe the bone scintigraphic,radiologic and histologic findings, which arecompared with a similar case of rapid non-crystal-deposition arthritis. The cases shall addto the differential diagnosis of shoulderarthropathy on bone scintigraphy.
Key words: Milwaukee shoulder syndrome,Bone scan, Arthritis,
Introduction
Milwaukee shoulder syndrome is a destructivearthropathy associated with calcium hydroxyapatiteand calcium pyrophosphate dehydrate crystaldeposition mostly affecting elderly females. Wedescribe the bone scintigraphic pattern observed ina patient with an established diagnosis of Milwaukeeshoulder syndrome and in another patient in whom
the diagnosis was suspected on the basis of thebone scan appearances. The aim of the reportis to introduce this syndrome and documentthe bone scintigraphic findings for thedifferential diagnosis of shoulder arthropathy.A basic knowledge of this condition isimportant in order to recognize the uptakepattern often seen in patients undergoing bonescans with the primary complaint of painfulshoulder joints.
Case 1
A 76-year-old lady with chronic renal failurepresented with bilateral shoulder pain andswelling without any preceding history oftrauma. Her x-rays of the shoulders showedjoint narrowing, subchondral sclerosis andsubchondral bone destruction, andcalcifications in the joint capsule There wasbilateral rotator-cuff tear. US of theshoulders showed fluid collection andsynovial thickening. Synovial fluid wasaspirated which appeared haemorrhagic andpositive for calcium apatite crystals. Thepatient was referred to the nuclear medicinedepartment for a bone scan in Nov 1997.
Multiple spot views of the skeletal wereobtained to cover the entire skeleton 3 hoursafter an intravenous injection of 600 MBq
www.pjnm.net 2305-1630(201701/01)7:1<56:FECPAC>2.0.TX;2-M
*Correspondence
Qaisar Hussain SirajNuclear Medicine DepartmentFarwania HospitalPO Box 18373Kuwait 81004Email: [email protected]
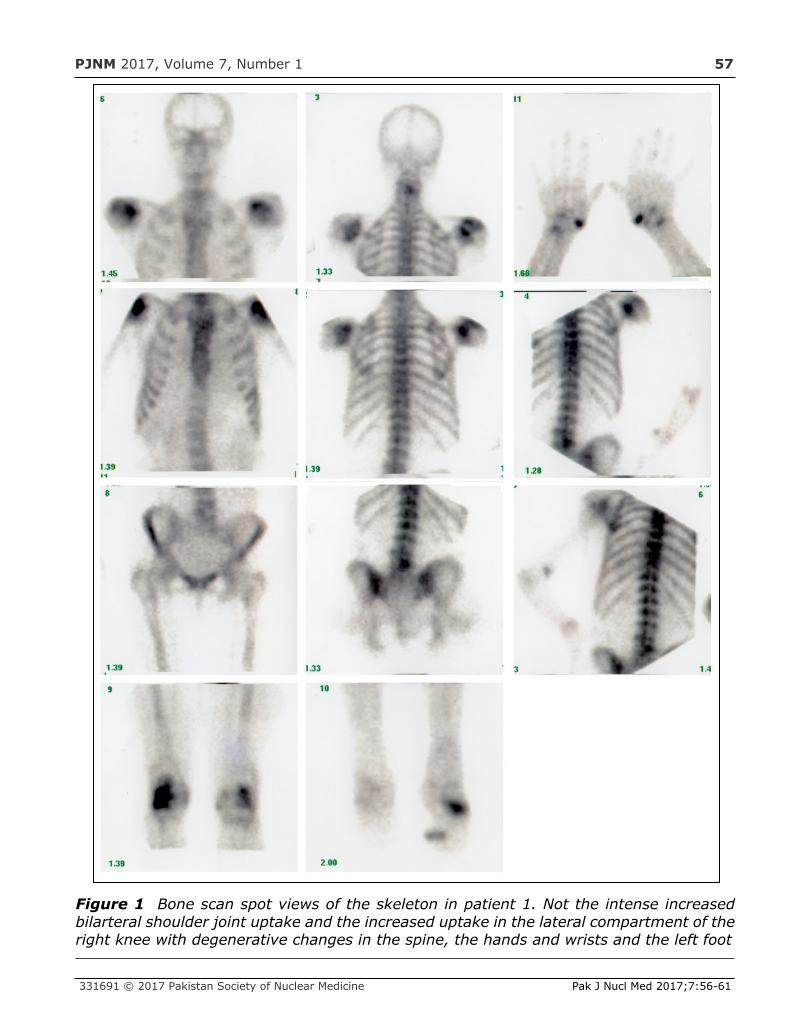
PJNM 2017, Volume 7, Number 1 57
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:56-61
Figure 1 Bone scan spot views of the skeleton in patient 1. Not the intense increasedbilarteral shoulder joint uptake and the increased uptake in the lateral compartment of theright knee with degenerative changes in the spine, the hands and wrists and the left foot

PJNM 2017, Volume 7, Number 1 58
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:56-61
99mTc-methylene diposphonate using a single-head camera fitted with a low-energy high-resolution collimator. The bone scan images(Figure 1) showed a high bone/soft-tissue ratiowith poor visualization of the kidneysconsistent with the known chronic renalfailure. There was intense increased uptakein both shoulder joints as well as the lateralcompartment of the right knee. These changestaken together with the x-rays and thesynovial fluid microscopy were consistent withMilwaukee shoulder syndrome. There was alsoincreased uptake seen in both 1st carpo-metacarpal joints and in the left tarsal regionand the base of the 1st left toe consistent with
arthritis. The changes in the shoulders werethought to be typical of Milwaukee shouldersyndrome and on basis of the increased uptakein the lateral compartment of the right knee,the knee joint was also thought to be involvedbut wasn't further investigated. The other joinswith active arthropathy were thought to bepossibly involved. The patient was treated withcolchicine and physiotherapy with symptomaticrelief. relief.
