Respiratory Presentation
93
Respiratory
-
Upload
meducationdotnet -
Category
Documents
-
view
166 -
download
0
Transcript of Respiratory Presentation

Respiratory

Lung VolumesInspiratory Reserve Volume
Inspiratory Reserve Volume
Vital Capacity Total
Lung Capacity
Tidal Volume
Tidal Volume
Expiratory Reserve Volume Functional
Residual Capacity
Residual Volume
Residual Volume

SpirometryVo
lum
e
Time
FEV1
FVC

Alternatively…
Volume (L)
Flow
(L/s
ec)
Inspiration
Expiration

Mechanics

Gas Exchange
Control of Respiration
Pontine Controll• Pneumotaxic centre• Apneustic centre
Medullary Control• Dorsal respiratory group• Ventral respiratory group
Investigations – Blood Tests• Full Blood Count• Urea & Electrolytes• Thyroid Function Tests• Arterial Blood Gas• Blood Cultures

Investigations - Imaging• Chest X-ray• CT scan• Ultrasound• Bronchoscopy• Pulmonary Angiography• MRI

Investigations - Others• Spirometry• Biopsy• Pleural biopsy• Bronchoalveolar lavage
• Video assisted Thoracoscopy• Sputum analysis• Pleural fluid aspirate & analysis• Exercise testing• Genetic testing

A 24-year old known IV drug abuser is bought into A&E unconscious. His respiratory rate is 4/min and his SaO2 is 85% on air.

Respiratory AcidosispH = 7.21PaCO2 = 11.9PaO2 = 8.2HCO3
- = 26Base Excess = 1

With Partial Metabolic CompensationpH = 7.31PaCO2 = 9.8PaO2 = 9.9HCO3
- = 34Base Excess = 8

CompensatedpH = 7.37PaCO2 = 6.7PaO2 = 10.9HCO3
- = 34Base Excess = 8

Management ApproachesVentilation
Pharmacology
Oxygen
Invasive
Non-InvasiveVs
Bronchodilators Respiratory Stimulants
Drug Antagonists Bicarbonate

A 34-year old woman with known anxiety disorder is bought in to A&E after a major panic attack. Her respiratory rate is 32/min.

Respiratory AlkalosispH = 7.47PaCO2 = 3.2PaO2 = 16HCO3
- = 22Base Excess = -1

With Partial Metabolic CompensationpH = 7.47PaCO2 = 3.7PaO2 = 13.7HCO3
- = 10Base Excess = -13

Fully CompensatedpH = 7.4PaCO2 = 4.2PaO2 = 12.6HCO3
- = 12Base Excess = -12

Management ApproachesTreat underlying disorder
Respiratory Failure Type 1
A 26-year old female comes in following a sudden collapse. She is a known asthmatic. She is tachypnoeic, tachycardic, normotensive, apyrexic and her SaO2 is 89% on air. An arterial blood gas is performed. The results are below:-pH - 7.36
PaO2 - 7.6
PaCO2 - 5.6
HCO3- - 24
Base Xs - -1

Causes
Management• Treat underlying cause• Give O2 to correct hypoxia• Consider assisted ventilation
Respiratory Failure Type 2
A 56-year old ex-smoker is bought into A&E. She is responsive to voice and her breathing is laboured. She is a known COPD patient. An ABG reveals the following:pH - 7.32
PaO2 - 7.6
PaCO2 - 7.6
HCO3- - 26
Base Xs - -2

Causes• Asthma/COPD/Pneumonia• Sedative Drugs• Cord lesion, Myasthenia Gravis, Guillain-Barré• Flail Chest/Kyphoscoliosis

Management• Underlying cause• O2 Therapy• ABG monitoring• Ventilation/Intubation

Asthma
A 12- year old is bought to the GP. His mother says he complains of chest tightness during PE and he has recently started coughing throughout the night. He has not been feeling unwell at all recently and had eczema as a child. His brother is a diagnosed asthmatic.

