Scottsdale Instit Presentation- Wegmiller

of 116
-
Upload
rick-kneipper -
Category
Documents
-
view
226 -
download
0
Transcript of Scottsdale Instit Presentation- Wegmiller
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
1/116
Health Care OutlookThe Need forCost Management is Real
Scottsdale Institute ConferenceScottsdale, ArizonaApril 14, 2000
Health Care OutlookThe Need forCost Management is Real
Scottsdale Institute ConferenceScottsdale, ArizonaApril 14, 2000
bybyDonald C. Wegmiller, PresidentDonald C. Wegmiller, President
HealthCare Compensation StrategiesHealthCare Compensation Strategies
HEALTHCARE COMPENSATION STRATEGIESa division of Clark/Bardes
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
2/116
Environmental Assessment 2000Environmental Assessment 2000--20042004
Leadership Survey 1999Leadership Survey 1999 Financial Status 2000Financial Status 2000--20022002 Managed Care Plan StatusManaged Care Plan Status Shortage of ProfessionalsShortage of Professionals Current and Future Leadership in Health CareCurrent and Future Leadership in Health Care Physician Hospital Integration (Retain orPhysician Hospital Integration (Retain or
Divest ?)Divest ?) Credit CrunchCredit Crunch
Critical Success FactorsCritical Success Factors Review Top 10 Critical Success Factors toReview Top 10 Critical Success Factors to
Succeed in New EnvironmentSucceed in New Environment
SummarySummary
Environmental Assessment 2000Environmental Assessment 2000--20042004
Leadership Survey 1999Leadership Survey 1999 Financial Status 2000Financial Status 2000--20022002 Managed Care Plan StatusManaged Care Plan Status Shortage of ProfessionalsShortage of Professionals Current and Future Leadership in Health CareCurrent and Future Leadership in Health Care Physician Hospital Integration (Retain orPhysician Hospital Integration (Retain or
Divest ?)Divest ?) Credit CrunchCredit Crunch
Critical Success FactorsCritical Success Factors Review Top 10 Critical Success Factors toReview Top 10 Critical Success Factors to
Succeed in New EnvironmentSucceed in New Environment
SummarySummary
Overview of PresentationOverview of PresentationOverview of PresentationOverview of Presentation
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
3/116
ENVIRONMENTAL ASSESSMENT 2000ENVIRONMENTAL ASSESSMENT 2000--20042004
EALT
AREOM
ENSATION
STRATE IES
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
4/116
Leadership Survey 1999Leadership Survey 1999
L
S
S S
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
5/116
ByByHospitals and Health NetworksHospitals and Health Networks 700 health care executives700 health care executives
Rank 30 issues for both importance andRank 30 issues for both importance andpreparednesspreparedness
ByByHospitals and Health NetworksHospitals and Health Networks 700 health care executives700 health care executives
Rank 30 issues for both importance andRank 30 issues for both importance andpreparednesspreparedness
Leadership Survey 1999Leadership Survey 1999
L! "
#
R
#
$ % & '
S ! ( $ '
S! R ! ) ( S
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
6/116
Top 5 issues for importance:Top 5 issues for importance:Physician and administrative collaborationPhysician and administrative collaborationControlling costsControlling costs Improving customer serviceImproving customer service Increasing patient satisfactionIncreasing patient satisfaction Investment incomeInvestment income
Top 5 issues for importance:Top 5 issues for importance:Physician and administrative collaborationPhysician and administrative collaborationControlling costsControlling costs Improving customer serviceImproving customer service Increasing patient satisfactionIncreasing patient satisfaction Investment incomeInvestment income
0
1 2 3 4 5
C2 6 1
C7 8 P1 9 @ 2 4 I7 9
A
4 6 2 4 1 B
I1
@
eadership urvey 1999eadership urvey 1999
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
7/116
Top six* issues for strategic gap:Top six* issues for strategic gap:
Controlling costsControlling costs Improving customer serviceImproving customer service Increasing patient satisfactionIncreasing patient satisfaction
Improving community health statusImproving community health statusMeasuring quality of care/improvingMeasuring quality of care/improvingoutcomesoutcomes
Medicare managed care contractingMedicare managed care contracting
Top six* issues for strategic gap:Top six* issues for strategic gap:
Controlling costsControlling costs Improving customer serviceImproving customer service Increasing patient satisfactionIncreasing patient satisfaction
Improving community health statusImproving community health statusMeasuring quality of care/improvingMeasuring quality of care/improvingoutcomesoutcomes
Medicare managed care contractingMedicare managed care contracting
*last three issues tied*last three issues tied
C
D E F G H
CE I D
CP MQ D R S E G IP R
T
G I E G D U
ID
S
eadership urvey 1999eadership urvey 1999
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
8/116
Financial Status 2000Financial Status 2000--20022002
V
W X Y ` a
b
X c W
b
d e f W g
SX ` h d g
S` c X ` W i h W S
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
9/116
0.2
2.8
0.