Case 2
A 97-year-old lady who presented withbilateral chronic shoulder and right hip pain
Figure 2 Whole-body bone scan of patient in Case 2. Note the intense increased bilateralshoulder joint uptake and the increased uptake in the right hip joint and the rib fractures
PJNM 2017, Volume 7, Number 1 59
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:56-61
referred to the nuclear medicine departmentof the Royal Hospital Haslar in Gosport, UK inSep 2000. X-rays of the shoulders showedjoint space narrowing with degenerativechanges and joint and peri-articular soft-tissuecalcifications.
A whole-body bone scan was performed 3hours after an intravenous injection of 640MBq 99mTc-methylene diposphonate using adouble headed ADAC gamma camera fittedwith a low-energy high-resolution collimator.The whole-body bone scan images (Figure 2)showed crescent-shaped areas of intenseincreased uptake in both shoulders correspondingto the glenohumeral joints. A similar patternof intense increased uptake was seen in theright hip. There changes were consistent withactive destructive arthritis of the bilateralshoulder and the right hip joints. The bonescan also showed scoliosis of the lumbar spineand focal increased uptake in the right 10-12ribs posteriorly consistent with rib fractures.X-rays of the shoulders showed moderatedegenerative changes. The scintigraphicfeatures were very suspicious of Milwaukeeshoulder syndrome and the patient was furtherinvestigated to establish or exclude thediagnosis. The bilateral large effusions in theshoulder joints were aspirated. The aspiratedfluid showed some lymphocytes andmacrophages but no crystals were identified.Rheumatoid factor was negative and there waspositive ANA with homogenous pattern whichwas thought to be of doubtful significance.The case was thought to be due to non-specificadvanced active arthropathy as a result offailed microscopic diagnosis of Milwaukeeshoulder syndrome.
Discussion
Milwaukee shoulder syndrome (MSS) was firstreported in 1981 in 4 elderly female patientsfrom the state of Milwaukee in the UnitedStates. The term was coined to describe theradiological, clinical and histological featuresseen in the shoulder joints of these patientswith chronic recurrent severe shoulder jointarthritis and joint effusions with x-rays showingrotator cuff tears and severe degenerative
joint disease [1-3]. Another report a year laterdescribed similar features introducing the termof rapid destructive arthritis of the shouldersfor the disease [4]. Further studies introducedother terms for the disease includinghaemorrhagic shoulder of the elderly, rapiddestructive arthritis of the shoulder, apatite-associated destructive arthritis and idiopathicdestructive arthritis of the shoulder, crystaldeposition disease, crystal-induced arthritis, etc.[5].
The involved joints show massive effusion,which is characteristically non-inflammatory,haemorrhagic with intraarticular calciumhydroxyapatite deposition that causes releaseof lysosomal enzymes resulting in destructionof the peri-articular tissue specially the rotatorcuff as well as the articular cartilage. Theshoulders are the most frequently involvedjoints but other joints such as the elbows,wrists, hands, hips, knees, and the feet aswell as the cervical and lumbar spine can beaffected [6]. Elderly age-group patients aremostly affected with a male:female ratio of1:4 [6-8].
The bone scan shows intense uptake in theaffected joints as well in the peri-articularcalcific soft-tissue deposits. Both of our casesshowed a similar pattern of uptake on the bonescan in the shoulders though the right kneewas seen to be involved in Case 1 where theuptake was seen to involve lateral tibiofemoralcompartment, which is the reported patternof knee involvement in Milwaukee shoulder-knee syndrome [9]. A somewhat characteristicappearance of crescentic increased activity inthe joint cavity as compared with that seen inthe articular regions was observed, presumablydue to bone crystal uptake in these cases ofcrystalline arthropathy (Figures 1 & 2).Although bone scintigraphy in these patientsis highly sensitive, it appears rather non-specific with the scintigraphic features similarto those seen in other types of arthritis.