Spirometry• Recommended in ALL adults• Recommended in children if able to do test and have a probability of
asthma

What it looks like…
Volume (L)
Flow
(L/s
ec)

Managing A New Presentation In Children
Lifestyle Advice SABA ± Corticosteroid
Referral to Respiratory Paediatrician
Leukotriene Receptor Antagonist
LABA
Increase Steroids
Under 2
2-5 Over 5
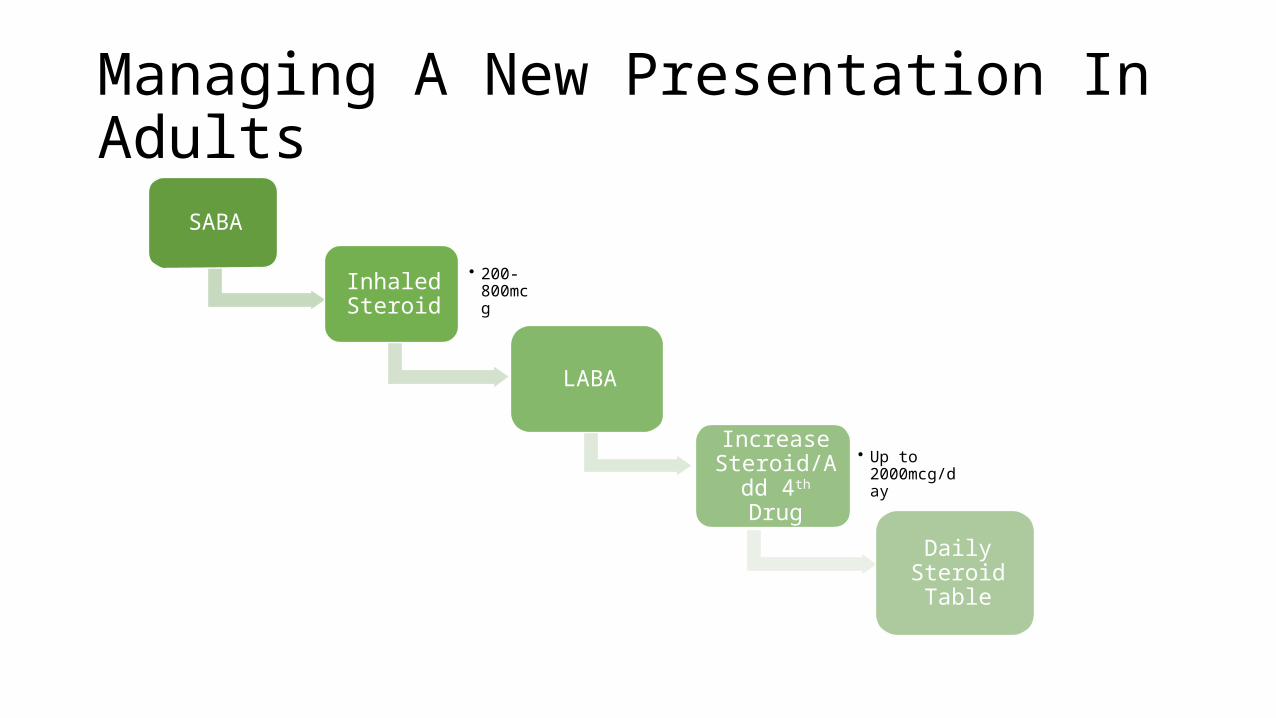
Managing A New Presentation In Adults
SABA
• 200-800mcg
Inhaled Steroid
LABA
Increase Steroid/Add
4th Drug
• Up to 2000mcg/day
Daily Steroid Table

Stepping Down Treatment• SLOWLY• Make sure patient feels Asthma is well controlled• Advise exacerbations may occur• Step down steroid dose 20-30% every 3-months

Asthma
A 21-year old female presents to A&E with a 3-day history of shortness of breath and wheezing. This is not relieved by her inhaler. It is disturbing her sleep and she cannot concentrate in her university classes. She has been asthmatic since childhood and takes a regular corticosteroid inhaler.

Assessing SeverityModerate Severe Life-threatening
PEF > 50% best or predicted
Speech normal
RR < 25 / min
Pulse < 110 bpm
PEF 33 - 50% best or predicted
Can't complete sentences
RR > 25/min
Pulse > 110 bpm
PEF < 33% best or predictedOxygen sats < 92%Silent chest, cyanosis or feeble respiratory effortBradycardia, dysrhythmia or hypotensionExhaustion, confusion or coma

Investigations• FBC• U&Es• PEAK FLOW• ABG• CXR• All the rest – LFTs, Glucose etc.