5.
1.1
8.5
1.
11.0
2.2
13.4
0
5
10
15
$
illion
1980 1990 1998 2004 2008
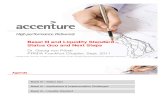
Health Care as a % of GDP
% Health Care% Health Care 8.9%8.9% 12.2%12.2% 13.5%13.5% 15.4%15.4% 16.2%16.2%
Health care is growingin dollar value and asHealth care is growingin dollar value and as
a percent of GDPa percent of GDP
Source: HCFA
Financial Status 2000Financial Status 2000--20022002Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
10/116
41.50%
18.30%
4.90%7.10%
28.20%
36.70%
20.90%
5.40%7.30%
29.70%
33.30%
20.00%
7.90%
7.60%
31.20%
31.40%
19.40%
9.90%
7.00%
32.20%
30.30%
19.10%
11.20%
6.90%
32.50%
1980 1990 1998 2004 2008
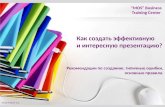
Distribution of Health Care Costs
Hospitals Physicians Drugs Long-Term Care Administration, Construction, Other
Source: HCFA
Hospitals are shrinking as a percentage ofHospitals are shrinking as a percentage of
the health care dollarthe health care dollar
Hospital($ Billions) $256 $103 $383 $531 $660
8.6 p
8.0%
11.3%
8.3%
6.9%
CompoundAnnual
Growth Rate
0%0%
20%20%
40%40%
60%60%
80%80%
100%100%
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
11/116
-10.0%
-8.0%
-6.0%
-4.0%
-2.0%
0.0%
2.0%
4.0%
1996 1997 1998 1999 2000 2001 2002
-10.0%
-8.0%
-6.0%
-4.0%
-2.0%
0.0%
2.0%
4.0%
1996 1997 1998 1999 2000 2001 2002
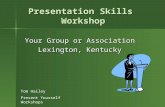
Urban All Hospitals Rural
Shrinking MarginsShrinking MarginsPayment cuts under the 1997 Balanced Budget Act will push hospital Medicare marginsPayment cuts under the 1997 Balanced Budget Act will push hospital Medicare marginson a downward slopeon a downward slope
Assuming costs grow at marketbasket,Assuming costs grow at marketbasket,Medicare margins for all hospitals willMedicare margins for all hospitals willdrop to negative 7.8% by 2002drop to negative 7.8% by 2002
if costs grow at marketbasket minusif costs grow at marketbasket minusone percentage point, margins will dropone percentage point, margins will dropto negative 4.4%.to negative 4.4%.
Post BBA-projections
ActualActual
Post BBA-projections
Source: The Lewin Group, May 1999
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
12/116
Summary of Key Findings - BBA
Total
Major Service Areas Studied
Inpatient PPS (operatingcapital, and bad debt)
Outpatient
Hospital-Based Home Health
PPS-Exempt Units andHospitals
-$71.2
-$40.7
-$11.2
-$5.5
-$2.8
-10.5%
-9.5%
-14.4%
-21.6%
-6.9%
-4.4%
7.5%
-20.3%
-11.4%
-4.7%
-7.8%
4.2%
-28.8%
-11.4%
-6.8%
5 YrPaymentImpact
(Billions)
5 YrPaymentImpact
(Percent)
2002 ProjectedMargin RangeDepending onCost Growth
Source: The Lewin Group analysis of Medicare Cost Report and AHA Annual Survey data.