The bone scan of the patient in Case 2 showedintense bilateral glenohumeral joint and righthip joint uptake with peak of activity confinedto the joint cavity (Figure 2). This uptakepattern was similar to that seen in Case 1, but
Figure 3 Early (left) and delayed (right)postoperative 99mTc-MIBI scan showing
PJNM 2017, Volume 7, Number 1 60
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:56-61
here microscopy revealed absence of crystals.Despite this, the case was clinically diagnosedand treated as Milwaukee shoulder syndrome.The detection of basic calcium phosphate(BCP) crystals in the synovial fluid of patientswith arthropathy is challenging due to thesubmicroscopic size of BCP, the complexnature of the matrix in which they are foundand the fact that other crystals can co-existwith them in cases of mixed pathology [10].Routine analysis of joint crystals relies almostexclusively on the use of optical microscopy,which has limited applicability for BCP crystalidentification due to limited resolution and theinherent subjectivity of the technique [10].
The key mechanisms whereby BCP crystalsmay cause tissue damage are: (1) theinduction of mitogenesis; (2) the upregulationof matrix metalloproteinase (MMP) production;(3) the stimulation of cyclooxygenases 1 and2 and prostaglandin E2 production; (4) thestimulation of cytokine production, and (5) theinduction of nitric oxide production [11].
Factors that may predispose to this syndromeinclude deposition of calcium pyrophosphatedihydrate crystals, direct trauma or chronicjoint overuse, denervation and chronic renalfailure [12]. Chronic renal impairment was thepredisposing risk factor in Case 1 in this report.
The treatment in these cases is supportive andinvolves resting the affected joint(s),prescription of nonsteroidal anti-inflammatoryagents. Refractory cases are suitably treatedwith substitution of magnesium-containingNSAID and oral chochicine [13].
References
1. McCarty DJ, Halverson PB, Carrera GF.Milwaukee shoulder—association ofmicrospheroids containing hydroxyapatitecrystals, active collagenase, and neutralprotease with rotator cuff defects. I:clinical aspects. Arthritis and Rheumatism1981;24(3):464–473.
2. Halverson PB, Cheung HS, McCarty DJ.
Milwaukee shoulder—association ofmicrospheroids containing hydroxyapatitecrystals, active collagenase, and neutralprotease with rotator cuff defects. II:synovial fluid studies. Arthritis andRheumatism 1981;24(3):474–483.
3. Garancis JC, Cheung HS, Halverson PB,McCarty DJ. Milwaukee shoulder—association of microspheroids containinghydroxyapatite crystals, activecollagenase, and neutral protease withrotator cuff defects. III: morphologic andbiochemical studies of an excisedsynovium showing chondromatosis.Arthritis and Rheumatism1981;24(3):484–491.
4. Lequesne M, Fallut M, Coulomb R et al.L’arthropathie destructrice rapide del’´epaule. Revue du Rhumatisme1982;49:427–437.
5. Neer II CS, Craig EV, Fukuda H. Cuff-teararthropathy. Journal of Bone and JointSurgery 1983;65(9):1232-1244.
6. Genta MS, Gabay C. Milwaukee Shoulder.New Engl J Med 2006;354(2), article e2,2006.
7. McCarty DJ. Milwaukee shouldersyndrome. Trans Am Clin ClimatologAssoc. 1990;102:271–283.
8. Nguyen VD. Rapid destructive arthritis ofthe shoulder. Skeletal Radiol.1996;25(2):107–112.
9. Halverson PB, Carrera GF, McCarty DJ.Milwaukee shoulder syndrome. Fifteenadditional cases and a description ofcontributing factors. Archives of InternalMedicine 1990;150(3):677 82.
10. Yavorskyy A, Hernandez-Santana A,McCarthy G, McMahonc G. Detection ofcalcium phosphate crystals in the jointfluid of patients with osteoarthritis -analytical approaches and challenges.Analyst. 2008 Mar; 133(3): 302-318.
Figure 3 Early (left) and delayed (right)postoperative 99mTc-MIBI scan showing
PJNM 2017, Volume 7, Number 1 61
Pak J Nucl Med 2017;7:56-61 2305-1630(201701/01)7:1<56:FECPAC>2.0.TX;2-M
11. Molloy ES, McCarthy GM. Basic calciumphosphate crystals: pathways to jointdegeneration. Curr Opin Rheumatol.2006;18(2):187-192.
