Remodelacion Pulmonar en Tuberculosis

of 10
-
Upload
yoshie-parras -
Category
Documents
-
view
214 -
download
0
Transcript of Remodelacion Pulmonar en Tuberculosis
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
1/10
Remodeling in TB JID 2005:192 (1 October) 1201
M A J O R A R T I C L E
Lung Remodeling in Pulmonary Tuberculosis
Keertan Dheda,1,2,3 Helen Booth,3 Jim F. Huggett,1 Margaret A. Johnson,2 Alimuddin Zumla,1 and Graham A. W. Rook1
1Centre for Infectious Diseases and International Health, 2Department of Thoracic and HIV Medicine, Royal Free Hospital, and 3Department
of Thoracic Medicine, Middlesex Hospital, Royal Free and University College Medical School, London, United Kingdom
Tuberculosis is a global public health catastrophe responsible for 18 million cases of illness and 2 million
deaths annually. Pulmonary cavitation with cough-generated aerosol is the principle means of spread, and
lung remodeling (healed cavitation, fibrosis, and bronchiectasis) is a major cause of lung disability, surpassing
all other diffuse parenchymal lung diseases combined. Efficient granuloma turnover is mycobactericidal, and
extracellular matrix is disbanded without scarring. In many with progressive disease, however, there is dys-
regulated granuloma turnover, liquefactive necrosis, and pathological scarring. The pathological mechanisms
and the related immunological pathways underpinning these phenomena are reviewed in the present article.
Further studies are needed to identify and develop specific immunotherapeutic interventions that target im-munopathology, since they have the potential to substantially reduce spread.
The lung remodeling associated with pulmonary tuber-
culosis (TB) (healed cavitation, fibrosis, and distorted
architecture) has never been satisfactorily explained. This
is despite TB being an international publichealth priority
and despite cavitation, with associated tissue and lique-
factive necrosis, being the mechanism by which disease
transmission occurs. In addition to addressing the sig-
nificant morbidity associated with lung remodeling, in-
vestigations that can elucidate mechanisms and immu-
nological pathways relevant to tissue necrosis might lead
to strategies for interrupting aerosol-mediated transmis-
sion. Such knowledge can be incorporated into immu-
notherapeutic strategies aimed at halting person-to-per-
son spread of Mycobacterium tuberculosis.
Why do caseous and liquefactive necrosis occur? More-
over, why is fibrosis present in a disease characterized by
a potent interferon (IFN)g response, when this cytokine
generally opposes fibrosis [1]? In this review, we reeval-
uate current knowledge of the immunopathogenesis of
tissue necrosis and fibrosis. Peer-reviewed data for the
Received 16 December 2004; accepted 9 May 2005; electronically published
29 August 2005.
Potential conflicts of interest: none reported.
Financial support: British Lung Foundation (support to K.D.).
Reprints or correspondence: Dr. Keertan Dheda, Centre for Infectious Diseases
and International Health, Royal Free and University College Medical School, 46
Cleveland St., London W1T 4JF, United Kingdom ([email protected]).
The Journal of Infectious Diseases 2005;192:120110
2005 by the Infectious Diseases Society of America. All rights reserved.
0022-1899/2005/19207-0012$15.00
present article were identified by searches of the Medline
and PubMed databases, up to and including October
2004, in all languages, by use of the search terms tu-
berculosis and remodeling, cavitation, fibrosis,
immunopathology, extracellular matrix, protease,
or necrosis. Other sources were the references cited in
retrieved articles and referenced textbooks.
DEFINITIONS
In asthma and chronic obstructive pulmonary dis-
ease, remodeling refers to anatomical and structural
changes that are not easily reversible (laying down of
extracellular matrix [ECM]), in contrast to reversible
changes, such as edema and cellular infiltration) [2, 3].
In this review, we have extended the term remodeling
to include residual cavitation, lung fibrosis or scarring,
distortion of lung architecture leading to volume loss,
and tuberculous bronchiectasis, all of which represent
an inappropriate response to lung injury. An appro-priate response occurs, for example, when granuloma
formation occurs in a coordinated fashion, followed by
disbanding of the granuloma, dissolution of ECM, and
return to normal tissue architecture. Fibrosis implies
a structural alteration, with laying down of collagenous
ECM by fibroblasts and other cell types. The fibrosis
may be interstitial; occur as a capsule around cavities;
be bandlike, with distortion of the lung architecture;
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
2/10
1202 JID 2005:192 (1 October) Dheda et al.
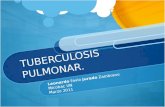
Figure 1. Principle cell types and cytokines involved in competent granuloma formation. NK T (NKT) cells, CD4+ T cells, CD8+ T cells, and gd
T cells produce type 1 cytokines that activate macrophages, which are mycobactericidal. Granulocytes (not shown) may be important in early granuloma
formation. Mycobacteria (rods) may be present within cells or extracellularly. Mycobacterial killing can occur by macrophage apoptosis, cytotoxic T
cell lysis (jagged arrow), or directly through granulysin (star)mediated destruction. Tumor necrosis factor (TNF)a is a likely requisite for macrophage
mycobactericidal activity, necrosis, and formation of the fibrous capsule. Cellular recruitment into the granuloma is facilitated by a chemokine gradient.
IFN-g, interferon-g; TGF-b, transforming growth factorb.
or be a combination of these. The term tissue necrosis en-
compasses both caseous and liquefactive necrosis.
CLINICAL ASPECTS
Cavitation into airways, with cough-induced aerosol genera-
tion, is the principle method by which TB is spread. Untreated,
there is a fatal outcome in 50% of individuals [4]. Despite che-
motherapy, however, there may be widespread lung destruction
with significant associated mortality [5]. Alternatively, subse-
quent healing can result in extensive fibrosis, traction bronchi-
ectasis [6, 7], and bronchostenosis [8], all of which may result
in volume loss, a restrictive defect during pulmonary function
testing [9, 10], and increased morbidity. Cavitation may erode
blood vessels, and bronchiectasis may cause significanthemopty-
sis [8, 11]. Poor drug penetration into cavities and fibrocaseousfoci, which are immunologically sealed off, may facilitate la-
tency and selection of drug resistance. Residual distortion of the
lung architecture depends on the degree to which the connective-
tissue matrix of a granuloma is degraded and removed. The key
question is what determines whether a granuloma resolves com-
pletely without scarring or whether liquefactive necrosis and/or
extensive scarring occurs.
EFFICIENT GRANULOMA FORMATION
AND DISSOLUTION
The first cell types encountered by inhaled mycobacteria are
the alveolar macrophages; phagocytosis is mediated by varioushost receptors [12, 13]. Lung gd T cells, NK T cells, and gran-
ulocytes are important early arrivals that precede the second
wave of expanded, IFN-g and tumor necrosis factor (TNF)
aproducing effector T cell populations [1416]. Collectively,
these cells initiate a chemokine and cytokine cascade that at-
tracts other macrophages and, later, T cells to the site of in-
fection [17] (figure 1). There is plasma exudation, and a fibrin
clot is formed [18, 19]. Macrophage aggregation to form an
early granuloma core is mediated by hyaluronic acid [20],
which binds to macrophages via CD44 [21]. Detailed histo-
logical analyses of developing granulomata in the rabbit model
[22] led to the view that macrophage activation driven by cell-
mediated immunity is followed by destruction of the same
macrophages, which then accumulate as caseous necrosis, and
is often associated with death of the contained bacilli. An al-
ternative view is that granulocytes are early arrivals that medi-
ate the cell lysis that forms the core of developing caseous
necrosis [16, 23, 24]. Recent pathological studies of granulomas
in tuberculous human lungs indicate that the peripheral lym-
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
3/10
Remodeling in TB JID 2005:192 (1 October) 1203
phocyte zones of the granuloma have secondary lymphoid fol-
licles analogous to those found in lymph nodes [16].