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
13/116
45%
46%48%
55%57%
61%66%
68%70%
52% 54%
43% 39%34% 32% 30%
0% Medicare Margin
Percent ofHospitals withNegative Margins
Percent ofHospitals with
Positive Margins
Margins of Hospitals
1996 1997 1998 1999 2000 2001 20021995Source: The Lewin Group analysis of Medicare Cost Report and AHA Annual Survey data.
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
14/116
Balanced Budget Refinement Act of 1999Balanced Budget Refinement Act of 1999
Return total of $13.7 billion to MedicareReturn total of $13.7 billion to Medicarepaymentspayments
Represents only 12% of $115 billion BBA cutsRepresents only 12% of $115 billion BBA cuts
Only $7.5 billion of return goes to hospitalsOnly $7.5 billion of return goes to hospitals Improves Lewin hospital Medicare marginsImproves Lewin hospital Medicare margins
fromfrom --7.8% to7.8% to --6.9%6.9%
Balanced Budget Refinement Act of 1999Balanced Budget Refinement Act of 1999
Return total of $13.7 billion to MedicareReturn total of $13.7 billion to Medicarepaymentspayments
Represents only 12% of $115 billion BBA cutsRepresents only 12% of $115 billion BBA cuts
Only $7.5 billion of return goes to hospitalsOnly $7.5 billion of return goes to hospitals Improves Lewin hospital Medicare marginsImproves Lewin hospital Medicare margins
fromfrom --7.8% to7.8% to --6.9%6.9%
q
r
AL
s t
u
AR
r
u
OMv r w
x As
IOw
y
s
RAs r
Ir
x
Financial tatus 2000Financial tatus 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
15/116
Results of BBA thus far: Two years into the BBA,Results of BBA thus far: Two years into the BBA,and with the BBRA, the following has occurred:and with the BBRA, the following has occurred:
Four of largest nursing home chains, withFour of largest nursing home chains, withover 1,500 homes, have filed for bankruptcyover 1,500 homes, have filed for bankruptcy(Vencor, Sun Healthcare Group, Mariner Post(Vencor, Sun Healthcare Group, Mariner Post--Acute Network, Integrated Health Services).Acute Network, Integrated Health Services).10% of all nursing homes in bankruptcy.10% of all nursing homes in bankruptcy.
Fifth national chain misses bond payments; isFifth national chain misses bond payments; islikely bankruptcy candidatelikely bankruptcy candidate
648 home health agencies have shut down648 home health agencies have shut downsince 1997since 1997
Hospital margins, both operating and total,Hospital margins, both operating and total,are decreasing dramaticallyare decreasing dramatically
Results of BBA thus far: Two years into the BBA,Results of BBA thus far: Two years into the BBA,and with the BBRA, the following has occurred:and with the BBRA, the following has occurred:
Four of largest nursing home chains, withFour of largest nursing home chains, withover 1,500 homes, have filed for bankruptcyover 1,500 homes, have filed for bankruptcy(Vencor, Sun Healthcare Group, Mariner Post(Vencor, Sun Healthcare Group, Mariner Post--Acute Network, Integrated Health Services).Acute Network, Integrated Health Services).10% of all nursing homes in bankruptcy.10% of all nursing homes in bankruptcy.
