Presentación de PowerPoint - Foro de Debate en … · mantienen la dependencia de la regulación...
40
21-24-JUNIO 2017
Transcript of Presentación de PowerPoint - Foro de Debate en … · mantienen la dependencia de la regulación...

21-24-JUNIO 2017
Hannahan D & Weinberg R. Cell 2000, Cell 2011
The Hallmarks of Cancer

Sherr C. NEJM 2016
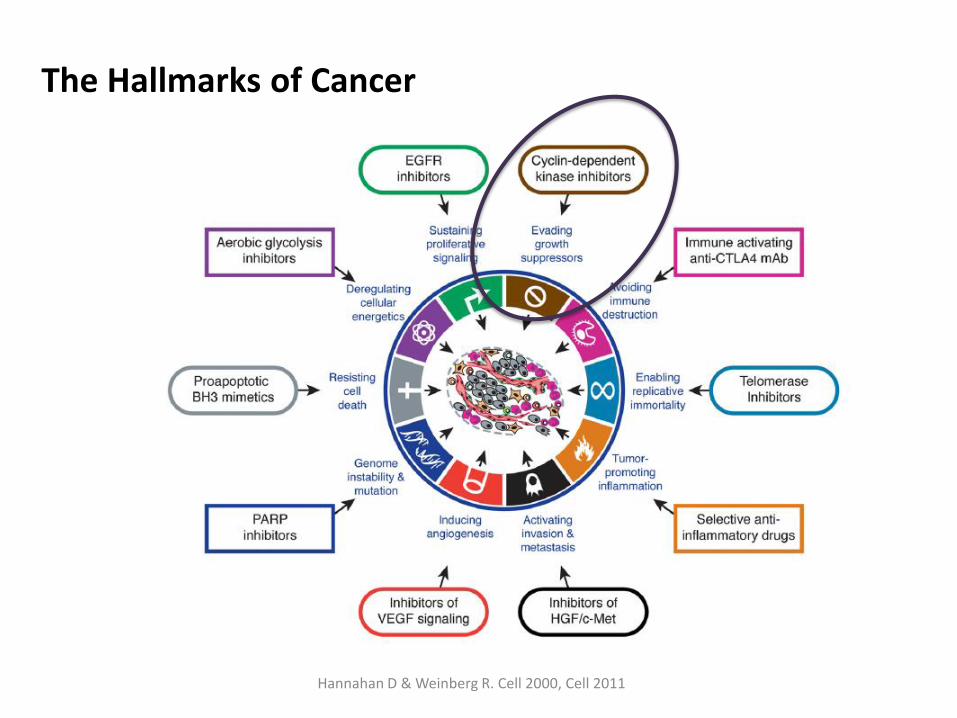
- Ciclinas/Kinasas dependientes de Ciclinas (C-CDK) – parte de la maquinaria que regula la secuencia del ciclo celular
- Mecanismos redundantes. Ausencia individual no es incompatible con la vida
- Predominan unos u otros en función del tipo celular - Maquinaria ciclo celular - Oncogenes, genes supresores - G1 S- Punto de Restricción – Regulado por la proteína Rb - Complejo ciclina D/CDK4/6 reguladores de la transición G1S
Ciclo celular
Garrido Castro A Curr Breast Cancer Rep 2017
INK4
Cip/Kip

Inhibición de CDKs
• Produce un stop de la evolución del ciclo celular
• Reversible a corto plazo
• La inhibicion mantenida lleva a las celulas a la muerte por apoptosis y senescencia

Ciclina D-CDK4/6 en cáncer de mama
• Sobreexpresión de CCND1 – proliferación mamaria anormal. 15% Amplificación del gen.
• Ratones Knockout D1 son resistentes a la formacion de canceres de mama inducidos por ErbB2 o Ras (pero no a los inducidos por otras vias)
• 47% perdida de p16INK4A
• D1/CDK4 importante para el mantenimiento de tumores establecidos

Ciclina D-CDK4/6 en cáncer de mama
• El estímulo E-dependiente del crecimiento es dependiente de la ciclina D1
• Los tumores que se hacen resistentes a la terapia endocrina mantienen la dependencia de la regulación D-CDKs
• El eje HER2-PIK3CA activado aumenta los niveles de Ciclina D1
• Los tumores Luminal A, B y HER2 enriquecidos frecuentemente tienen amplificacion de CCND1
• Los tumores luminales tiene proteina Rb funcional y altos niveles / Los tumores basales suelen presentar perdida funcional de Rb
• Modelos preclínicos – Actividad en modelos ER+, HER2 y sinergismo con TMX en ER+.