Macrophages and other cell types, such as fibroblasts, endo-
thelial cells, and neutrophils, also produce proteases (metal-
loproteinases [collagenase, gelatinase, and stromelysin]; the ly-
sosomal proteinases [cathepsins]; and the plasminogen/plas-
min system and its activator, urokinase]). Such enzymes may
facilitate granuloma formation by mediating antigen process-ing, removal of ECM and cellular debris, and processing of
cytokines and hormones [25]. They are tightly regulated at
multiple levels, including transcription, proenzyme formation,
and signaling control, as well as by tissue inhibitors of metal-
loproteinases (TIMPs) [26, 27].
Within the granuloma, both T cells and macrophages secrete
TNF-a and lymphotoxin a3. Not only is TNF-a crucial for
host defense [2832], but it also facilitates the structural in-
tegrity of the granuloma by mediating the formation of the en-
capsulating fibrous wall [33], together with transforming growth
factor (TGF)b [34, 35]. Macrophages also secrete insulin-like
growth factor (GF)1, fibroblast GF, fibronectin, and platelet-derived GF [36, 37]. These GFs are chemotactic and support
macrophage proliferation and, hence, the laying down of ECM
comprising collagen, fibronectins, and glycosaminoglycans [38
40]. Caseous necrosiswhich occurs at 23 weeks in the
rabbit model [22]and its associated low oxygen content cre-
ate unfavorable conditions for mycobacterial multiplication
[41]. This, together with macrophage activation and CD3+ ef-
fector cell mechanisms, culminates in mycobacterial steriliza-
tion. It was shown in 1927 that healed primary lesions are usu-
ally sterile within 5 years, although latent bacilli may persist in
other, superficially normal, parts of the lung [42, 43].
Controlled dissolution of the granuloma follows mycobac-
terial containment, although this may be incomplete if there
has been massive production of caseum. Proteases cleave com-
ponents of the ECM [26]. Macrophages phagocytose the part-
ly degraded ECM components, which are terminally degraded
within the lysosome or transported out of the lung [4446].
Minor residual scarring may remain.
DYSREGULATED GRANULOMA TURNOVER
AND LIQUEFACTIVE NECROSIS
In a significant minority of infected individualsthose with pro-
gressive primary and reactivation diseasethere is progressive
disease and liquefactive necrosis. This forms an ideal culture
medium for mycobacteria; they multiply extracellularly to large
numbers [47], since macrophages are unable to survive in ne-
crotic tissue, partly because of its toxic fatty acid content [41].
The proteolytic enzymes [48] compromise the integrity of the
fibrous granuloma capsule. Caseous material may discharge in-
to surrounding blood vessels and airways, thereby facilitating
systemic dissemination, and to the outside environment via
cough-induced respiratory droplets. The cavity often has an
external zone of collagen, internal to which is a zone of gran-
ulation tissue rich in fibroblasts, inflammatory cells, and cap-
illaries [47]. The role of vasculopathy as a primary event in the
facilitation of cavitation is unclear. With antimicrobial therapy,
the cavities may persist as fibrotic walled structures lined by
metaplastic squamous epithelium or as emphysematous bullae,or they may become distorted from without by traction fibrosis
[47].
Although the exact mechanisms of liquefaction are unknown,
the available data suggest that dysregulated proteolysis, direct
mycobacterial toxicity, the Koch phenomenon [49] and Shwartz-
man reaction [50], and host effector cells and cytokines are key
players (figure 2). These concepts are further discussed below.
Dysregulated Proteolysis and Direct Mycobacterial Toxicity
A variety of host proteases are up-regulated in mycobacteri-al infection [48, 5153], and dysregulation of protease control
mechanisms is likely to mediate proteolysis of structural com-
ponents of the lung [54]. Cytokines such as TNF-a and in-
terleukin (IL)1b can up-regulate proteases [5557] in mouse
and human monocytes in response to mycobacterial proteins
[58], and lipoarabinomannan induces collagenases in myeloid
cells [54]. Macrophage destruction by cytotoxic T cells and the
release of lysosomal contents are likely to play a significant role
in tissue destruction and may explain some of the necrosis in
the central part of the granuloma where macrophages pre-
dominate. Granulocytes may be important facilitators of early
necrosis [16, 23]. As discussed below, local tissue damage willbe more likely if the macrophages undergo necrosis rather than
apoptosis. Although thought to be less important, mycobacte-
ria themselves may produce endopeptidases [25] or other pro-
necrotic virulence factors. Recently, however, a polyketide tox-
ic factor, isolated from M. ulcerans, has been shown to have
cytopathic properties and produced necrotic cutaneous le-
sions in guinea pigs [59]. Since the M. tuberculosis genome
contains many polyketide synthesis genes [60], it is reasonable
to speculate that this toxin may represent one of a family of
virulence factors associated with immunopathology in myco-
bacterial diseases. Similarly, the secreted protein early secreted
antigenic target 6 kDa (ESAT-6) is a virulence factor for M.
tuberculosis and appears to cause lysis of lung epithelial cells
and to facilitate local spread [61]. Its contribution to caseation
is not known. Certain deletional mutants of M. tuberculosis
have an unchanged ability to proliferate within the host but
induce much less immunopathology, suggesting that myco-
bacterial virulence factors actively induce tissue-damaging cell-
mediated immune responses [62, 63].
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
4/10
1204 JID 2005:192 (1 October) Dheda et al.
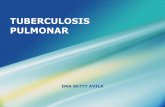
Figure 2. Factors that might contribute to dysregulated granuloma formation. Mycobacterial antigens mediate uncoupled protease metabolism ac-
tivity, apoptosis, the Koch phenomenon, and, perhaps, cell lysis mediated by early secreted antigenic target 6 kDa (ESAT-6) and induce the release
of cytokines (tumor necrosis factor [TNF]a, mixed Th1/Th2, and transforming growth factor [TGF]b), which collectively facilitate liquefactive necrosis
and deranged extracellular matrix (ECM) turnover. Mycobacteria (solid capsules) multiply extracellularly, compromise the fibrous granuloma capsule,
and may discharge into a bronchial lumen or blood vessel.
The Koch Phenomenon and Shwartzman Reaction
Koch [49] showed that tuberculous guinea pigs developed ne-
crosis locally and at distant sites of infection after rechallenge
with tuberculin. High tuberculin reactivity occurs in experi-
mental animals with liquefaction [64]. Similarly, the tubercu-
lin test is frequently necrotic in humans with TB but not in
healthy bacille Calmette-Guerin (BCG)vaccinated individuals
[47]. More recently, an elegant study showed that M. tuber-
culosisinfected mice developed increased lung inflammation
and elevated TNF-a levels when rechallenged with mycobac-
terial antigens [65]. Moreover, when prophylactic-vaccine can-
didates are tested for therapeutic effects in mice with TB, they
develop increased immunopathology [66] and classical Koch
reactions characterized by cellular necrosis within granuloma-
ta [67]. One explanation may be the systemic Shwartzman re-
action [50], which referred originally to cutaneous necrosis at a
site of a previous endotoxin injection after intravenous injec-
tion of lipopolysaccharide (LPS). The concept is that the initial
skin inflammation causes endothelial activation and accumula-
tion of inflammatory cells. Then, a subsequent systemic cyto-
kine-inducing signal administered 24 h later preferentially
triggers necrosis in the prepared skin site. Indeed, M. tuber-
culosisinfected C57BL/6 mice, which do not conventionally
develop necrosis in this model, develop caseous necrosis after
inoculation with LPS [68]. Moreover, LPS shares many physical
properties and biological functions with a major mycobacterial
antigen, lipoarabinomannan [69].
Host Cytokines and Effector Mechanisms
Necrosis and cavitation can occur in response to nonviable,
nontoxic components of mycobacteria [48, 64, 70]. This sug-
gests that host cytokines and enzymes are responsible for the
necrosis. Although the precise mechanisms inducing progres-
sion from controlled protease release and granuloma forma-
tion to dysregulated protease production with liquefactive ne-
crosis are unknown, a likely facilitator is TNF-a.