12. Halverson PB1, Carrera GF, McCarty DJ.Milwaukee shoulder syndrome. Fifteenadditional cases and a description ofcontributing factors. Arch Intern Med.1990 Mar;150(3):677-82.
13. Nguyen VD. Rapid destructive arthritis ofthe shoulder. Skeletal Radiology1996;25(2):107-12.
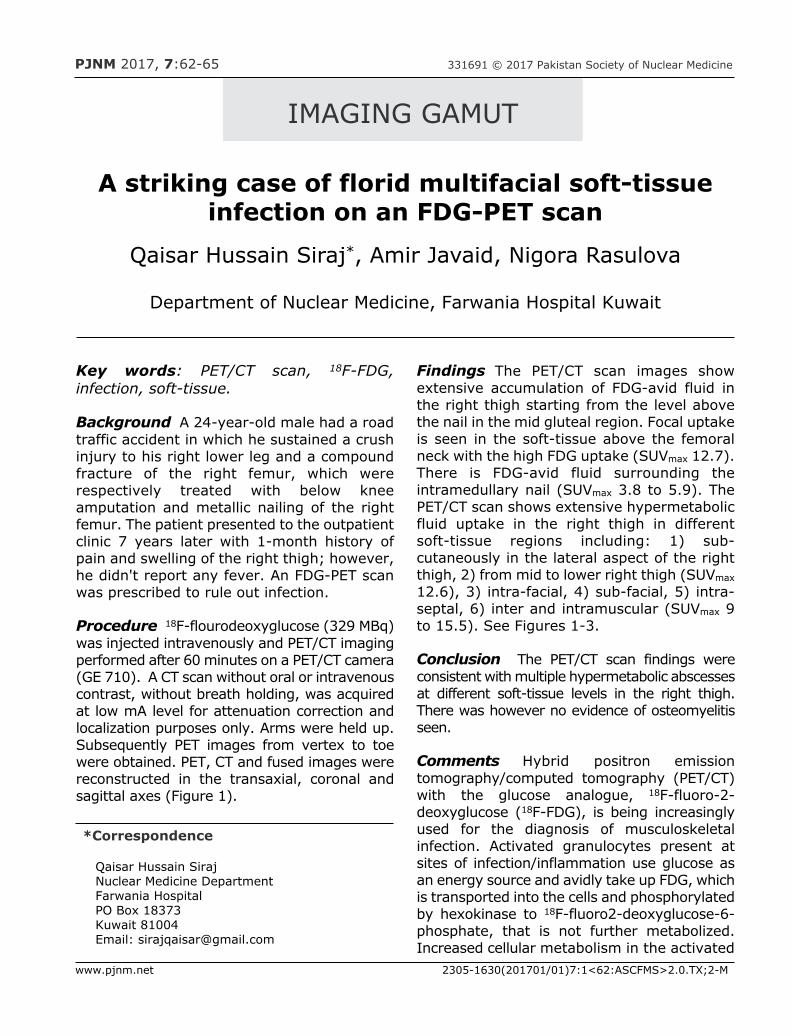
PJNM 2017, 7:62-65 331691 © 2017 Pakistan Society of Nuclear Medicine
A striking case of florid multifacial soft-tissueinfection on an FDG-PET scan
Qaisar Hussain Siraj*, Amir Javaid, Nigora Rasulova
Department of Nuclear Medicine, Farwania Hospital Kuwait
IMAGING GAMUT
Key words: PET/CT scan, 18F-FDG,infection, soft-tissue.
Background A 24-year-old male had a roadtraffic accident in which he sustained a crushinjury to his right lower leg and a compoundfracture of the right femur, which wererespectively treated with below kneeamputation and metallic nailing of the rightfemur. The patient presented to the outpatientclinic 7 years later with 1-month history ofpain and swelling of the right thigh; however,he didn't report any fever. An FDG-PET scanwas prescribed to rule out infection.
Procedure 18F-flourodeoxyglucose (329 MBq)was injected intravenously and PET/CT imagingperformed after 60 minutes on a PET/CT camera(GE 710). A CT scan without oral or intravenouscontrast, without breath holding, was acquiredat low mA level for attenuation correction andlocalization purposes only. Arms were held up.Subsequently PET images from vertex to toewere obtained. PET, CT and fused images werereconstructed in the transaxial, coronal andsagittal axes (Figure 1).
Findings The PET/CT scan images showextensive accumulation of FDG-avid fluid inthe right thigh starting from the level abovethe nail in the mid gluteal region. Focal uptakeis seen in the soft-tissue above the femoralneck with the high FDG uptake (SUVmax 12.7).There is FDG-avid fluid surrounding theintramedullary nail (SUVmax 3.8 to 5.9). ThePET/CT scan shows extensive hypermetabolicfluid uptake in the right thigh in differentsoft-tissue regions including: 1) sub-cutaneously in the lateral aspect of the rightthigh, 2) from mid to lower right thigh (SUVmax
12.6), 3) intra-facial, 4) sub-facial, 5) intra-septal, 6) inter and intramuscular (SUVmax 9to 15.5). See Figures 1-3.