Fifth national chain misses bond payments; isFifth national chain misses bond payments; islikely bankruptcy candidatelikely bankruptcy candidate
648 home health agencies have shut down648 home health agencies have shut downsince 1997since 1997
Hospital margins, both operating and total,Hospital margins, both operating and total,are decreasing dramaticallyare decreasing dramatically
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
16/116
Financial Status 2000Financial Status 2000--20022002Financial Status 2000Financial Status 2000--20022002
One In Ten Nursing Homes BankruptOne In Ten Nursing Homes BankruptOne In Ten Nursing Homes BankruptOne In Ten Nursing Homes Bankrupt
West14.9%
South14%
Midwest4.9%
Northeast6.7%
(Percentagebankrupt by
region)
Total U.S. 9.8%Source: American Health Care Association
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
17/116
Hospital Quarterly Operating Margins for 1998
0%
2%
3%
4%
5%
6%
7%
8% 7.94%
6.72%
6.38% 5.41%
4.15%3.78%
4.01%
2.60%
4.51%
3.87%
2.92%3.17%
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
0 to 99 Bed Facility 100 to 299 Bed Facility 300+ Bed Facility
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
18/116
4.5%
4.3%
4.9%
3.2%
2.0%
3.7%
-0.4%
0.5%
2.0%1.5%
3.1%
3.9%
-1%
0%
1%
2%
3%
4%
5%
1994 1995 1996 1997 1998 1999**
*Major teaching hospital indicated by membership in Council of Teaching Hospitals **EstimatedSource: HealthCare Advisory Board
NonNon--teaching hospitalsteaching hospitals
Major teaching hospitals*Major teaching hospitals*
In addition to absorbing standard reductions in Medicare payments, teaching hospitals also faceIn addition to absorbing standard reductions in Medicare payments, teaching hospitals also facesubstantial cuts in indirect medical education payments, and reductions in disproportionatesubstantial cuts in indirect medical education payments, and reductions in disproportionate--sharesharepayments.payments.
Operating margins in crisis
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
19/116
Hospital Total Margins(operating income plus investment income)
6.3%6.3%
4.3%4.3%
2.7%2.7%
1.1%1.1%
0
1
2
3
4
5
6
7
1997 1998 1999 2000 (est)
Financial Status 2000Financial Status 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
20/116
Tell me what you need, and Ill tell youTell me what you need, and Ill tell you
how to get along without it.how to get along without it.
Tell me what you need, and Ill tell youTell me what you need, and Ill tell you
how to get along without it.how to get along without it.
Dilberts Wisdom and Laws
T
TI
T
T
I
Financial tatus 2000Financial tatus 2000--20022002
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
21/116
Managed Care Plan StatusManaged Care Plan Status
C
C MP S
S S
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
22/116
10.9%10.9%199319936.6%6.6%
2.1%2.1%
2.2%2.2%2.1%2.1%
19951995
3.3%3.3%19971997
199919997.8%7.8%
Private HC PremiumsPrivate HC PremiumsHealth Care CostsHealth Care Costs
Managed Care PlansManaged Care PlansManaged Care PlansManaged Care Plans
Overall Percentage Change from Previous YearOverall Percentage Change from Previous Year
Source: VHA andDeloitte & Touche
5.7%5.7%
20002000 10.0%10.0%6.5%6.5%
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
23/116
Operating MarginsOperating Margins
19971997 57% of all HMOs reported losses57% of all HMOs reported losses
$768 million in total losses$768 million in total losses
Blue Cross plans had underwriting losses ofBlue Cross plans had underwriting losses of$790 million$790 million
19981998 56% of all HMOs reported losses56% of all HMOs reported losses
$490 million in total losses$490 million in total losses 45 of 55 Blue Cross plans had underwriting45 of 55 Blue Cross plans had underwriting
losses; total $835 millionlosses; total $835 million
Operating MarginsOperating Margins
19971997 57% of all HMOs reported losses57% of all HMOs reported losses
$768 million in total losses$768 million in total losses
Blue Cross plans had underwriting losses ofBlue Cross plans had underwriting losses of$790 million$790 million
19981998 56% of all HMOs reported losses56% of all HMOs reported losses
$490 million in total losses$490 million in total losses 45 of 55 Blue Cross plans had underwriting45 of 55 Blue Cross plans had underwriting
losses; total $835 millionlosses; total $835 million
Managed Care Plan StatusManaged Care Plan StatusManaged Care Plan StatusManaged Care Plan Status
H
j k l m
HC
k n j
COMPj o Sk m Oo
Sm n k m j j S
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