CDKi en modelos celulares Ca mama
Finn R CBC 2009
Cell lines representing luminal (ER+) subtype (including those HER2 amplified) were most sensitive to growth inhibition by PD 0332991 while nonluminal/basal subtypes were most resistant.
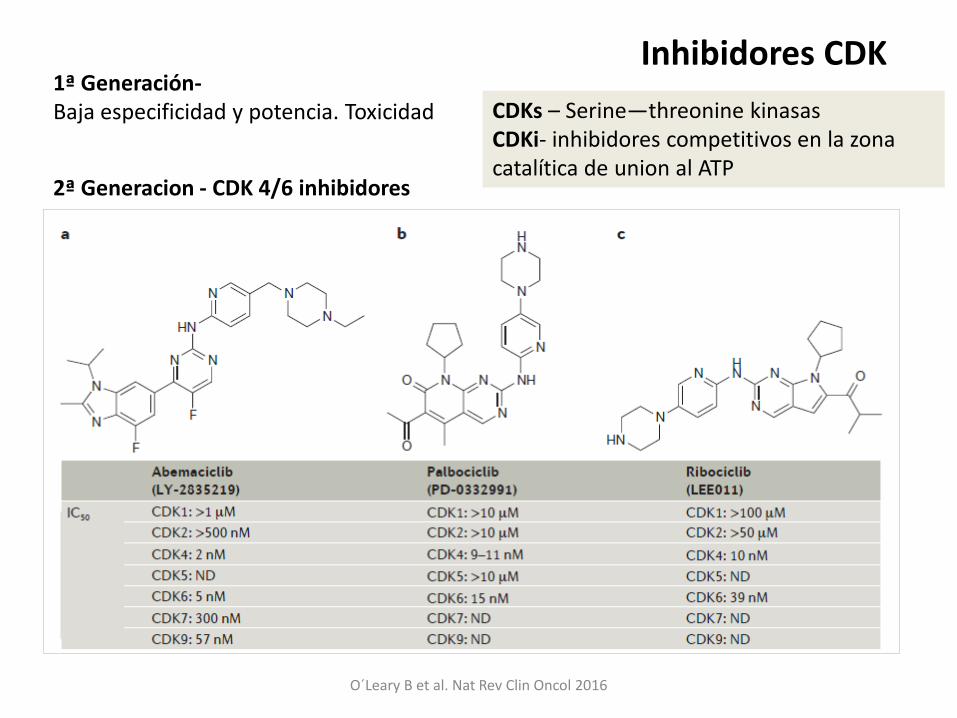
O´Leary B et al. Nat Rev Clin Oncol 2016
1ª Generación- Baja especificidad y potencia. Toxicidad
2ª Generacion - CDK 4/6 inhibidores
Inhibidores CDK
CDKs – Serine—threonine kinasas CDKi- inhibidores competitivos en la zona catalítica de union al ATP
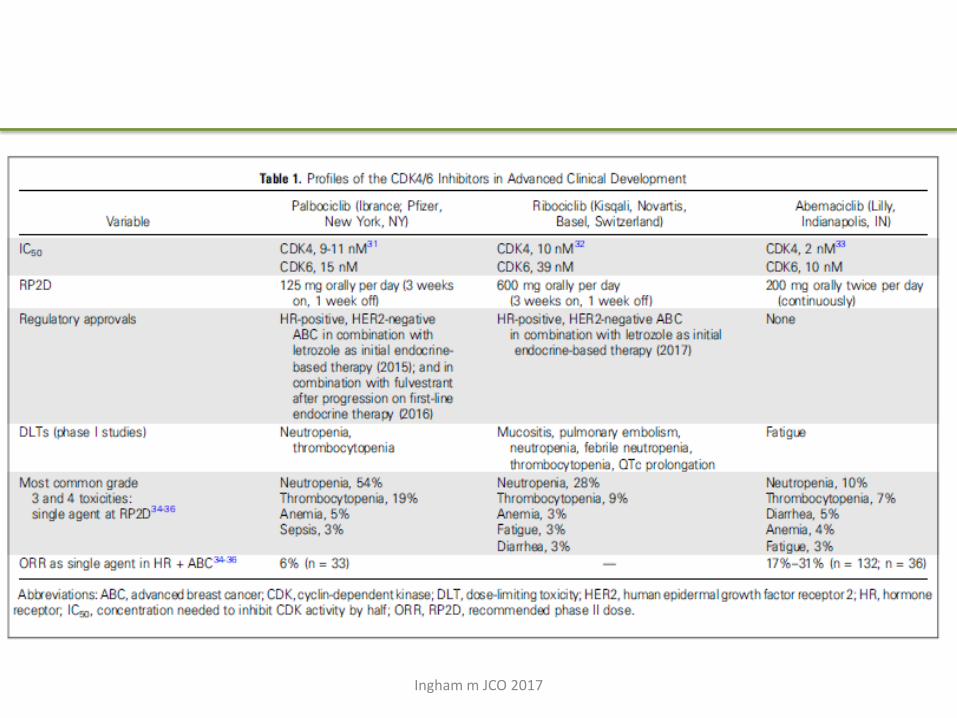
Ingham m JCO 2017