Conclusion The PET/CT scan findings wereconsistent with multiple hypermetabolic abscessesat different soft-tissue levels in the right thigh.There was however no evidence of osteomyelitisseen.
Comments Hybrid positron emissiontomography/computed tomography (PET/CT)with the glucose analogue, 18F-fluoro-2-deoxyglucose (18F-FDG), is being increasinglyused for the diagnosis of musculoskeletalinfection. Activated granulocytes present atsites of infection/inflammation use glucose asan energy source and avidly take up FDG, whichis transported into the cells and phosphorylatedby hexokinase to 18F-fluoro2-deoxyglucose-6-phosphate, that is not further metabolized.Increased cellular metabolism in the activated
*Correspondence
Qaisar Hussain SirajNuclear Medicine DepartmentFarwania HospitalPO Box 18373Kuwait 81004Email: [email protected]
www.pjnm.net 2305-1630(201701/01)7:1<62:ASCFMS>2.0.TX;2-M
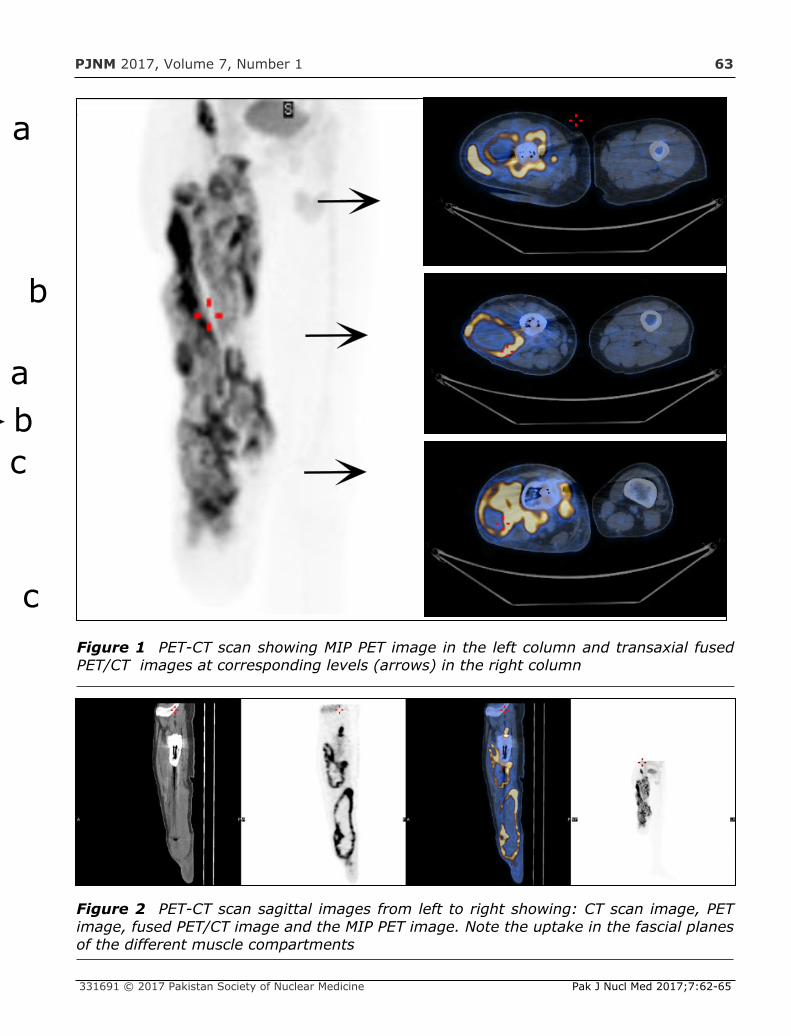
PJNM 2017, Volume 7, Number 1 63
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:62-65
Figure 1 PET-CT scan showing MIP PET image in the left column and transaxial fusedPET/CT images at corresponding levels (arrows) in the right column
b
c
a
ba
c
a
Figure 2 PET-CT scan sagittal images from left to right showing: CT scan image, PETimage, fused PET/CT image and the MIP PET image. Note the uptake in the fascial planesof the different muscle compartments
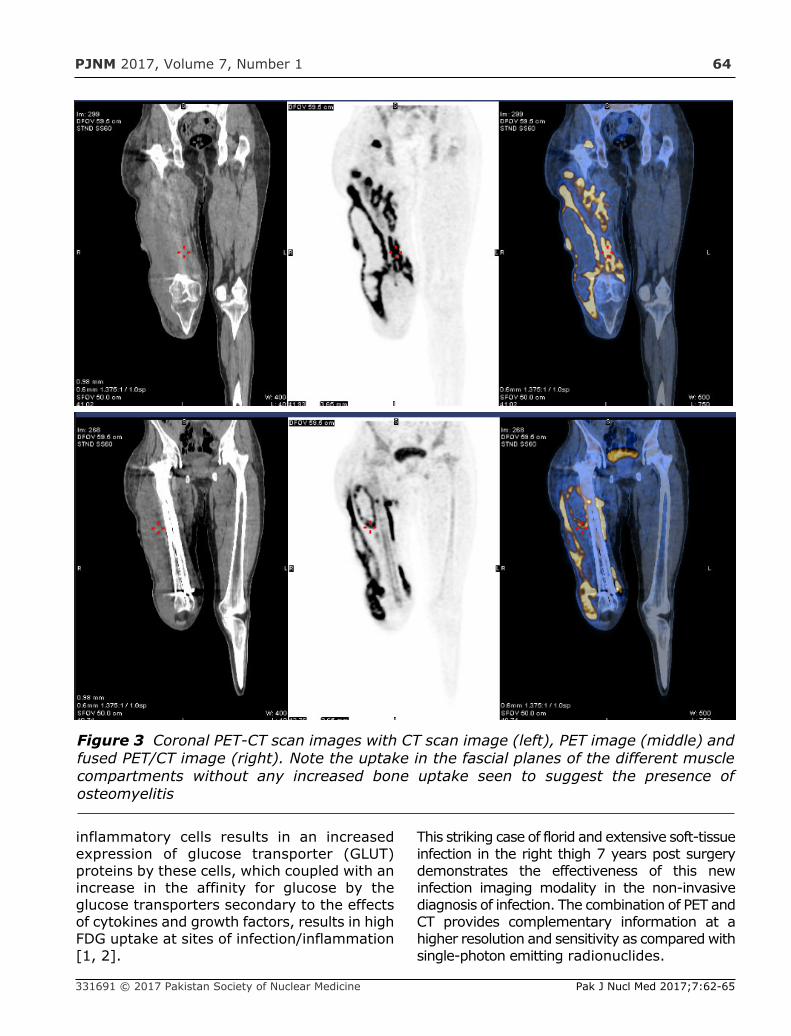
PJNM 2017, Volume 7, Number 1 64
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:62-65
inflammatory cells results in an increasedexpression of glucose transporter (GLUT)proteins by these cells, which coupled with anincrease in the affinity for glucose by theglucose transporters secondary to the effectsof cytokines and growth factors, results in highFDG uptake at sites of infection/inflammation[1, 2].