Do they need admitting?
Yes• Life-threatening• Severe asthma that doesn’t
respond rapidly• Moderate who have a factor
that warrants a lower threshold
No• Severe asthma that respons
rapidly• Moderate asthma
Managing an Admission• High Flow O2
• Salbutamol Nebuliser• Give the first dose of a course of prednisolone/IV hydrocortisone• Monitor PEFR and O2 sats to determine response to treatment• Nebulised Ipratropium Bromide• IV Magnesium Sulphate• IF STILL NO RESPONE IV SALBUTAMOL

Managing a Patient Who Does NOT Need Admission• Steroid course• Do NOT prescribe antibiotics unless indicated• Use SABA - 2 puffs every 2 minutes up to 10 puffs• Repeat every 10-20 minutes and reassess
• Advice to monitor PEFR and symptoms• Consider initiating montelukast if over 2 years• Follow up within 24 hours either with GP or respiratory physician and
1 week later
COPD
A 52-year old presents to her GP with increasing breathlessness when she’s walking that’s been coming on over the past year. She has noticed a dry cough more recently since September, alongside feeling very lethargic. She has smoked 50 cigarettes a day for the past 25 years of her life. You note last Winter and the Winter previous she was treated for bronchitis.
Investigations• Post-Bronchodilator Spirometry• Chest X-ray• Full Blood Count• Body Mass Index


Diagnosis & Assessing Severity
Post-bronchodilator FEV1/FVC FEV1 (of predicted) Severity
< 0.7 > 80% Stage 1 - Mild**
< 0.7 50-79% Stage 2 - Moderate
< 0.7 30-49% Stage 3 - Severe
< 0.7 < 30% Stage 4 - Very severe

Managing Stable COPD
GeneralSmoking CessationAnnual Influenza
VaccineOne-Off Pneumococcal
Vaccine
BronchodilatorsSABA/SAMA First-line
FEV1>50% - LABA/LAMAFEV1<50% -
LABA+ICS/LAMA
Next StepsIf taking LABA, add ICS
If taking LABA + ICS, add LAMA
Oral TheophyllineMucolytics
Cor PulmonaleLoop Diuretic
Consider for LTOT
NutritionDietician if BMI <20 or
>25Nutritional
Supplements if BMI <20

Oxygen Criteria
Long-Term Oxygen Therapy
Ambulatory Oxygen Therapy
Short-Burst Oxygen Therapy
Severe Airflow Obstruction People on LTOT who wish to have O2 outside the home
If not appropriate for LTOT
Cyanosis
Polycythaemia
Peripheral Oedema
Raised JVP
PaO2 ≤ 92% on air

Acute Exacerbations• Assess and decide to admit• Follow Hospital-at-home scheme if possible
• Follow instructions on oxygen alert card• Administer oxygen• 100% OR 28% venture mask 4L/min and titrate

Treatments• Increase bronchodilator use and give via nebuliser• 30mg Prednisolone daily for 7-14 days• Give antibiotics if sputum purulent or clinical signs of pneumonia• Amoxicillin 500mg TDS OR Doxycycline 200mg then 100mg OD for 5 days• OR Erythromycin 500mg QDS/Clarithromycin 500mg BD for 5 days

Bronchiectasis
A 32-year old presents with a cough that has been ongoing for several months. She produces green-sputum daily, but doesn’t feel feverish. She does not ave a history of smoking. You note when she was younger she was hospitalised with pneumonia and has previously cultivated Pseudomonas in her sputum.On examination you observe her fingers are clubbed, and hear coarse crackles during early inspiration.

Investigations• Chest X-ray• High resolution CT• Cystic fibrosis testing• Antibody deficiency• Immunological disorder investigations• Bronchoscopy• 24-hour pH monitorin
Management• Physical inspiratory muscle training• Postural Drainage• Immunisations• Bronchodilators• Antibiotics• Dependent on previous sputum results & Local Guidelines

Smoking Cessation
Varenicline
Nicotine Replacement
Therapy
Bupropion

Pleural Fluid AnalysisTransudate Exudate
Main causesIncreased hydrostaticpressure,Decreased colloidosmotic pressure
Inflammation
Appearance Clear Cloudy
Protein content < 25 g/L > 29 g/fluid protein
serum protein < 0.5 > 0.5
Difference ofalbumin contentwith blood albumin
> 1.2 g/dL < 1.2 g/dL
fluid LDHupper limit for serum < 0.6 or < ⅔ > 0.6 or > ⅔
Cholesterol content < 45 mg/dL > 45 mg/dL