ESTUDIOS EN PRIMERA LÍNEA -- ENFERMEDAD HORMONOSENSIBLE--
• “De novo” disease • Relapse after > 1y from completion of adjuvant ET
• Metastatic disease – 1st line therapy
N Engl J Med 2016;375:1925-36.
N Engl J Med 2016;375:1738-48.
Lancet Oncol 2015; 16: 25–35
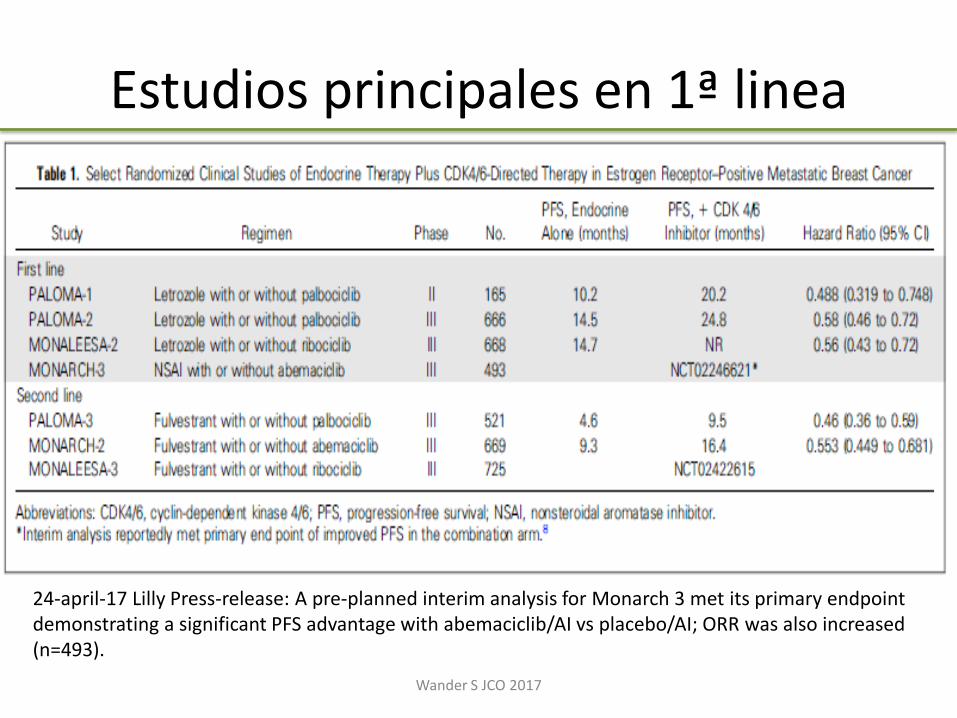
Estudios principales en 1ª linea
Wander S JCO 2017
24-april-17 Lilly Press-release: A pre-planned interim analysis for Monarch 3 met its primary endpoint demonstrating a significant PFS advantage with abemaciclib/AI vs placebo/AI; ORR was also increased (n=493).
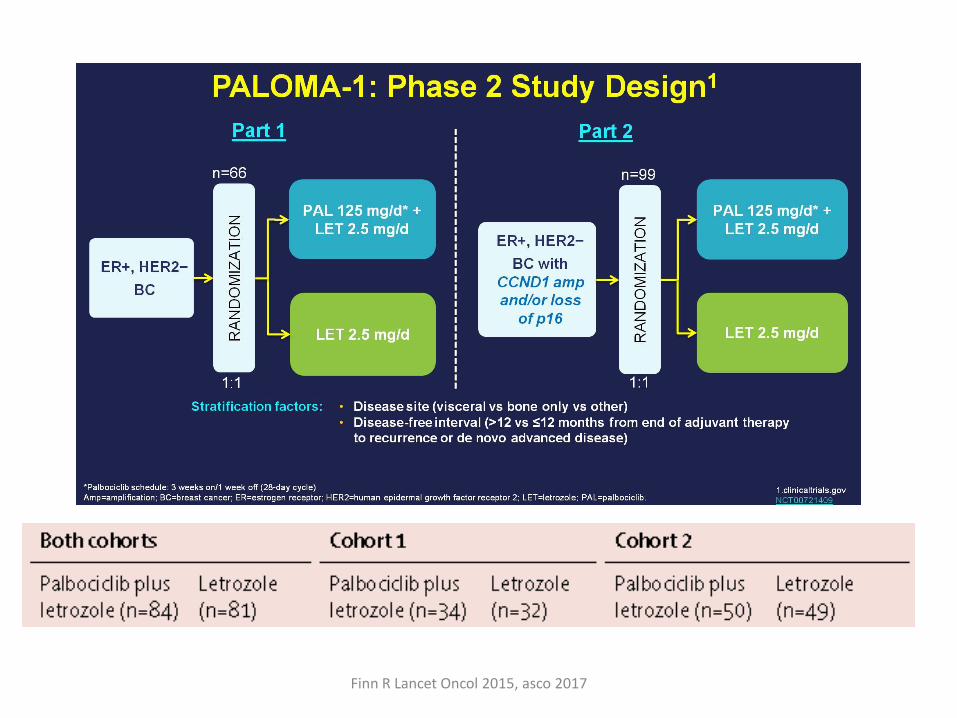
Finn R Lancet Oncol 2015, asco 2017
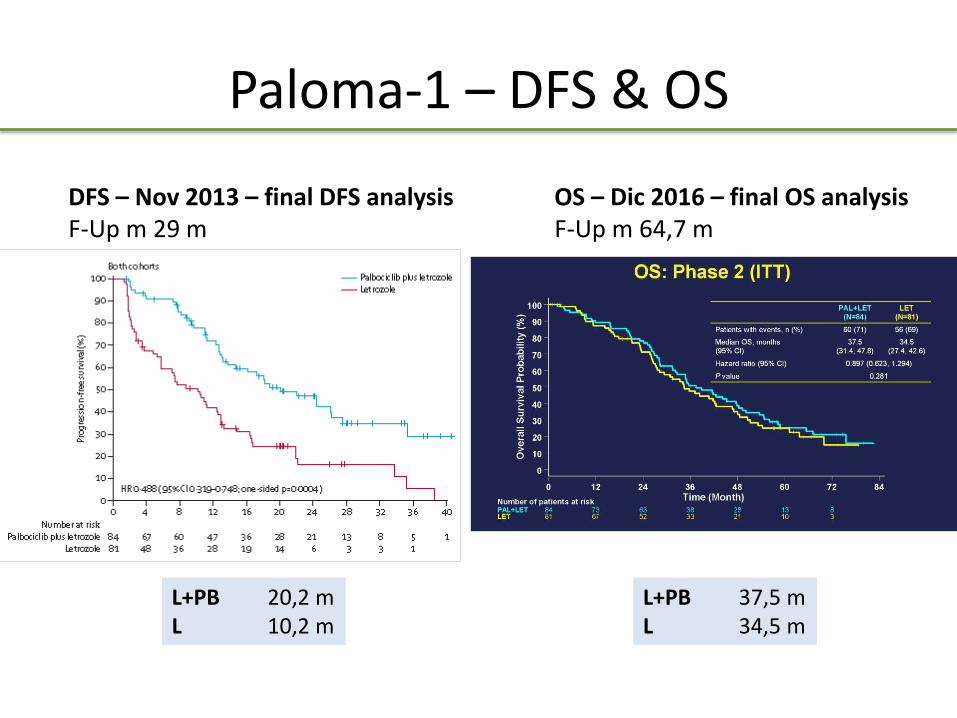
Paloma-1 – DFS & OS
L+PB 20,2 m L 10,2 m
DFS – Nov 2013 – final DFS analysis F-Up m 29 m
OS – Dic 2016 – final OS analysis F-Up m 64,7 m
L+PB 37,5 m L 34,5 m