This striking case of florid and extensive soft-tissueinfection in the right thigh 7 years post surgerydemonstrates the effectiveness of this newinfection imaging modality in the non-invasivediagnosis of infection. The combination of PET andCT provides complementary information at ahigher resolution and sensitivity as compared withsingle-photon emitting radionuclides.
Figure 3 Coronal PET-CT scan images with CT scan image (left), PET image (middle) andfused PET/CT image (right). Note the uptake in the fascial planes of the different musclecompartments without any increased bone uptake seen to suggest the presence ofosteomyelitis
PJNM 2017, Volume 7, Number 1 65
Pak J Nucl Med 2017;7:62-65 2305-1630(201701/01)7:1<62:ASCFMS>2.0.TX;2-M
FDG-PET technique demonstrates themetabolic changes that occur earlier comparedto the anatomical changes seen by CT or MRIalone. The high metabolic activity of infectiveabscesses due to a high degree of FDG aviditycoupled with structural CT changes of infectionfacilitates rapid interpretation of both theseverity and the extent of infection and helpsdelineate osseous from soft-tissue involvement.The PET/CT scan in this case showed multiplehypermetabolic areas which were preciselylocalized to the soft-tissue and showed nobone involvement. The findings are extremelyhelpful in determining and instituting theappropriate treatment and also useful formonitoring the therapeutic efficacy.
References
1. Signore A, Glaudemans AWJM. Themolecular imaging approach to imageinfections and inflammation by nuclearmedicine techniques. Annals of NuclearMedicine, 2011;25(10):681–700.
2. de Winter F, van de Wiele C, VogelaersD,et al. Fluorine-18 fluorodeoxyglucosepositron emission tomography: a highlyaccurate imaging modality for thediagnosis of chronic musculoskeletalinfections. J Bone Joint Surg Am, 2001;83-A:651-660.