24/116
Comparison of HMO Profit Margins and Overall PercentComparison of HMO Profit Margins and Overall Percent
Increases in HMO PremiumsIncreases in HMO Premiums
Comparison of HMO Profit Margins and Overall PercentComparison of HMO Profit Margins and Overall Percent
Increases in HMO PremiumsIncreases in HMO Premiums
92 93 94 95 96 97 98 99
PercentPercentIncrease inIncrease in
OverallOverallPremiumsPremiums
HMO ProfitHMO ProfitMarginsMargins
Overall HealthOverall HealthInsurance PremiumsInsurance Premiums
HMO Profit MarginHMO Profit Margin
15%
10%
5%
0%
15%
10%
15%
10%
5%
0%
15%
10%
Managed Care Plan StatusManaged Care Plan StatusManaged Care Plan StatusManaged Care Plan Status
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
25/116
-2
10
12
14
Annual Percent ChangeAnnual Percent ChangeAnnual Percent ChangeAnnual Percent Change
0
2
4
6
8
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
HMO PremiumsHMO Premiums
General InflationGeneral Inflation
Source: KPMG Peat Marmick, Sherlock Company, Bureau of Labor Statistics
Managed Care Plan StatusManaged Care Plan StatusManaged Care Plan StatusManaged Care Plan Status
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
26/116
Shortage of ProfessionalsShortage of Professionals
z {
P |
S } z |
S ~ } S
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
27/116
US population age 30US population age 30 -- 44:44:
1999 = 64.3 million1999 = 64.3 million2003 = 62.3 million (2003 = 62.3 million (--3.2%)3.2%)2009 = 57.5 million (2009 = 57.5 million (--10.5%)10.5%)
Growth in US employment:Growth in US employment:Conservative estimates = +9.0% 1999 to 2009Conservative estimates = +9.0% 1999 to 2009Last two decades have had far greater growthLast two decades have had far greater growth
ratesrates
Conclusions:Conclusions:
20% shortfall in available prime20% shortfall in available prime--ofof--lifelifeemployees over next ten yearsemployees over next ten years
US population age 30US population age 30 -- 44:44:
1999 = 64.3 million1999 = 64.3 million2003 = 62.3 million (2003 = 62.3 million (--3.2%)3.2%)2009 = 57.5 million (2009 = 57.5 million (--10.5%)10.5%)
Growth in US employment:Growth in US employment:Conservative estimates = +9.0% 1999 to 2009Conservative estimates = +9.0% 1999 to 2009Last two decades have had far greater growthLast two decades have had far greater growth
ratesrates
Conclusions:Conclusions:
20% shortfall in available prime20% shortfall in available prime--ofof--lifelifeemployees over next ten yearsemployees over next ten years
Shortage of ProfessionalsShortage of ProfessionalsShortage of ProfessionalsShortage of Professionals
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
28/116
Health care delivery organizations not viewed asHealth care delivery organizations not viewed as
positively as employers, as in past decades:positively as employers, as in past decades: Evening, night, weekend, holiday schedules not asEvening, night, weekend, holiday schedules not asappealing to baby boomers who value lifeappealing to baby boomers who value lifestyle/work balancestyle/work balance
Alternative employment opportunities to use healthAlternative employment opportunities to use healthcare professional skills abound:care professional skills abound: Pharmaceutical firmsPharmaceutical firms
Medical supply companiesMedical supply companies
Medical device firmsMedical device firms
HMOs, managed care plansHMOs, managed care plans Consulting firmsConsulting firms
Equal/greater pay, better benefits, wealthEqual/greater pay, better benefits, wealthaccumulation, better life style, attractive featuresaccumulation, better life style, attractive featureselsewhereelsewhere
Health care delivery organizations not viewed asHealth care delivery organizations not viewed as
positively as employers, as in past decades:positively as employers, as in past decades: Evening, night, weekend, holiday schedules not asEvening, night, weekend, holiday schedules not asappealing to baby boomers who value lifeappealing to baby boomers who value lifestyle/work balancestyle/work balance
Alternative employment opportunities to use healthAlternative employment opportunities to use healthcare professional skills abound:care professional skills abound: Pharmaceutical firmsPharmaceutical firms
Medical supply companiesMedical supply companies
Medical device firmsMedical device firms
HMOs, managed care plansHMOs, managed care plans Consulting firmsConsulting firms