CMM RH+/HER2- - HT 1ª línea
IA vs TMX1
(5 trials)
SWOG-
S02262
FACT3 FALCON4 PALOMA-25 MONALEESA-26
N 2400 694 514 524 666 521
M de novo NA 42% 30% 43% 37% 34%
HT previa NA 40% 69% NO 56% 52%
Ramas IA
TMX
Anastrozol
Ana + Fulv 250
Anastrozol
Ana + Fulv 250
Anastrozol
Fulvestrant 500
Letrozol
L + Palbociclib
Letrozol
L + Ribociclib
SLP IA: 8,2-12
TMX: 5,6-8,3
A: 13,5
A+F: 15
A: 10,2
A+F: 10,8
A: 13,8 m
F: 16, 6 m
L: 14,5 m
L+P: 24,8 m
L: 16
L+R: 25,3
HR 0,68-0,99 0,8
P 0,007
0,99
P 0,91
0,79
P 0.048
0.58
P<0.001
0.56
P = 9.63 × 10−8
1.Riemsma R, et al. Breast Ca Res Treat 2010; 2.Mehta RS et al. NEJM 2012; 3.Bergh J et al JCO 2012; 4.Robertson J et al. Lancet 2016; 5.Finn R et al. NEJM 2016; 6.Hortobagyi G et al. NEJM 2016; Hortobagyi G et al ASCO 2017