↑ ↓
pH Empyema/Cancer
Glucose Cancer/Bacterial Infection/Rheumatoid
PleuritisAmylase Oesophageal Rupture,
Pancreatic Pleural Effusion, Cancer
Cytology If neg:- thorascopy/needle biopsy
Gram staining Culture and test for TB if indicated
Community-Acquired Pneumonia
A 53-year old male is bought into A&E with dyspnoea and fever coming on over the last day. He has started coughing up purulent sputum. He is in pain when he breathes in. He has recently returned from holiday in France and is noted to have an ulcerated lesion on his upper lip.On examination you find decreased chest expansion on the right hand side, dullness to percussion, bronchial breathing and coarse inspiratory crackles.
Aetiology
Organism• Pneumococcus
• Haemophilus
• Staphylococcus• Klebsiella• Pseudomonas
History• Most common. Commonly
reactivates herpes• Most common infective
exacerbation of COPD• Commonly occurs after the flu• Classically in alcoholic• Common in CF and bronchiectasis

Aetiology
Organism• Mycoplasma
• Legionella
• Chlamydophila
• Pneumocystis jiruveci
History• Epidemics. Flu-like symptoms with
dry cough• Colonises water tanks. Typically post
travel. Anorexia, D&V, hepatitis, renal failure• Biphasic illness – pharyngitis,
hoarseness, otitis followed by cough• Causes pneumonia in
immunosuppressed


Investigations

• Full blood count• Urea & Electrolytes• C-reactive protein• Blood cultures• Sputum C&S• Arterial Blood Gas
Assessing Severity• Mini-mental score of 6/10• Urea of 11.4 mmol/L• C-reactive protein of 154• Respiratory Rate of 30• Aged 75• Blood Pressure 87/65
• Mini-mental score of 6/10• Urea of 11.4 mmol/L• C-reactive protein of 154• Respiratory Rate of 30• Aged 75• Blood Pressure 87/65

Management• Low – Moderate Severity CAP• Oral Amoxicillin ± macrolide if admitted
• High Severity CAP• IV Co-amoxiclav + clarithromycin• Cefuroxime + clarithromycin• Cefotaxime + clarithromycin
• Oxygen & analgesia
Hospital-Acquired Pneumonia
A 72-year old female is in hospital following a traumatic injury resulting in a hip replacement. 48 hours after her operation she becomes breathless and has a high-grade fever. A chest x-ray performed shows acute changes compared to an X-ray the FY1 took in A&E.

Complications• Respiratory Failure• Hypotension• Atrial Fibrillation• Pleural Effusion• Empyema• Lung Abscess• Septicaema• Pericarditis• Jaundice

Tuberculosis
An 18-year old female smoker attended her GP complaining of a cough. It’s been ongoing for about 4 weeks and yesterday she coughed up blood. She has noticed some weight loss and at night she’s been waking up with the sheets soaked.She rarely comes to the GP and lives in a council block of high-rise flats.

Investigations• General ones• CXR• Three sputum samples for microscopy, sensitivities and culture

Management• Rifampacin• Isoniazid• Pyrazinamide• Ethambutol
2 Months initial phase
4 months continuation
Pharmacology• Rifampacin• Inhibits bacterial DNA dependent RNA polymerase preventing transcription• Potent liver enzyme inducer (decreases action of warfarin)• Hepatitis, orange secretions• Flu-like symptoms

Pharmacology• Isoniazid• Inhibits mycolic acid synthesis• Peripheral neuropathy (give with Vitamin B6)• Hepatitis, agranulocytosis• Liver enzyme inhibitor (increases action of warfarin)

Pharmacology• Pyrazinamide• Converted into pyrazinoic acid which inhibits fatty acid synthase• Hyperuricaemia causing gout• Hepatitis

Pharmacology• Ethambutol• Inhibits arabinosyl transferase which polymerises arabinose into arabinan• Optic neuritis• Dose needs adjusting in patients with renal impairment

Pneumothorax under Tension
A 22-year old male presents with right sided chest pain and difficulty breathing. You note he is extremely tall and has arachnodactyly. The pain is worth on breathing in and his PaO2 is 95% on room air.
You notice the right side of his chest isn’t expanding fully, and is hyper-resonant on percussion. You hear no air entry on the right hand side either. His apex beat is laterally displaced.