Equal/greater pay, better benefits, wealthEqual/greater pay, better benefits, wealthaccumulation, better life style, attractive featuresaccumulation, better life style, attractive featureselsewhereelsewhere
Shortage of ProfessionalsShortage of ProfessionalsShortage of ProfessionalsShortage of Professionals
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
29/116
AONE SurveyAONE Survey
Median age of R.N.s is 44 years; up from 38 tenMedian age of R.N.s is 44 years; up from 38 tenyears agoyears ago
Satisfaction downSatisfaction down----76% will remain in field;76% will remain in field;down from 86% ten years agodown from 86% ten years ago
Rigid hoursRigid hoursWorking conditions (staffing)Working conditions (staffing) Enrollment in fourEnrollment in four--year nursing programs downyear nursing programs down
AONE SurveyAONE Survey
Median age of R.N.s is 44 years; up from 38 tenMedian age of R.N.s is 44 years; up from 38 tenyears agoyears ago
Satisfaction downSatisfaction down----76% will remain in field;76% will remain in field;down from 86% ten years agodown from 86% ten years ago
Rigid hoursRigid hoursWorking conditions (staffing)Working conditions (staffing) Enrollment in fourEnrollment in four--year nursing programs downyear nursing programs down
E
E
E
E
E
hortage of rofessionalshortage of rofessionalshortage of rofessionalshortage of rofessionals
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
30/116
Other areas of shortage looming:Other areas of shortage looming:
Physical therapistsPhysical therapistsPharmacistsPharmacistsImaging TechnologistsImaging Technologists
Other areas of shortage looming:Other areas of shortage looming:
Physical therapistsPhysical therapistsPharmacistsPharmacistsImaging TechnologistsImaging Technologists
Source: AHA
T
P
TI
T
T
I
hortage of Professionalshortage of Professionalshortage of Professionalshortage of Professionals
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
31/116
Study by American Society of Health SystemStudy by American Society of Health SystemPharmacistsPharmacists
350 system directors polled350 system directors polled
50% reported vacancies50% reported vacanciesAverage open positions = 17%Average open positions = 17% National Association of Chain Drug StoresNational Association of Chain Drug Stores
Estimate 3,800 pharmacist vacanciesEstimate 3,800 pharmacist vacancies
Study by American Society of Health SystemStudy by American Society of Health SystemPharmacistsPharmacists
350 system directors polled350 system directors polled
50% reported vacancies50% reported vacanciesAverage open positions = 17%Average open positions = 17% National Association of Chain Drug StoresNational Association of Chain Drug Stores
Estimate 3,800 pharmacist vacanciesEstimate 3,800 pharmacist vacancies
Source: AHA
Environmental Assessment 2000Environmental Assessment 2000--20042004
Shortage of ProfessionalsShortage of Professionals
EA
A
E
PE
SA
S A E ES
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
32/116
Lack of investment in training and developmentLack of investment in training and development
American Society of Training andAmerican Society of Training andDevelopment 1998 surveyDevelopment 1998 surveyall industriesall industries All firms = $649/employee; 1.8% of payrollAll firms = $649/employee; 1.8% of payroll Leading edge firms = $1,966/employee;Leading edge firms = $1,966/employee;
4.4% of payroll4.4% of payroll Health care = $345/employee; 1.2% of payrollHealth care = $345/employee; 1.2% of payroll
Lack of investment in training and developmentLack of investment in training and development
American Society of Training andAmerican Society of Training andDevelopment 1998 surveyDevelopment 1998 surveyall industriesall industries All firms = $649/employee; 1.8% of payrollAll firms = $649/employee; 1.8% of payroll Leading edge firms = $1,966/employee;Leading edge firms = $1,966/employee;
4.4% of payroll4.4% of payroll Health care = $345/employee; 1.2% of payrollHealth care = $345/employee; 1.2% of payroll
H
AL
H
A
-
A -
A
hortage of rofessionalshortage of rofessionalshortage of rofessionalshortage of rofessionals
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
33/116
Current and Future Leadership in Health CareCurrent and Future Leadership in Health Care
H
L
H
C
C
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
34/116
The changing face of health care leadership:The changing face of health care leadership:attitudes and trends.attitudes and trends.The changing face of health care leadership:The changing face of health care leadership:attitudes and trends.attitudes and trends.