TNF-a. Although TNF-a is essential for immunity to TB,
in progressive disease TNF-a is associated with fever and wast-
ing [7173] and correlates with disease activity and immuno-
pathology [29, 7477]. Cells containing M. tuberculosisare ren-
dered exquisitely sensitive to killing by TNF-a [75, 78]. As out-
lined above, TNF-a can up-regulate metalloproteinases and
urokinase and thereby facilitate proteolysis of structural lung
elements. However, under what conditions is the protective
TNF-a molecule toxic? Data, as outlined below, support a
possible role for Th2 cytokines in such toxicity.
Th1 and Th2 cytokines. Recent data have convincingly
demonstrated the presence of Th2 cytokines in human TB [79].
Th2 cells may mediate local tissue damage that is IL-4 depen-
dent [80]. In M. tuberculosisinfected mice, susceptibility to the
toxic effects of TNF-a injected into the footpads coincided
temporally with the emergence of Th2 cytokines in the lungs
[81]. IL-4 may also regulate TNF-amediated enteropathy inTrichinella spiralis infection [82], and necrosis in a schistoso-
miasis model coincides precisely with the superimposition of
Th2 response on an existing Th1 pattern [83]. Mouse (BALB/
c) models of TB showed high IFN-g levels early during infec-
tion, with increased levels of IL-4 during the chronic phase of
infection, which was characterized by progressive fibrosis and
necrosis [84, 85]. The Th2 response may exacerbate tissue dam-
age by enhancing the pathological effect of TNF-a [81]. More
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
5/10
Remodeling in TB JID 2005:192 (1 October) 1205
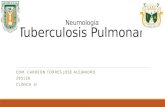
Figure 3. The roles of the subversive Th2-like component of the immune response in progressive human tuberculosis. This Th2-like interleukin
(IL)4 response, modulated by IL-4d2, may be primed by environmental mycobacteria and helminths and is most striking in developing countries [92,
93]. After exposure to Mycobacterium tuberculosis, certain cell-wall components and protein antigens [9497] are then able to drive and enhance
this IL-4 response, which may contribute to deactivation of macrophages, as well as to necrosis and fibrosis. TGF-b, transforming growth factor b;
TNF-a, tumor necrosis factor a.
recent evidence, from IL-4 gene knockout experiments in BALB/
c mice, showed an absence of TNF-amediated toxicity after
TNF-a challenge in the absence of IL-4 [86]. Collectively, these
murine data suggest that, under the influence of superimposed
Th2 cytokines, TNF-a is toxic in dominantly Th1-mediated le-
sions. It is not unreasonable to suggest that a similar mechanism
operates in humans. Studies of lavage fluid from patients with
TB show the presence of IL-4producing Th2 lymphocyte sub-sets in those with cavitary TB [87] and the presence of a Th1
cytokine profile in those with noncavitary disease [74]. Simi-
larly, expression of IL-4 in peripheral blood lymphocytes cor-
relates with cavitary disease [88].
In other murine knockout models of immunopathology in-
duced by mycobacteria, g/d T cells [89], a/b-positive T cells,
IL-12, IFN-g, and TNF-a [90, 91] also seem to be essential for
necrosis of granulomata (figure 3). It has been suggested that
caseous necrosis is a protective mechanism to reduce the log-
arithmic growth of the organisms [47]. However, it is apoptosis
rather than necrosis that destroys M. tuberculosis (see below),
so it is intriguing to speculate that M. tuberculosishas evolvedcomponents that exploit the hosts tissue-damaging protective
responses by driving a Th2 response and necrosis. It is inter-
esting that particularly virulent Beijing strains ofM. tuberculosis
cause human monocytes to express IL-4 and IL-13 [94].
Apoptosis. Caseation is a mixture of necrosis and apopto-
sis. Large numbers of apoptotic T cells and macrophages are
seen in caseous foci [98]. Immunohistochemical analysis and
in situ hybridization have shown that macrophages surround-
ing caseous foci are negative for the antiapoptotic protein bcl2
but positive for the proapoptotic protein bax, whereas the as-
sociated T cells express IFN-g and FasL [98]. Apoptosis of
macrophages may be beneficial to the host. Both in mice [99]
and in humans [100], CD8+ cytotoxic T cells that use the gran-
ule-mediated pathway to induce apoptosis (as opposed to the
FasFas ligand pathway) lead to killing of the contained my-
cobacteria too. The role of the granule contents, particularly
granulysin, has been reviewed [101]. Apoptosis induced by ATP
[102, 103], TNF-a independent of IFN-g [104], Fas ligand
[105], and hydrogen peroxide [106] all promote killing of vir-
ulent M. tuberculosiswithin macrophages, whereas the necrotic
mode of death does not [105, 107]. Moreover, M. tuberculosishas mechanisms that tend to inhibit apoptosis. Mannose-cap-
ped lipoarabinomannan (Man-LAM) stimulates phosphoryla-
tion of Bad, a proapoptotic protein, and so inhibits apoptosis
[108]. Another group has shown that Man-LAM inhibits ap-
optosis by a mechanism involving calcium-dependent signal-
ing [109]. Recently, cathepsins have been shown to modulate
apoptosis in human pulmonary epithelial cells [110], although
their role in TB has not been investigated. It is, therefore, pos-
sible that the material that accumulates as caseum is, in fact,
a product of inappropriate necrosis. Apoptotic cells are usu-
ally removed by surrounding cells with minimal inflammatory
consequences, whereas necrotic cells accumulate. However, itis also possible that, when a sufficient percentage of the cells
are undergoing apoptosis, the normal clearance mechanism
fails, and apoptotic cells can themselves contribute to caseum.
FIBROSIS IN TB
TNF-a, TGF-b, and the pathogenesis of fibrosis. Extensive
deposition of ECM occurs in the guinea pig model of TB [111].
Available data suggest that TGF-b, together with TNF-a, plays
a key role in the formation of the fibrous wall that encapsu-
lates the tuberculous granuloma [3335]. The importance of
TGF-b with respect to pulmonary fibrosis has been established
in human [38, 112] and animal [113, 114] models. Although
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
6/10
1206 JID 2005:192 (1 October) Dheda et al.
the exact signaling pathways that drive fibroblasts to lay down
ECM and macrophages to dissolve ECM are poorly under-
stood, it is reasonable to speculate that TGF-b may contribute
to the dysregulation of ECM turnover in TB. Indeed, TGF-b
may also perpetuate fibrogenesis by inhibiting apoptosis of
fibroblasts [115] and mediating localized production of inhib-
itors of TIMP [116]. However, it seems that TGF-b, although
necessary, is not sufficient for fibrosis. The importance of othermolecules, such as TNF-a, in lung fibrosis is illustrated by
models of bleomycin and hypersensitivity pneumonitis, in
which antiTNF-a antibodies ameliorate lung fibrosis [117,
118]. The role of other cell typessuch as alveolar epithelial
cells, which can harbor M. tuberculosis [42] and can be an im-
portant source of cytokines and GFs in idiopathic pulmonary
fibrosis [119]merits further investigation.
Two paradoxes immediately arise. The first is the presence
of increased ECM at the periphery of the granuloma but dis-
solution of ECM in the central part of the granuloma. Possible
explanations include a cytokine gradient within the granuloma
[120], including low IFN-g levels in the central macrophage-
dominant part of the granuloma or selective binding of cyto-
kines to glycosaminoglycans in different parts of the granuloma
[121]. Therefore, in the center of the granuloma, high TNF-a
concentrations, protease activity, and lysis of infected macro-
phages predominate, whereas, in the periphery, TGF-b activity
and fibroblast activation predominate.
The second paradox is the presence of fibrosis where there
are potent IFN-g responses, which down-regulate TGF-b and
production of collagen by fibroblasts [122, 123]. The answer
may lie in the significant Th2 response that develops parallel
to and within the framework of a Th1 response.Role of Th2 cytokines in fibrosis. IL-4 and IL-13 are pro-
fibrotic and enhance collagen production by fibroblasts [123].