• Aspirate• 2nd Intercostal space, mid-clavicular line• Large bore needle with syringe attached, partially filled with saline• Remove plunger to allow air to bubble through saline
• Insert chest drain• Follow protocol, STERILE procedure• Insert 4th-6th intercostal space anterior-mid axillary line

Primary Pneumothorax NOT under tension
CXR
SOB and/or rim of air > 2 cm on CXR
Aspiration successful?
Repeat aspiration
Chest drain
Consider discharge with outpatient monitoring
NO
NO
NO
YES
YES
YES

Secondary Pneumothorax NOT under tension
CXR
SOB and/or rim of air >2cm on CXR and age >50 Rim of air <1 cm
Chest drain Aspirate Admit for 24 hours and give O2
NOYES
YESNO

Carbon Monoxide Poisoning
A 73-year old gentleman is bought in to the GP by his son-in-law after a few weeks being very confused and unsure where he is. He has also had headaches for the past few weeks. On examination he has a low-grade pyrexia and has abnormally pink mucosa.His son-in-law asks for some pills for a headache he woke up with this morning. He stayed in the same house last night.

Cystic Fibrosis
A 3-year old is bought in with diarrhoea and shortness of breath. He has been vomiting up thick green sputum and struggling to clear his throat.On examination you notice a small rectal prolapse and that his weight has dropped two centiles. Looking back through his notes you see he has been treated for several chest infections within the past year.

Investigations• Sweat testing• Molecular genetic testing• Faecal elastase• Spirometry• Sputum microbiology• General tests

Management• Chest• Regular physiotherapy• Antibiotics• Mucolytics• Bronchodilators
• GI tract• Pancreatic enzyme replacement• Vitamin ADEK• Ursodeoxycholic acid
Other Management• Screen for CF-related diabeters• Screen and treat osteoporosis• Arthritis• Sinusitis• Vasculitis• Fertility & genetic counselling

Advanced Disease• O2
• Diuretics• NIV• Lung transplantation• Liver transplantation
Lung Cancer
A 56-year old female presents with a 3 week history of shoulder pain, shortness of breath and haemoptysis. She has a 30-pack year history.On examination there is nail bed fluctuation and cervical lymphadenopathy.You refer her urgently for a chest x-ray.

Type of Lung CancerSquamous = 35%Adenocarcinoma = 30%Small Cell = 15%Large Cell = 10%Other = 5%

Features of Small Cell Lung Cancer• Usually central• Arise from APUD cells• Associated with ectopic ADH & ACTH secretion• Hyponatremia• Cushing’s syndrome• Hypokalemic alkalosis
• Lambert-Eaton syndrome

Management of Small Cell Lung Cancer• Chemotherapy & Radiotherapy• Extensive disease = palliation• Surgery only appropriate for debulking

Features of Non-Small Cell Lung Cancer• Squamous cell cancer• Typically central• Ectopic PTH secretion causing hypercalcaemia• Hypertrophic pulmonary osteoarthropathy
• Adenocarcinoma• Most common in non-smokers• Located on periphery

Management of Non-Small Cell Lung Cancers• Excision if no metastatic spread• Chemotherapy ± radiotherapy for advanced disease