CDK4/6 1ª línea
Ingham m JCO 2017
Ribociclib – aumento del QTc > 480 ms en el 3%

OP- SLP
PALOMA-2 MONALEESA- 2
SG – NA – datos no maduros
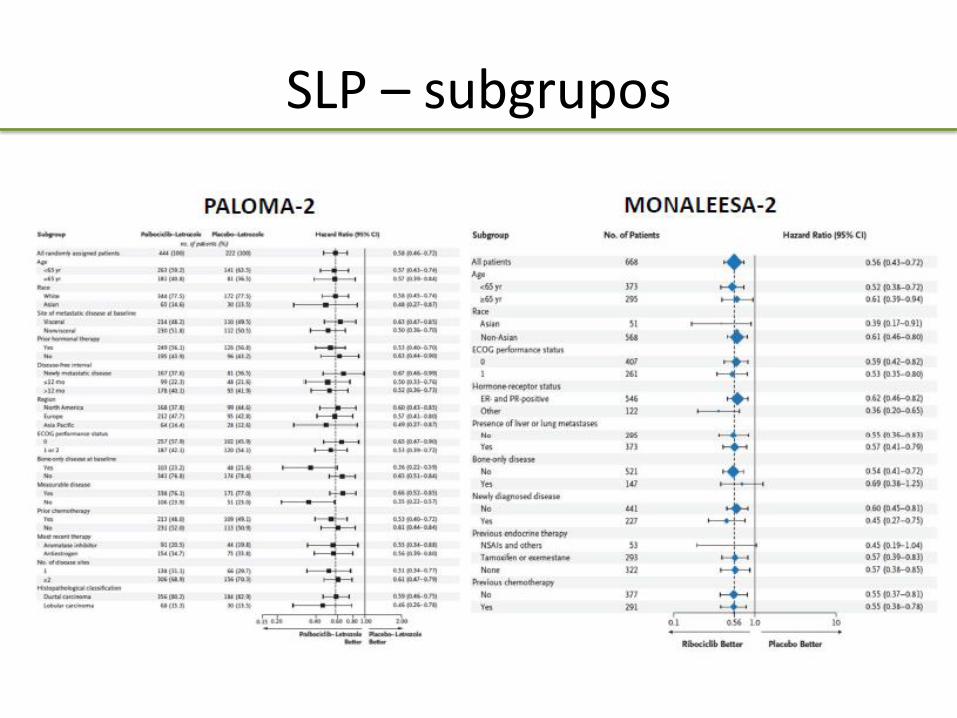
SLP – subgrupos
ESTUDIOS EN SEGUNDA LÍNEA -- RESISTENCIA ENDOCRINA --
• Relapse on adjuvant endocrine therapy
• Relapse within 1y from completion of adjuvant ET
• Metastatic disease > 1 line of ET