Mice, when infected with saprophytic mycobacteria, only de-
velop peribronchial and interstitial fibrosis when primed for IL-
4 [84]. Even a single epitope (16 aa) inducing a Th2 response
can drive fibrosis in a murine model of TB [124].
In all human diseases characterized by marked pulmonary
fibrosis (systemic sclerosis, idiopathic pulmonary fibrosis, ra-
diation-induced pulmonary fibrosis, and chronic lung allograft
rejection; reviewed in [125]), there is expression of type 2 cy-
tokines. The same is true in the bleomycin murine model [125]
and in schistosomiasis, in which fibrosis and tissue remodel-ing do not occur if induction of type 2 cytokines by the ova
is blocked by preimmunization with ova plus IL-12 [126]. No-
tably, there are no data on cytokine profiles in the late stages
of fibrotic sarcoidosis [127]. These observations have led to the
type 2 cytokine hypothesis of fibrosis [125]. This paradigm
implies an initial Th1-type response to antigenic challenge, fol-
lowed by a Th2 response that seeks to wall off, or isolate, a
persistent antigen from the host [128130]. M. tuberculosismay
be exploiting this host response to remain immunologically
sealed off in fibrocaseous foci.
The Th2 phenotype causes fibroblast activation and collagen
deposition in human [131, 132] and animal [114, 133] models.
Collagen synthesis in granulomata is stimulated by Th2 cyto-
kines (IL-4, IL-13, and IL-4d2) and reciprocally inhibited by
Th1 cytokines such as IFN-g and IL-12 [1, 126]. Moreover,
granulomatous inflammation and fibrosis are significantly re-duced in Stat6/ mice [134]; IL-4 and IL-13 are the major
activators of Stat6. Fibrosis is particularly pronounced in mice
overexpressing IL-13 [125]. This cytokine, like IL-4 and IL-4d2
[135], activates fibroblasts and promotes collagen formation.
However, IL-13 also drives expression and activation of TGF-
b [125]. Significantly, the increase in expression of type 2 cy-
tokines in human TB extends to IL-13, which, like IL-4 and
IL-4d2, is increased 80100-fold [136, 137].
Smoking can reactivate TB, probably because nicotine switches
off secretion of TNF-a by macrophages, leaving IL-10 secretion
unchanged [138]. Similarly, TNF-amediated fibrotic lung dis-
eases like sarcoidosis and extrinsic allergic alveolitis [139, 140]are less common in smokers, and smoking improves survival in
a Th2-type fibrotic lung condition, idiopathic pulmonary fibro-
sis [141, 142]. The common denominator facilitating fibrosis in
all of these disorders might be the presence of a Th2 cytokine
component acting synergistically with TNF-a.
IL-4 or IL-4d2 from CD8+ T cells and their role in fibrosis.
In systemic sclerosis, Th2 cytokine expression is associated with
pulmonary fibrosis [135]. Interestingly, in several patients, the
IL-4, made mostly by the CD8+ T cells, was in fact not IL-
4 at all but rather IL-4d2, raising the likelihood that the CD8+
T cells making IL-4 in TB reported by van Crevel et al. might
be really making IL-4d2 (van Crevel et al. used reagents that
do not distinguish between the 2 cytokines [88]). IL-4d2 is
antagonistic to IL-4 with regard to lymphocyte function [143,
144], but it is an agonist on fibroblasts [135].
ARE THERE ANTIGENS THAT PREFERENTIALLY
DRIVE NECROSIS AND FIBROSIS?
IMPLICATIONS FOR IMMUNOTHERAPY
It is not yet clear whether there are antigens that preferentially
drive Th2, or whether M. tuberculosis merely contains Th2
adjuvant activity. The recent discovery that virulent Beijing
strains contain lipids that cause human monocytes to make
IL-4 and IL-13 suggests that adjuvanticity is part of the mech-
anism [94]. Similarly, dendritic cells derived from BCG-in-
fected precursors can drive a Th2-like response [145]. Nev-
ertheless, there does seem to be some antigenic specificity to
the Th2 response. ESAT-6 fails to drive IL-4 production [146],
but certain epitopes from within the 16-kDa heat-shock pro-
tein do so [95]. Identification of the antigens or epitopes that
drive IL-4 production will allow design of vaccines that sup-
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
7/10
Remodeling in TB JID 2005:192 (1 October) 1207
press the unwanted Th2 component [79]. Agents like M. vac-
cae, which attenuate Th2 responses [147, 148], have demon-
strated the ability to modulate lung remodeling and radiographic
absorbance in both drug-sensitive and resistant TB [149, 150];
clinical trials using multiple dose regimes are currently under
way [151].
In conclusion, further research into the genetic, molecular,
immunological, and cellular pathways that drive cavitation andfibrosis are required. This could yield clinical benefit and has
the potential to interrupt transmission. For instance, vaccines
that target immunopathology (either host responses or bacte-
rial virulence factors), even if they are not completely protec-
tive, may have the ability to reduce global disease burden by
minimizing cavitation and interrupting transmission. Like the
antiTNF-a agents [152154], other immunotherapeutic mo-
dalities could target pathways relating to cytokine signaling, ap-
optosis, protease activity,and ECM turnover. However, such goals
are tenable only if adequate funding is committed by government
agencies, the pharmaceutical industry,and internationalcharities.
Moreover, there will have to be a global organizational structurecommitted to achieving such goals.
References
1. Sempowski GD, Derdak S, Phipps RP. Interleukin-4 and interferon-
gamma discordantly regulate collagen biosynthesis by functionally
distinct lung fibroblast subsets. J Cell Physiol 1996; 167:2906.
2. Caughey GH. Chairmans summary: mechanisms of airway remod-
eling. Am J Respir Crit Care Med 2001; 164:S267.
3. Jeffery PK. Remodeling in asthma and chronic obstructive lung dis-
ease. Am J Respir Crit Care Med 2001; 164:S2838.
4. Smith PG, Moss AR. Epidemiology of tuberculosis. In: Bloom BR,
ed. Tuberculosis: pathogenesis, protection, and control. 1st ed. Wash-ington DC, American Society for Microbiology, 1994:4759.
5. Bobrowitz ID. The destroyed tuberculous lung. Scand J Respir Dis
1974; 55:828.
6. Curtis JK. The significance of bronchiectasis associated with pulmonary
tuberculosis. Am J Med 1957; 22:894903.
7. Rosenzweig DY. The role of tuberculosis and other forms of bron-
chopulmonary necrosis in the pathogenesis of bronchiectasis. Am Rev
Respir Dis 1966; 93:76985.
8. Kim YH, Kim HT, Lee KS, Uh ST, Cung YT, Park CS. Serial fiberoptic
bronchoscopic observations of endobronchial tuberculosis before and
early after antituberulosis chemotherapy. Chest 1993; 103:6737.
9. Lopez-Majano V. Ventilation and transfer of gases in pulmonary tu-
berculosis. Respiration 1973; 30:4863.
10. Skoogh BE. Lung mechanics in pulmonary tuberculosis. I. Static lung
volumes. Scand J Respir Dis 1973; 54:14856.
11. Thompson JR. Mechanisms of fatal pulmonary hemorrhage in tu-
berculosis. Am J Surg 1955; 89:63744.
12. Ernst JD. Macrophage receptors for Mycobacterium tuberculosis. Infect
Immun 1998; 66:127781.
13. Heldwein KA, Fenton MJ. The role of Toll-like receptors in immunity
against mycobacterial infection. Microbes Infect 2002; 4:93744.
14. Apostolou I, Takahama Y, Belmant C, et al. Murine natural killer T
(NKT) cells [correction of natural killer cells] contribute to the gran-
ulomatous reaction caused by mycobacterial cell walls. Proc Natl Acad
Sci USA 1999; 96:51416.
15. Kaufmann SH. g/d and other unconventional T lymphocytes: what
do they see and what do they do? Proc Natl Acad Sci USA 1996;93:
22729.
16. Ulrichs T, Kosmiadi GA, Trusov V, et al. Human tuberculous gran-
ulomas induce peripheral lymphoid follicle-like structures to orches-
trate local host defence in the lung. J Pathol 2004; 204:21728.