StagingTumour Description
TX Malignant cells in bronchial secretions
TIS Carcinoma in situ
T0 None evident
T1 <3cm in lobar or distal airway
T2 >3 cm and >2cm distal to carina or ANY size if pleural involvement
T3 Involves chest wall, diaphragm, mediastinal pleura, pericardium or <2cm from carina
T4 Involves mediastinum, heart, great vessels, trachea, oesophagus
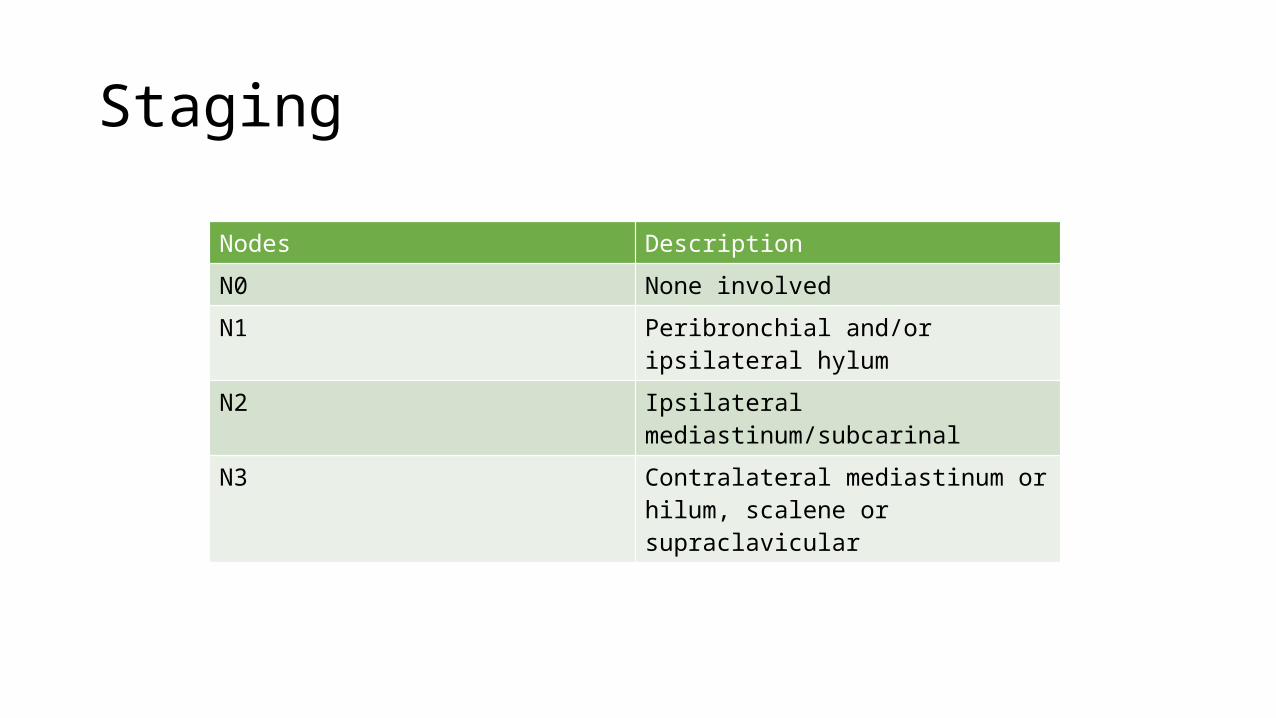
StagingNodes Description
N0 None involved
N1 Peribronchial and/or ipsilateral hylum
N2 Ipsilateral mediastinum/subcarinal
N3 Contralateral mediastinum or hilum, scalene or supraclavicular

StagingMetastases Description
M0 None
M1 Distant metastases

Superior Vena Cava Obstruction
A 72-year old female comes for review. She has a history of small cell lung cancer for which she has recently completed a course of chemotherapy.Over the past week she has become more short of breath and has noticed some facial swelling. She also has a headache. You notice she has distended neck veins although examination of the chest reveals nothing further.

Interstitial Lung Disease
A 44-year old male presents with a history of exertional breathlessness and dry cough that’s been on and off for a few months. On examination he is apyrexic and has no crackles, but you do hear widespread abnormal air entry and breath sounds.You refer for a chest x-ray which returns with interstitial shadowing, and refer him for a HRCT scan and spirometry.

Sarcoidosis• Multisystem granulomatous disorder of unknown cause• Cause of erythema nodosum• Hilar lymphadenopathy, dry cough, dyspnoea, polyarthralgia• Hepato/splenomegaly, keratoconjunctivitis sicca, uveitis, glaucoma,
bells palsy, lupus pernio, nodules, cardiomyopathy, hypercalcaemia• Raised ESR, LFTs, ACE, Ca2+, immunoglobulins• Bed rest, NSAIDs in acute sarcoidosis• Steroid therapy if parenchymal lung disease, uveitis, hypercalcaemia,
neurological/cardiological involvement
Goodpasture’s Syndrome• Acute glomerulonephritis and pulmonary alveolar haemorrhage• Autoimmune disease• Type II hypersensitivity
• Chills & fever, nausea & vomiting, weight loss, chest pain, pulmonary haemorrhage, haematuria, AKI, arthralgia• Anti-glomerular basement membrane antibodies are diagnostic• Plasmapharesis, immunosuppression, remove identifiable causes

Kartagener’s Syndrome• Autosomal recessive syndrome• Defects in structure and function of sensory and motile cilia• Situs inversus, abnormal frontal sinuses (causing sinusitis and
bronchiectasis), primary ciliary dyskinesia• Upper respiratory symptoms, otitis media,
COPD/bronchiectasis/recurrent pneumonia• Medical – antibiotics, bronchodilators, mucolytics, physiotherapy,
vaccination• Surgery – tympanostomy tubes, endoscopic sinus surgery, lobectomy