PJNM 2017, 7:66-68 331691 © 2017 Pakistan Society of Nuclear Medicine
Unusual breast radioiodine uptake in a non-breastfeeding woman with papillary thyroid
carcinomaYassir Benameur*, Hasnae Guerrouj, Salah Nabih Oueriagli,
Omar Ait Sahel, Imad Ghfir, Nouzha Ben Raïs Aouad
Department of Nuclear Medicine, IBN-SINA Hospital Center,University Med V-Rabat, Morocco
IMAGING GAMUT
Key words: Whole-body scintigraphy,radioiodine, papillary thyroid carcinoma,soft-tissue uptake
Background A 48-year-old woman underwenttotal thyroidectomy for a multinodular goiter.Histopathological examination revealed papillarythyroid carcinoma.
The patient was referred to the nuclear medicinedepartment for ablative dose of iodine-131iodine (3.7 GBq) and post therapy radioiodinescan. Thyroglobulin level was at 11 ng/ml.
Procedure Planar whole-body radioiodinescintigraphy was performed in the anterior andposterior projections 5 days after the ablativedose of 131I. Single-photon emission computedtomography (SPECT-CT) was additionallyperformed for anatomical localization of thethoracic radioiodine-avid foci.
*Correspondence
Dr Yassir BenameurNuclear Medicine DepartmentIBN-SINA Hospital CenterUniversity Med V-RabatRabat, MoroccoTel: 0021 2661209162Email: [email protected]
www.pjnm.net 2305-1630(201701/01)7:1<66:MOOBSP>2.0.TX;2-M
Figure 1 Planar 131I whole-body scanshowing two thoracic radioiodine-avid fociprobably outside the pulmonary fields
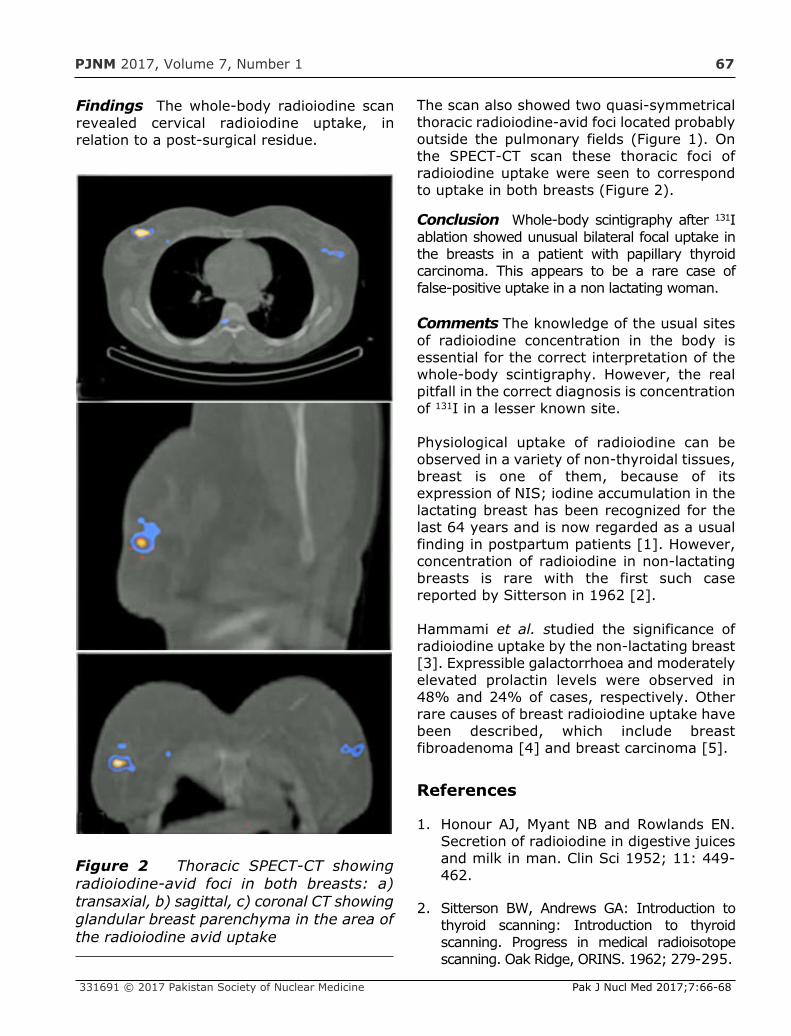
PJNM 2017, Volume 7, Number 1 67
Findings The whole-body radioiodine scanrevealed cervical radioiodine uptake, inrelation to a post-surgical residue.
The scan also showed two quasi-symmetricalthoracic radioiodine-avid foci located probablyoutside the pulmonary fields (Figure 1). Onthe SPECT-CT scan these thoracic foci ofradioiodine uptake were seen to correspondto uptake in both breasts (Figure 2).
Conclusion Whole-body scintigraphy after 131Iablation showed unusual bilateral focal uptake inthe breasts in a patient with papillary thyroidcarcinoma. This appears to be a rare case offalse-positive uptake in a non lactating woman.