17. Ulrichs T, Kaufmann SHE. Cell-mediated immune response. In: Rom
WN, Garay SM, eds. Tuberculosis. 2nd ed. Philadelphia: Lippincott
Williams & Wilkins, 2004:25162.
18. Behling CA, Perez RL, Kidd MR, Staton GW Jr, Hunter RL. Induction
of pulmonary granulomas, macrophage procoagulant activity, and
tumor necrosis factor-alpha by trehalose glycolipids. Ann Clin Lab
Sci 1993; 23:25666.
19. Perez RL, Roman J, Staton GW Jr, Hunter RL. Extravascular coag-
ulation and fibrinolysis in murine lung inflammation induced by the
mycobacterial cord factor trehalose-6,6-dimycolate. Am J Respir Crit
Care Med 1994; 149:5108.
20. Love SH, Shannon BT, Myrvik QN, Lynn WS. Characterization of
macrophage agglutinating factor as a hyaluronic acid-protein com-
plex. J Reticuloendothel Soc 1979; 25:26982.
21. Green SJ, Tarone G, Underhill CB. Aggregation of macrophages and
fibroblasts is inhibited by a monoclonal antibody to the hyaluronate
receptor. Exp Cell Res 1988; 178:22432.
22. Lurie MB, Zappasodi P, Tickner C. On the nature of genetic resistance
to tuberculosis in the light of the host-parasite relationshipsin natively
resistant and susceptible rabbits. Am Rev Tuberc 1955; 72:297329.
23. Seiler P, Aichele P, Bandermann S, et al. Early granuloma formationafter aerosol Mycobacterium tuberculosisinfection is regulated by neu-
trophils via CXCR3-signaling chemokines. Eur J Immunol 2003;33:
267686.
24. Turner OC, Basaraba RJ, Orme IM. Immunopathogenesis of pulmonary
granulomas in the guinea pig after infection with Mycobacterium tu-
berculosis. Infect Immun 2003; 71:86471.
25. Munger, JS, Chapman HA Jr. Tissue destruction by proteases. In: Rom
WN, Garay SM, eds. Tuberculosis. 2nd ed. Philadelphia: Lippincott
Williams & Wilkins, 2004:35362.
26. Chapman HA Jr. Role of enzyme receptors and inhibitors in regulating
proteolytic activities of macrophages. Ann N Y Acad Sci 1991;624:
8796.
27. Mauviel A. Cytokine regulation of metalloproteinase gene expression.
J Cell Biochem 1993; 53:28895.
28. Appelberg R. Protective role of interferon gamma, tumor necrosisfactor alpha and interleukin-6 in Mycobacterium tuberculosis and M.
avium infections. Immunobiology 1994; 191:5205.
29. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with in-
fliximab, a tumor necrosis factor a-neutralizing agent. N Engl J Med
2001; 345:1098104.
30. Mohan VP, Scanga CA, Yu K, et al. Effects of tumor necrosis factor
alpha on host immune response in chronic persistent tuberculosis:
possible role for limiting pathology. Infect Immun 2001; 69:184755.
31. Ogawa T, Uchida H, Kusumoto Y, Mori Y, Yamamura Y, Hamada S.
Increase in tumor necrosis factor alpha- and interleukin-6-secreting
cells in peripheral blood mononuclear cells from subjects infected
with Mycobacterium tuberculosis. Infect Immun 1991; 59:30215.
32. Roach DR, Briscoe H, Saunders B, France MP, Riminton S, Britton
WJ. Secreted lymphotoxin-alpha is essential for the control of an
intracellular bacterial infection. J Exp Med 2001; 193:23946.
33. Lukacs NW, Chensue SW, Strieter RM, Warmington K, Kunkel SL.
Inflammatory granuloma formation is mediated by TNF-a-inducible
intercellular adhesion molecule-1. J Immunol 1994; 152:58839.
34. Aung H, Toossi Z, McKenna SM, et al. Expression of transforming
growth factor-b but not tumor necrosis factor-a, interferon-g, and
interleukin-4 in granulomatous lung lesions in tuberculosis. Tuber
Lung Dis 2000; 80:617.
35. Marshall BG, Wangoo A, Cook HT, Shaw RJ. Increased inflammatory
cytokines and new collagen formation in cutaneous tuberculosis and
sarcoidosis. Thorax 1996; 51:125361.
36. Wangoo A, Taylor IK, Haynes AR, Shaw RJ. Up-regulation of alveolar
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
8/10
1208 JID 2005:192 (1 October) Dheda et al.
macrophage platelet-derived growth factor-B (PDGF-B) mRNA by
interferon-gamma from Mycobacterium tuberculosis antigen (PPD)-
stimulated lymphocytes. Clin Exp Immunol 1993; 94:4350.
37. Yeager H Jr, Azumi N, Underhill CB. Fibrosis: the formation of the
granuloma matrix. In: Rom WN, Garay SM, eds. Tuberculosis. 2nd
ed. Philadelphia: Lippincott Williams & Wilkins, 2004:36372.
38. Limper AH, Colby TV, Sanders MS, Asakura S, Roche PC, DeRemee
RA. Immunohistochemical localization of transforming growth fac-
tor-beta 1 in the nonnecrotizing granulomas of pulmonary sarcoid-
osis. Am J Respir Crit Care Med 1994; 149:197204.
39. Mornex JF, Leroux C, Greenland T, Ecochard D. From granuloma to
fibrosis in interstitial lung diseases: molecular and cellular interactions.
Eur Respir J 1994; 7:77985.
40. Peyrol S, Takiya C, Cordier JF, Grimaud JA. Organization of the con-
nective matrix of the sarcoid granuloma: evolution and cell-matrix in-
teractions. Ann N Y Acad Sci 1986; 465:26885.
41. Hemsworth GR, Kochan I. Secretion of antimycobacterial fatty acids
by normal and activated macrophages. Infect Immun 1978; 19:1707.
42. Hernandez-Pando R, Jeyanathan M, Mengistu G, et al. Persistence of
DNA from Mycobacterium tuberculosis in superficially normal lung
tissue during latent infection. Lancet 2000; 356:21338.
43. Opie EL, Aronson JD. Tubercle bacilli in latent tuberculosis lesions
and in lung tissue without tuberculous lesions. Arch Pathol 1927; 4:
121.
44. Culty M, OMara TE, Underhill CB, Yeager H Jr, Swartz RP. Hyalu-
ronan receptor (CD44) expression and function in human peripheralblood monocytes and alveolar macrophages. J Leukoc Biol 1994;56:
60511.
45. Parakkal PF. Involvement of macrophages in collagen resorption. J
Cell Biol 1969; 41:34554.
46. Werb Z, Bainton DF, Jones PA. Degradation of connective tissue ma-
trices by macrophages. III. Morphological and biochemical studies on
extracellular, pericellular, and intracellular events in matrix proteolysis
by macrophages in culture. J Exp Med 1980; 152:153753.
47. Dannenburg AM, Rook GAW. Pathogenesis of pulmonary tubercu-
losis: an interplay of tissue-damaging and macrophage-activatingim-
mune responsesdual mechanisms that control bacillary multipli-
cation. In: Bloom BR, ed. Tuberculosis: pathogenesis, protection, and
control. 1st ed. Washington DC, American Society for Microbiology,
1994:45983.
48. Dannenberg AM Jr, Sugimoto M. Liquefaction of caseous foci in tu-berculosis. Am Rev Respir Dis 1976; 113:2579.
49. Koch R. Fortsetzung uber ein Heilmittel gegen Tuberculose. Dtsch
Med Wochenschr 1989; 17:1012.
50. Rook GA, Al Attiyah R. Cytokines and the Koch phenomenon. Tu-
bercle 1991; 72:1320.
51. Rojas-Espinosa O, Dannenberg AM Jr, Sternberger LA, Tsuda T. The
role of cathepsin D in the pathogenesis of tuberculosis:a histochemical
study employing unlabeled antibodies and the peroxidase-antiperox-
idase complex. Am J Pathol 1974; 74:117.