F= Fulvestrant 500, PB= Palbociclib, AB=Abemaciclib, EXE= Exemestano, EVE= Everolimus 10 mg, PL= Placebo, NEAI: non steroideal aromatase inhibitors -- * +GHRH agonist
Palbociclib 125 mg v.o/d x21 d /28 d + Fulvestrant 500 i.m /28 d + LD
Abemaciclib 200 mg/12 h continuous Amendment: 150 mg/12 h + Fulvestrant 500 i.m./28 d + LD
1 Cristofanilli M et al. Lancet Oncol 2016; 2 Sledge G et al. JCO 2017; 3 Baselga J et al. NEJM 2012. Piccart M et al. Ann Oncol 2014; 4 Kornblum N et al. SABCS 2016; 5 Di Leo et al. JCO 2010. Di Leo et al. JNCI 2013


PALOMA-3 MONARCH- 2
OP- SLP
SG – NA – nº eventos insuficiente

PI3K mutado y ESR1 mutado - Peor pronostico - No predictores de beneficio diferencial
PALOMA-3 MONARCH- 2

Evolución tras progresión – Datos Paloma 3
Turner et al. SABCS 2016
Parece que el efecto de la siguiente línea de tratamiento no se ve influenciada por el uso de CDKis A verificar evolución en el resto de estudios
ESTUDIOS EN NEOADYUVANCIA
↓ of Ki 67 after neoadjuvant Endocrine Therapy as surrogate marker of long term benefit from adjuvant endocrine therapy


CCCA= Complete Cell Cycle Arrest = Ki 67 < 2,7%
1ry EP: CCCA C1D15 vs C1D1
1ry EP: Change in Ki67 at day 15
Amendment: last patienes resumed a 5th cycle of Palbo prior to surgery
Sherr C. NEJM 2016

Palbociclib enhanced cell cycle control over A monotherapy regardless of luminal subtype (A vs B) and PIK3CA status with activity observed across a broad range of clinicopathological and mutation profiles. Ki67 recovery at surgery following palbociclib washout was suppressed by cycle 5 palbociclib. Resistance was associated with non-luminal subtypes and persistent E2F-target gene expression.
N Patients 1ryEP CCCA RR
NeoPalAna Phase II
50 40 eval 39 completed
Pre/post II/III (no infl) Estratif PI3K mut/wt
CCCA C1D1 (A) vs C1D15 (A+P)
26% 87%
EF 80% US 41% No pCR
NeoMonarch Phase II R
224 A 74 A+AB 74 AB 76 Surgery 95
Post I/III Stratif PR, T
Change Ki67 2w CCCA
A 14,8% A+AB 66,1% AB 58,8%
EF 54% Rx 56 % 1 pCR (3%)

Toxicidades Neutropenia – Principal toxicidad de Palbociclib y Ribociclib. Generalmente sin fiebre y reversible
Ribociclib – Prolonga el intervalo QTc de una forma dosis dependiente ECG pre tto, iniciar si QTcF < 450 mseg, d14 y pre ciclo 2 y monitorizar electrolitos Evitar en pacientes de riesgo y uso concomintante con inh de CYP3A
Diarrea – toxicidad relevante con el abemaciclib. Uso profilactico y precoz de antidiarreicos y reduccion de dosis
Finn RS, et al. Breast Cancer Res 2016

Palbociclib (IBRANCE) FDA granted palbociclib accelerated approval in February 2015, in combination with letrozole for the treatment of HR + HER2-neg, advanced BC as initial endocrine based therapy in postmenopausal women. FDA granted palbociclib regular approval in February 2016, in combination with fulvestrant for the treatment of HR-+, HER2-neg advanced or metastatic breast cancer in women with disease progression following endocrine therapy. On March 31, 2017, the U.S. FDA granted regular approval to palbociclib (IBRANCE®, Pfizer Inc.) for the treatment of hormone receptor (HR) +, (HER2) negative advanced or metastatic breast cancer in combination with an AI as initial endocrine based therapy in postmenopausal women.
Ribociclib (Kisqali) On March 13, 2017, the U.S. FDA approved ribociclib (KISQALI, Novartis Pharmaceuticals Corp.), in combination with an AI as initial endocrine-based therapy for the treatment of postmenopausal women with (HR)-+, +(HER2)-negative advanced or metastatic breast cancer.
Palbociclib (IBRANCE) 16/09/2016 New treatment for breast cancer The European Medicines Agency (EMA) has recommended granting a marketing authorisation in the European Union (EU) for Ibrance for the treatment of women with locally advanced or metastatic breast cancer. IBRANCE is indicated for the treatment of (HR)-positive, (HER2)-negative locally advanced or metastatic breast cancer: - in combination with an aromatase inhibitor; - in combination with fulvestrant in women who have received prior endocrine therapy (see section 5.1). In pre- or perimenopausal women, the endocrine therapy should be combined with a luteinizing hormone-releasing hormone (LHRH) agonist.