Comments The knowledge of the usual sitesof radioiodine concentration in the body isessential for the correct interpretation of thewhole-body scintigraphy. However, the realpitfall in the correct diagnosis is concentrationof 131I in a lesser known site.
Physiological uptake of radioiodine can beobserved in a variety of non-thyroidal tissues,breast is one of them, because of itsexpression of NIS; iodine accumulation in thelactating breast has been recognized for thelast 64 years and is now regarded as a usualfinding in postpartum patients [1]. However,concentration of radioiodine in non-lactatingbreasts is rare with the first such casereported by Sitterson in 1962 [2].
Hammami et al. studied the significance ofradioiodine uptake by the non-lactating breast[3]. Expressible galactorrhoea and moderatelyelevated prolactin levels were observed in48% and 24% of cases, respectively. Otherrare causes of breast radioiodine uptake havebeen described, which include breastfibroadenoma [4] and breast carcinoma [5].
References
1. Honour AJ, Myant NB and Rowlands EN.Secretion of radioiodine in digestive juicesand milk in man. Clin Sci 1952; 11: 449-462.
2. Sitterson BW, Andrews GA: Introduction tothyroid scanning: Introduction to thyroidscanning. Progress in medical radioisotopescanning. Oak Ridge, ORINS. 1962; 279-295.
331691 © 2017 Pakistan Society of Nuclear Medicine Pak J Nucl Med 2017;7:66-68
Figure 2 Thoracic SPECT-CT showingradioiodine-avid foci in both breasts: a)transaxial, b) sagittal, c) coronal CT showingglandular breast parenchyma in the area ofthe radioiodine avid uptake

PJNM 2016, Volume 6, Number 1 68
Pak J Nucl Med 2017;7:66-68 2305-1630(201701/01)7:1<66:MOOBSP>2.0.TX;2-M
3. Hammami MM and Bakheet S. Radioiodinebreast uptake in nonbreastfeeding women:clinical and scintigraphic characteristics. JNucl Med 1996; 37: 26-31.
4. Berger F, Unterholzner S, Diebold J,Knesewitsch P, Hahn K, Spitzweg C.Mammary radioiodine accumulation due tofunctional sodium iodide symporterexpression in a benign fibroadenoma.Biochem Biophys Res Commun 2006;3 49:1258-63.
5. Wapnir IL, Goris M, Yudd A, Dohan O,Adelman D, Nowels K, et al. The Na+/I-symporter mediates iodide uptake in breastcancer metastases and can be selectivelydown-regulated in the thyroid. Clin CancerRes 2004;10: 4294-302.

ORIGINAL ARTICLESA brief review of targetted radionuclide therapiesMohammed Hathaf Al-Rowaily, Daniele Dondi, Marco Chinol, Iqbal Munir, Muaadh AbdualrehmanAlasbahi
1
Determination of the optimum filter for 99mTc SPECT breast imaging using a wire meshcollimatorXianling Dong, MI Saripan, R. Mahmud, S. Mashohor, Aihui Wang
8
Measurement of radiation doses to occupational workers in nuclear medicineMisbah Javed, Saeed Ur Rahman, Iqra Tanveer, Ghulam Asghar, Shazia Fatima, Mohammad Fahim
18
Behaviour of wedges for different field sizes and depthsSajjad Ahmed Memon, Naeem Ahmed Laghari, Fayaz Hussain Mangi
24
Pre-operative cardiac risk stratification for non-cardiac surgery in cancer patients usingmyocardial perfusion scintigraphyIqbal Munir, Amrah Javaid, Khalid Nawaz, Mohammed Hathaf Al-Rowaily, Muaadh Abdualrehman Al-Asbahi
34
Clinical characteristics and long-term outcome of patients with differentiated carcinomaof thyroid with bone metastases: a retrospective studySadaf Tufail Butt, Shazia Fatima, Noreen Marwat, Kahkashan Mir, Ayesha Ammar, MohammadFaheem
43
CASE REPORTSSuccessful Ra-223 treatment with a long interval between the second and the thirdcycles: a case reportTatiana Kochetova, Valeriy Krylov
48
Cutaneous flow pattern of primary lymphoedemaQaisar Hussain Siraj
53
Bone scintigraphy in apatite-associated destructive arthritis (Milwaukeeshoulder syndrome)Qaisar Hussain Siraj
56
IMAGING GAMUTSA striking case of florid multifacial soft-tissue infection on an FDG-PET scanQaisar Hussain Siraj, Amir Javaid, Nigora Rasulova
62
Unusual breast radioiodine uptake in a non- breastfeeding woman with papillary thyroidcarcinomaYassir Benameur, Hasnae Guerrouj, Salah Nabih Oueriagli, Omar Ait Sahel, Imad Ghfir, Nouzha BenRaïs Aouad
66