52. Tsuda T, Dannenberg AM Jr, Ando M, Rojas-Espinosa O, Shima K.
Enzymes in tuberculous lesions hydrolyzing protein, hyaluronic acid
and chondroitin sulfate: a study of isolated macrophages and devel-
oping and healing rabbit BCG lesions with substrate film techniques;
the shift of enzyme pH optima towards neutrality in intact cells
and tissues. J Reticuloendothel Soc 1974; 16:22031.
53. Yagel S, Gallily R, Weiss DW. Effect of treatment with the MER fraction
of tubercle bacilli on hydrolytic lysosomal enzyme activity of mouse
peritoneal macrophages. Cell Immunol 1975; 19:3816.
54. Chang JC, Wysocki A, Tchou-Wong KM, Moskowitz N, Zhang Y,
Rom WN. Effect of Mycobacterium tuberculosis and its components
on macrophages and the release of matrix metalloproteinases. Tho-
rax 1996; 51:30611.
55. Schonthal A, Herrlich P, Rahmsdorf HJ, Ponta H. Requirement for
fos gene expression in the transcriptional activation of collagenase by
other oncogenes and phorbol esters. Cell 1988; 54:32534.
56. Gyetko MR, Shollenberger SB, Sitrin RG. Urokinase expression in mono-
nuclear phagocytes: cytokine-specific modulation by interferon-gamma
and tumor necrosis factor-alpha. J Leukoc Biol 1992; 51:25663.
57. Gyetko MR, Wilkinson CC, Sitrin RG. Monocyte urokinase expres-
sion: modulation by interleukins. J Leukoc Biol 1993; 53:598601.
58. Gordon S, Cohn ZA. Bacille Calmette-Guerin infection in the mouse:
regulation of macrophage plasminogen activator by T lymphocytes
and specific antigen. J Exp Med 1978; 147:117588.
59. George KM, Pascopella L, Welty DM, Small PL. A Mycobacterium ul-
cerans toxin, mycolactone, causes apoptosis in guinea pig ulcers and
tissue culture cells. Infect Immun 2000; 68:87783.60. Cole ST, Brosch R, Parkhill J, et al. Deciphering the biology ofMy-
cobacterium tuberculosisfrom the complete genome sequence. Nature
1998; 393:53744.
61. Hsu T, Hingley-Wilson SM, Chen B, et al. The primary mechanism
of attenuation of bacillus Calmette-Guerin is a loss of secreted lytic
function required for invasion of lung interstitial tissue. Proc Natl
Acad Sci USA 2003; 100:124205.
62. Steyn AJ, Collins DM, Hondalus MK, Jacobs WR Jr, Kawakami RP,
Bloom BR. Mycobacterium tuberculosis WhiB3 interacts with RpoV
to affect host survival but is dispensable for in vivo growth. Proc Natl
Acad Sci USA 2002; 99:314752.
63. Kaushal D, Schroeder BG, Tyagi S, et al. Reduced immunopathology
and mortality despite tissue persistence in a Mycobacterium tuber-
culosis mutant lacking alternative sigma factor, SigH. Proc Natl Acad
Sci USA 2002; 99:83305.
64. Yamamura Y, Ogawa Y, Maeda H, Yamamura Y. Prevention of tu-
berculous cavity formation by desensitization with tuberculin-active
peptide. Am Rev Respir Dis 1974; 109:594601.
65. Moreira AL, Tsenova L, Aman MH, et al. Mycobacterial antigens
exacerbate disease manifestations in Mycobacterium tuberculosis-in-
fected mice. Infect Immun 2002; 70:21007.
66. Turner J, Rhoades ER, Keen M, Belisle JT, Frank AA, Orme IM.
Effective preexposure tuberculosis vaccines fail to protect when they
are given in an immunotherapeutic mode. Infect Immun 2000;68:
17069.
67. Taylor JL, Turner OC, Basaraba RJ, Belisle JT, Huygen K, Orme IM.
Pulmonary necrosis resulting from DNA vaccination against tuber-
culosis. Infect Immun 2003; 71:21928.
68. Cardona PJ, Llatjos R, Gordillo S, et al. Towards a human-likemodel
of tuberculosis: intranasal inoculation of LPS induces intragranulom-
atous lung necrosis in mice infected aerogenically with Mycobacterium
tuberculosis. Scand J Immunol 2001; 53:6571.
69. Roach TI, Barton CH, Chatterjee D, Blackwell JM. Macrophage acti-
vation: lipoarabinomannan from avirulent and virulent strains ofMy-
cobacterium tuberculosis differentially induces the early genes c-fos, KC,
JE, and tumor necrosis factor-a. J Immunol 1993; 150:188696.
70. Yamamura Y. The pathogenesis of tuberculous cavities. Bibl Tuberc
1958; 13:1337.
71. Cadranel J, Philippe C, Perez J, et al. In vitro production of tumour
necrosis factor and prostaglandin E2 by peripheral blood mononuclear
cells from tuberculosis patients. Clin Exp Immunol 1990; 81:31924.
72. Flynn JL, Goldstein MM, Chan J, et al. Tumor necrosis factor-alpha
is required in the protective immune response against Mycobacterium
tuberculosis in mice. Immunity 1995; 2:56172.
73. Takashima T, Ueta C, Tsuyuguchi I, Kishimoto S. Productionof tumor
necrosis factor alpha by monocytes from patients with pulmonary
tuberculosis. Infect Immun 1990; 58:328692.
74. Condos R, Rom WN, Liu YM, Schluger NW. Local immuneresponses
correlate with presentation and outcome in tuberculosis. Am J Respir
Crit Care Med 1998; 157:72935.
75. Filley EA, Bull HA, Dowd PM, Rook GA. The effect ofMycobacterium
tuberculosis on the susceptibility of human cells to the stimulatory and
toxic effects of tumour necrosis factor. Immunology1992; 77:5059.
76. Olobo JO, Geletu M, Demissie A, et al. Circulating TNF-a, TGF-b,
and IL-10 in tuberculosis patients and healthy contacts. Scand J Im-
munol 2001; 53:8591.
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
9/10
Remodeling in TB JID 2005:192 (1 October) 1209
77. Saltini C, Colizzi V. Soluble immunological markers of disease activity
in tuberculosis. Eur Respir J 1999; 14:4856.
78. Filley EA, Rook GA. Effect of mycobacteria on sensitivity to the cytotoxic
effects of tumor necrosis factor. Infect Immun 1991; 59:256772.
79. Rook GA, Hernandez-Pando R, Dheda K, Teng SG. IL-4 in tuberculosis:
implications for vaccine design. Trends Immunol 2004; 25:4838.
80. Muller KM, Jaunin F, Masouye I, Saurat JH, Hauser C. Th2 cells medi-
ate IL-4-dependent local tissue inflammation. J Immunol 1993;150:
557684.
81. Hernandez-Pando R, Rook GA. The role of TNF-alpha in T-cell-me-
diated inflammation depends on the Th1/Th2 cytokine balance. Im-
munology 1994; 82:5915.
82. Lawrence CE, Paterson JC, Higgins LM, MacDonald TT, Kennedy
MW, Garside P. IL-4-regulated enteropathy in an intestinal nematode
infection. Eur J Immunol 1998; 28:267284.
83. Grzych JM, Pearce E, Cheever A, et al. Egg deposition is the major
stimulus for the production of Th2 cytokines in murine schistoso-
miasis mansoni. J Immunol 1991; 146:13227.
84. Hernandez-Pando R, Orozcoe H, Sampieri A, et al. Correlation between
the kinetics of Th1, Th2 cells and pathology in a murine model of ex-
perimental pulmonary tuberculosis. Immunology 1996; 89:2633.
85. Orme IM, Roberts AD, Griffin JP, Abrams JS. Cytokine secretion by
CD4 T lymphocytes acquired in response to Mycobacterium tubercu-
losis infection. J Immunol 1993; 151:51825.