Biomarcadores predictivos - Resistencia
• RH+, subtipo Luminal
• Rb funcional – (los luminales lo son)
• No otros marcadores (mut de PI3K, def p16, amplificación CCND1, mutaciones ESR1…)
• Resistencia – Rb: Pérdida de función como marcador de resistencia
– RBsig…
– Aumento de actividad CDK6
– Hiperactividad E-CDK2
– Otros
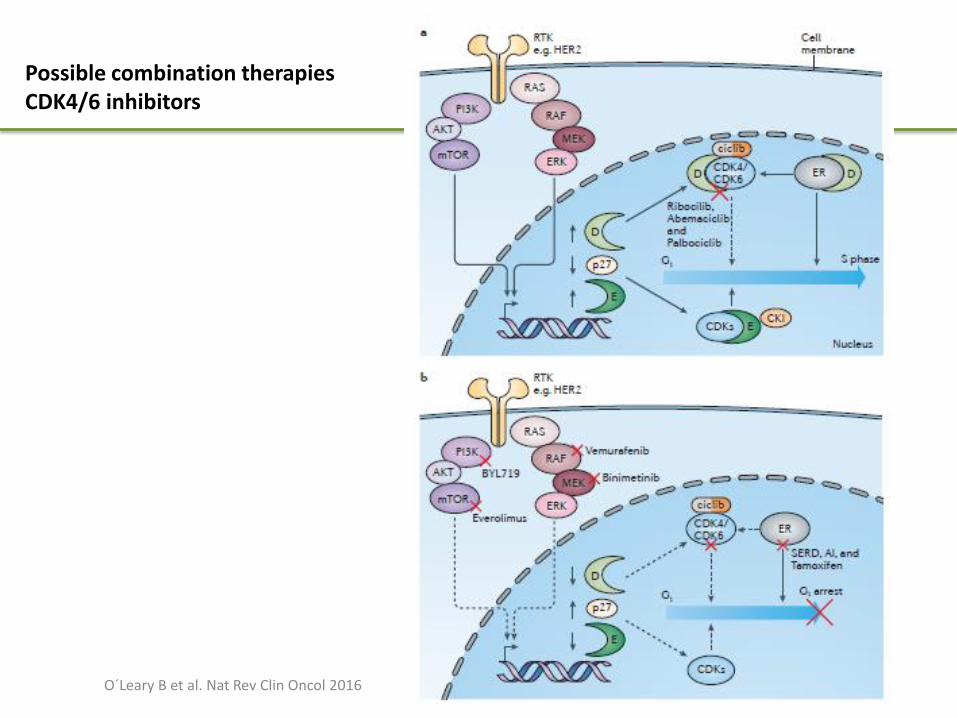
Possible combination therapies CDK4/6 inhibitors
O´Leary B et al. Nat Rev Clin Oncol 2016

Secuencia de terapia endocrina +/- terapias diana moduladoras de resistencia
Rugo H GEICAM 2017. Adapted from Jonhston- SABCS 2016
16m if pure 2nd line

Coste -eficacia
Mamiya H et el. Ann Oncol 2017

Conclusiones- … en el Ca de mama RH+HER2- avanzado…
• Los inhibidores de CDK/6 en combinación con hormonoterapia han demostrado eficacia en aumento de SLP en combinación con HT en 1ª y segunda línea en pacientes postmenopáusicas (real o farmacológica)
• Toxicidad manejable • Sin impacto evidente aun en la SG • Cuestiones
– Partner hormonal – Secuencia – Todas de inicio? – Efecto de clase? – Son intercambiables entre si?
Futuro
• Papel en neo/adyuvancia
• Mantenimiento de la inhibición cambiando el partner?
• Combinación con agentes a nivel de otras vías (inh de PI3K, inh HDAC… +/- HT revertir resistencias 1ª o 2ª)
• Papel en tumores HER2+ - esp Luminal-HER2+
• QT- ef antagónico?
• Necesidad de biomarcadores predictivos