Current and Future Leadership in Health CareCurrent and Future Leadership in Health CareCurrent and Future Leadership in Health CareCurrent and Future Leadership in Health Care
John S. LloydJohn S. LloydVice ChairmanVice Chairman
Witt/Kieffer, Ford, Hadelman & LloydWitt/Kieffer, Ford, Hadelman & LloydACHEACHE
March 9, 1999March 9, 1999
HEALTHCA EC M E SAT
ST ATE ES
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
35/116
AESCAESC--Witt/Kieffer survey focuses on executivesWitt/Kieffer survey focuses on executives
opinionsopinionsInIn--depth interviews with current and futuredepth interviews with current and future
CEOs (Up & Comers health care leaders)CEOs (Up & Comers health care leaders)
Compared findings with comments fromCompared findings with comments fromFortune 1000 executivesFortune 1000 executives
AESCAESC--Witt/Kieffer survey focuses on executivesWitt/Kieffer survey focuses on executives
opinionsopinionsInIn--depth interviews with current and futuredepth interviews with current and future
CEOs (Up & Comers health care leaders)CEOs (Up & Comers health care leaders)
Compared findings with comments fromCompared findings with comments fromFortune 1000 executivesFortune 1000 executives
E C E
CO E IO
E
IE
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
36/116
CEOs expect short tenureCEOs expect short tenure
40% of health care CEOs expect shorter40% of health care CEOs expect shortertenures in the next 10 yearstenures in the next 10 years
But 69% of Fortune 1000 CEOs expect shorterBut 69% of Fortune 1000 CEOs expect shortertenurestenures
CEOs expect short tenureCEOs expect short tenure
40% of health care CEOs expect shorter40% of health care CEOs expect shortertenures in the next 10 yearstenures in the next 10 years
But 69% of Fortune 1000 CEOs expect shorterBut 69% of Fortune 1000 CEOs expect shortertenurestenures
E C E
CO E O
E
E
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
37/116
The portable CEO negatively affects loyalty toThe portable CEO negatively affects loyalty tothe organizationthe organization
2/3 or more of current health care CEOs agree2/3 or more of current health care CEOs agreeit has had a negative impact on loyaltyit has had a negative impact on loyalty
throughout corporate Americathroughout corporate America
The portable CEO negatively affects loyalty toThe portable CEO negatively affects loyalty tothe organizationthe organization
2/3 or more of current health care CEOs agree2/3 or more of current health care CEOs agreeit has had a negative impact on loyaltyit has had a negative impact on loyalty
throughout corporate Americathroughout corporate America
EA CA E
CO E
A
O
A
E
E
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
38/116
Future health care CEOs see opportunities inFuture health care CEOs see opportunities in
current positioncurrent positionHealth care: 55% of future CEOsHealth care: 55% of future CEOsFortune 1000: 57% of future CEOs expect theirFortune 1000: 57% of future CEOs expect their
opportunity will come elsewhere; 25% say in aopportunity will come elsewhere; 25% say in adifferent industrydifferent industry
Future health care CEOs see opportunities inFuture health care CEOs see opportunities in
current positioncurrent positionHealth care: 55% of future CEOsHealth care: 55% of future CEOsFortune 1000: 57% of future CEOs expect theirFortune 1000: 57% of future CEOs expect their
opportunity will come elsewhere; 25% say in aopportunity will come elsewhere; 25% say in adifferent industrydifferent industry
HE HC ECO
E
O
E
E
Current and Future eadership in Health CareCurrent and Future eadership in Health CareCurrent and Future eadership in Health CareCurrent and Future eadership in Health Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
39/116
Health care CEOs are less concerned aboutHealth care CEOs are less concerned aboutcompensationcompensation Health care CEOs are less concerned aboutHealth care CEOs are less concerned aboutcompensationcompensation
20%
27%
Say compensation causes high CEO turnoverSay compensation causes high CEO turnover
Current CEOsFuture CEOs
HE HC ECO
E
S
O
S E ES
Current and Future eadership in Health CareCurrent and Future eadership in Health CareCurrent and Future eadership in Health CareCurrent and Future eadership in Health Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
40/116
CEOs as mentorCEOs as mentor CEOs as mentorCEOs as mentor
100%
18% say current CEO is active in developing training
Current CEOsFuture CEOs
E C E
CO
E
O
E
E
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
41/116
Management training is lackingManagement training is lacking
But 100% of CEOs and 64% of future CEOs agree itBut 100% of CEOs and 64% of future CEOs agree itmakes sense to invest in training and developmentmakes sense to invest in training and development
Management training is lackingManagement training is lacking
But 100% of CEOs and 64% of future CEOs agree itBut 100% of CEOs and 64% of future CEOs agree itmakes sense to invest in training and developmentmakes sense to invest in training and development
90%
82%
Current CEOs
Future CEOs
E C E
COM
E
O
E!