86. Hernandez-Pando R, Aguilar D, Hernandez ML, Orozco H, Rook G.
Pulmonary tuberculosis in BALB/c mice with non-functional IL-4genes: changes in the inflammatory effects of TNF-a and in the reg-
ulation of fibrosis. Eur J Immunol 2004; 34:17483.
87. Mazzarella G, Bianco A, Perna F, et al. T lymphocyte phenotypic profile
in lung segments affected by cavitary and non-cavitary tuberculosis.
Clin Exp Immunol 2003; 132:2838.
88. van Crevel R, Karyadi E, Preyers F, et al. Increased production of
interleukin 4 by CD4+ and CD8+ T cells from patients with tuber-
culosis is related to the presence of pulmonary cavities. J Infect Dis
2000; 181:11947.
89. Saunders BM, Frank AA, Cooper AM, Orme IM. Role ofgd T cells
in immunopathology of pulmonary Mycobacterium avium infection
in mice. Infect Immun 1998; 66:550814.
90. Ehlers S, Benini J, Held HD, Roeck C, Alber G, Uhlig S. ab T cell
receptor-positive cells and interferon-g, but not inducible nitric oxide
synthase, are critical for granuloma necrosis in a mouse model ofmycobacteria-induced pulmonary immunopathology. J Exp Med 2001;
194:184759.
91. Florido M, Cooper AM, Appelberg R. Immunological basis of the
development of necrotic lesions following Mycobacterium avium in-
fection. Immunology 2002; 106:590601.
92. Malhotra I, Mungai P, Wamachi A, et al. Helminth- and bacillus
Calmette-Guerin-induced immunity in children sensitized in utero
to filariasis and schistosomiasis. J Immunol 1999; 162:68438.
93. Rook GAW, Dheda K, Zumla A. Do successful tuberculosis vaccines
need to be immunoregulatory rather than merely Th1-boosting? Vac-
cine 2005; 23:211520.
94. Manca C, Reed MB, Freeman S, et al. Differential monocyte activation
underlies strain-specific Mycobacterium tuberculosispathogenesis. In-
fect Immun 2004; 72:55114.
95. Agrewala JN, Wilkinson RJ. Differential regulation of Th1 and Th2 cells
by p91110 and p2140 peptides of the 16-kD a-crystallin antigen of
Mycobacterium tuberculosis. Clin Exp Immunol 1998; 114:3927.
96. Seah GT, Rook GA. IL-4 influences apoptosis of mycobacterium-re-
active lymphocytes in the presence of TNF-a. J Immunol 2001; 167:
12307.
97. Dheda K, Chang JS, Breen RA, et al. In vivo and in vitro studies of
a novel cytokine, interleukin 4d2, in pulmonary tuberculosis. Am J
Respir Crit Care Med 2005; 172:5018.
98. Fayyazi A, Eichmeyer B, Soruri A, et al. Apoptosis of macrophages
and T cells in tuberculosis associated caseous necrosis. J Pathol 2000;
191:41725.
99. Silva CL, Lowrie DB. Identification and characterization of murine
cytotoxic T cells that kill Mycobacterium tuberculosis. Infect Immun
2000; 68:326974.
100. Cho S, Mehra V, Thoma-Uszynski S, et al. Antimicrobial activity of
MHC class I-restricted CD8+ T cells in human tuberculosis. Proc
Natl Acad Sci USA 2000; 97:122105.
101. Krensky AM. Granulysin: a novel antimicrobial peptide of cytolytic
T lymphocytes and natural killer cells. Biochem Pharmacol 2000;59:
31720.
102. Kusner DJ, Barton JA. ATP stimulates human macrophages to kill
intracellular virulent Mycobacterium tuberculosis via calcium-depen-
dent phagosome-lysosome fusion. J Immunol 2001; 167:330815.
103. Lammas DA, Stober C, Harvey CJ, Kendrick N, Panchalingam S,
Kumararatne DS. ATP-induced killing of mycobacteria by human
macrophages is mediated by purinergic P2Z(P2X7) receptors. Im-
munity 1997; 7:43344.
104. Keane J, Shurtleff B, Kornfeld H. TNF-dependent BALB/c murine
macrophage apoptosis following Mycobacterium tuberculosisinfection
inhibits bacillary growth in an IFN-gamma independent manner. Tu-
berculosis (Edinb) 2002; 82:5561.
105. Oddo M, Renno T, Attinger A, Bakker T, MacDonald HR, Meylan
PR. Fas ligand-induced apoptosis of infected human macrophages
reduces the viability of intracellular Mycobacterium tuberculosis. J Im-
munol 1998; 160:544854.
106. Laochumroonvorapong P, Paul S, Manca C, Freedman VH, Kaplan G.
Mycobacterial growth and sensitivity to H2O2 killing in human mono-cytes in vitro. Infect Immun 1997; 65:48507.
107. Molloy A, Laochumroonvorapong P, Kaplan G. Apoptosis, but not
necrosis, of infected monocytes is coupled with killing of intracellular
bacillus Calmette-Guerin. J Exp Med 1994; 180:1499509.
108. Maiti D, Bhattacharyya A, Basu J. Lipoarabinomannan from Myco-
bacterium tuberculosis promotes macrophage survival by phosphor-
ylating Bad through a phosphatidylinositol 3-kinase/Akt pathway. J
Biol Chem 2001; 276:32933.
109. Rojas M, Garcia LF, Nigou J, Puzo G, Olivier M. Mannosylatedlipoara-
binomannan antagonizes Mycobacterium tuberculosisinduced macro-
phage apoptosis by altering Ca+2-dependent cell signaling. J Infect Dis
2000; 182:24051.
110. Wille A, Gerber A, Heimburg A, et al. Cathepsin L is involved in ca-
thepsin D processing and regulation of apoptosis in A549 human lung
epithelial cells. Biol Chem 2004; 385:66570.111. Jayasankar K, Shakila H, Umapathy KC, Ramanathan VD. Biochem-
ical and histochemical changes pertaining to active and healed cu-
taneous tuberculosis. Br J Dermatol 2002; 146:97782.
112. Broekelmann TJ, Limper AH, Colby TV, McDonald JA. Transforming
growth factor beta 1 is present at sites of extracellular matrix gene
expression in human pulmonary fibrosis. Proc Natl Acad Sci USA
1991; 88:66426.
113. Liu JY, Sime PJ, Wu T, et al. Transforming growth factor-b1
overex-
pression in tumor necrosis factor-a receptor knockout mice induces
fibroproliferative lung disease. Am J Respir Cell Mol Biol 2001; 25:37.
114. Sime PJ, Xing Z, Graham FL, Csaky KG, Gauldie J. Adenovector-me-
diated gene transfer of active transforming growth factor-b1 induces
prolonged severe fibrosis in rat lung. J Clin Invest 1997; 100:76876.
115. Desmouliere A, Redard M, Darby I, Gabbiani G. Apoptosis mediates
the decrease in cellularity during the transition between granulation
tissue and scar. Am J Pathol 1995; 146:5666.
116. Ramos C, Montano M, Garcia-Alvarez J, et al. Fibroblasts from id-
iopathic pulmonary fibrosis and normal lungs differ in growth rate,
apoptosis, and tissue inhibitor of metalloproteinases expression. Am
J Respir Cell Mol Biol 2001; 24:5918.
117. Denis M, Ghadirian E. Transforming growth factor-beta is generated
in the course of hypersensitivity pneumonitis: contributionto collagen
synthesis. Am J Respir Cell Mol Biol 1992; 7:15660.
118. Piguet PF, Collart MA, Grau GE, Sappino AP, Vassalli P. Requirement
of tumour necrosis factor for development of silica-induced pulmo-
nary fibrosis. Nature 1990; 344:2457.
-
7/29/2019 Remodelacion Pulmonar en Tuberculosis
10/10
1210 JID 2005:192 (1 October) Dheda et al.
119. Selman M, Pardo A. The epithelial/fibroblastic pathway in the path-
ogenesis of idiopathic pulmonary fibrosis. Am J Respir Cell Mol Biol
2003; 29(Suppl):S937.
120. Elias JA, Freundlich B, Kern JA, Rosenbloom J. Cytokine networks in
the regulation of inflammation and fibrosis in the lung. Chest 1990;
97:143945.
121. Rider C. Many cytokines and interleukins bind to glycosaminoglycans
[letter]. Immunol Today 1993; 14:615.
122. Giri SN, Hyde DM, Marafino BJ Jr. Ameliorating effect of murine
interferon gamma on bleomycin-induced lung collagen fibrosis in
mice. Biochem Med Metab Biol 1986; 36:1947.
123. Serpier H, Gillery P, Salmon-Ehr V, et al. Antagonistic effects of in-
terferon-gamma and interleukin-4 on fibroblast cultures. J Invest Der-
matol 1997; 109:15862.
124. Wangoo A, Sparer T, Brown IN, et al. Contribution of Th1 and Th2
cells to protection and pathology in experimental models of granu-
lomatous lung disease. J Immunol 2001; 166:34329.
125. Lee CG, Homer RJ, Zhu Z, et al. Interleukin-13 induces tissue fibrosis
by selectively stimulating and activating transforming growth factor
b1. J Exp Med 2001; 194:80921.
126. Wynn TA, Cheever AW, Jankovic D, et al. An IL-12-based vaccination
method for preventing fibrosis induced by schistosome infection. Na-
ture 1995; 376:5946.
127. Moller DR. Pulmonary fibrosis of sarcoidosis: new approaches, old
ideas. Am J Respir Cell Mol Biol 2003; 29(Suppl):S3741.
128. Kunkel SL, Chensue SW, Lukacs N, Hogaboam C. Cytokine phe-notypes serve as a paradigms for experimental immune-mediatedlung
diseases and remodeling. Am J Respir Cell Mol Biol 2003; 29(Suppl):
S636.
129. Chensue SW, Warmington K, Ruth J, Lincoln P, Kuo MC, Kunkel
SL. Cytokine responses during mycobacterial and schistosomal an-
tigen-induced pulmonary granuloma formation: production of Th1
and Th2 cytokines and relative contribution of tumor necrosis fac-
tor. Am J Pathol 1994; 145:110513.
130. Wynn TA, Eltoum I, Cheever AW, Lewis FA, Gause WC, Sher A.
Analysis of cytokine mRNA expression during primary granuloma
formation induced by eggs of Schistosoma mansoni. J Immunol 1993;
151:143040.
131. Gillery P, Fertin C, Nicolas JF, et al. Interleukin-4 stimulates colla-
gen gene expression in human fibroblast monolayer cultures: poten-
tial role in fibrosis. FEBS Lett 1992; 302:2314.132. Oriente A, Fedarko NS, Pacocha SE, Huang SK, Lichtenstein LM, Es-
sayan DM. Interleukin-13 modulates collagen homeostasis in human
skin and keloid fibroblasts. J Pharmacol Exp Ther 2000; 292:98894.
133. Zhu Z, Homer RJ, Wang Z, et al. Pulmonary expression of interleu-
kin-13 causes inflammation, mucus hypersecretion, subepithelial fi-
brosis, physiologic abnormalities, and eotaxin production. J Clin In-
vest 1999; 103:77988.
134. Kaplan MH, Whitfield JR, Boros DL, Grusby MJ. Th2 cells are re-
quired for the Schistosoma mansoni egg-induced granulomatous re-
sponse. J Immunol 1998; 160:18506.
135. Atamas SP, Yurovsky VV, Wise R, et al. Production of type 2 cytokines
by CD8+ lung cells is associated with greater decline in pulmonary
function in patients with systemic sclerosis. Arthritis Rheum 1999;
42:116878.
136. Seah GT, Scott GM, Rook GA. Type 2 cytokine gene activation and
its relationship to extent of disease in patients with tuberculosis. J In-
fect Dis 2000; 181:3859.
137. Seah GT, Rook GA. High levels of mRNA encoding IL-4 in unstim-
ulated peripheral blood mononuclear cells from tuberculosis patients
revealed by quantitative nested reverse transcriptase-polymerasechain
reaction; correlations with serum IgE levels. Scand J Infect Dis 2001;
33:1069.
138. Dheda K, Johnson MA, Zumla A, Rook GA. Smoking is not beneficial
for tuberculosis [letter]. Am J Respir Crit Care Med 2004; 170:821.
139. Hance AJ, Basset F, Saumon G, et al. Smoking and interstitial lung
disease: the effect of cigarette smoking on the incidence of pulmonary
histiocytosis X and sarcoidosis. Ann N Y Acad Sci 1986; 465:64356.140. Warren CP. Extrinsic allergic alveolitis: a disease commoner in non-
smokers. Thorax 1977; 32:5679.
141. King TE Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Pre-
dicting survival in idiopathic pulmonary fibrosis: scoring system and
survival model. Am J Respir Crit Care Med 2001; 164:117181.
142. King TE Jr, Schwarz MI, Brown K, et al. Idiopathic pulmonary fibro-
sis: relationship between histopathologic features and mortality. Am
J Respir Crit Care Med 2001; 164:102532.
143. Arinobu Y, Atamas SP, Otsuka T, et al. Antagonistic effects of an
alternative splice variant of human IL-4, IL-4d2, on IL-4 activities in
human monocytes and B cells. Cell Immunol 1999; 191:1617.
144. Atamas SP, Choi J, Yurovsky VV, White B. An alternative splice var-
iant of human IL-4, IL-4d2, inhibits IL-4-stimulated T cell prolifer-
ation. J Immunol 1996; 156:43541.
145. Martino A, Sacchi A, Sanarico N, et al. Dendritic cells derived from
BCG-infected precursors induce Th2-like immune response. J Leukoc
Biol 2004; 76:82734.
146. Pathan AA, Wilkinson KA, Klenerman P, et al. Direct ex vivo analysis
of antigen-specific IFN-g-secreting CD4 T cells in Mycobacterium tu-
berculosis-infected individuals: associations with clinical disease state
and effect of treatment. J Immunol 2001; 167:521725.
147. Zuany-Amorim C, Sawicka E, Manlius C, et al. Suppression of airway
eosinophilia by killed Mycobacterium vaccae-induced allergen-specific
regulatory T-cells. Nat Med 2002; 8:6259.
148. Zuany-Amorim C, Manlius C, Trifilieff A, et al. Long-term protective
and antigen-specific effect of heat-killed Mycobacterium vaccae in a
murine model of allergic pulmonary inflammation. J Immunol 2002;
169:14929.
149. Johnson JL, Kamya RM, Okwera A, et al. Randomized controlledtrial
of Mycobacterium vaccae immunotherapy in nonhuman immuno-
deficiency virusinfected Ugandan adults with newly diagnosed pul-
monary tuberculosis. J Infect Dis 2000; 181:130412.
150. Luo Y, Lu S, Guo S. Immunotherapeutic effect of Mycobacterium vaccae
on multi-drug resistant pulmonary tuberculosis [in Chinese]. Zhonghua
Jie He He Hu Xi Za Zhi 2000; 23:858.
151. Stanford J, Stanford C, Grange J. Immunotherapywith Mycobacterium
vaccae in the treatment of tuberculosis. Front Biosci 2004; 9:170119.
152. Sampaio EP, Hernandez MO, Carvalho DS, Sarno EN. Management
of erythema nodosum leprosum by thalidomide: thalidomide ana-
logues inhibit M. leprae-induced TNFa production in vitro. Biomed
Pharmacother 2002; 56:139.
153. Tramontana JM, Utaipat U, Molloy A, et al. Thalidomide treatment
reduces tumor necrosis factor alpha production and enhances weight
gain in patients with pulmonary tuberculosis. Mol Med 1995; 1:38497.
154. Weiner HL. Oral tolerance: immune mechanisms and the genera-
tion of Th3-type TGF-beta-secreting regulatory cells. Microbes Infect
2001; 3:94754.