E
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
42/116
Future health care CEOs need fastFuture health care CEOs need fast--tracktrackdevelopment programsdevelopment programs
But 50% of CEOs and 100% of future CEOs sayBut 50% of CEOs and 100% of future CEOs say
these programs dont existthese programs dont exist
Future health care CEOs need fastFuture health care CEOs need fast--tracktrackdevelopment programsdevelopment programs
But 50% of CEOs and 100% of future CEOs sayBut 50% of CEOs and 100% of future CEOs say
these programs dont existthese programs dont exist
90% agree
82% agree
Current CEOs
Future CEOs
"
E# $ % & C# ' E
CO( )
E0
1
# % 2
O0
3
% ' # %
E4
2
E1
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
43/116
Without training, finding qualified CEOs becomesWithout training, finding qualified CEOs becomesmore difficultmore difficult
Percent who say finding firstPercent who say finding first--rate CEOs willrate CEOs willbecome harder during the next ten yearsbecome harder during the next ten years
Without training, finding qualified CEOs becomesWithout training, finding qualified CEOs becomesmore difficultmore difficult
Percent who say finding firstPercent who say finding first--rate CEOs willrate CEOs willbecome harder during the next ten yearsbecome harder during the next ten years
% of future CEOswho agree
% of future CEOswho agree
9%9%
91%91%
60%60%
40%40%
Current and Future Leadership in Health CareCurrent and Future Leadership in Health CareCurrent and Future Leadership in Health CareCurrent and Future Leadership in Health Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
44/116
New CEOs will come from outside theNew CEOs will come from outside theorganizationorganization
But these new CEOs must have health careBut these new CEOs must have health careindustry experienceindustry experience
60%
82%
Current CEOs
Future CEOs
5
E6 7 8 9 C6 @ E
COA B
ENC6 8 D
ON
E
8 @ 6 8
EF
D
EC
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
45/116
Organizational flattening affects internal CEOOrganizational flattening affects internal CEOcandidate developmentcandidate development
Agree organizational flattening has a negativeAgree organizational flattening has a negativeeffect on internal CEO candidate developmenteffect on internal CEO candidate development
60%
64%
Current CEOs
Future CEOs
G
EAH I P CAQ E
COR S
ET
U AI V
OT
W
I Q
AI
EX
V
EU
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
46/116
Current CEOs rarely opt out, but future onesCurrent CEOs rarely opt out, but future onesmaymay
20%
64% say opting out willbecome more widespreadand a drain on talent
Current CEOs
Future CEOs
Y
E` a b c C` d E
COe f
Eg
h
` b i
Og
p
b d ` b
Eq
i
Eh
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
47/116
If CEOs leave, stress is the most likely reasonIf CEOs leave, stress is the most likely reason
Dealing with physicians and job burnout areDealing with physicians and job burnout areamong the factorsamong the factors
Pressure from shareholders contributes to CEOPressure from shareholders contributes to CEOturnoverturnover
r
Es t u v Cs w E
COx
PEy
s u
Oy
u w s u
E
E
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
48/116
Recognize factors contributing to stressRecognize factors contributing to stress
54% of CEOs in 1997 survey: stress has54% of CEOs in 1997 survey: stress hasincreased substantially in last five yearsincreased substantially in last five years
Only 34% say they achieve balance in theirOnly 34% say they achieve balance in their
personal livespersonal lives
E C E
CO
E
O
E
E
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
49/116
Find fun at workFind fun at work
Be a mentorBe a mentorChoose and train your successorChoose and train your successorFocus on the big pictureFocus on the big picture
Recognize exemplary performanceRecognize exemplary performanceTake a doc out to lunchTake a doc out to lunchVisit a patientVisit a patient
T C R
C
j
Tk
l TR
T
m
k
j
Current and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth CareCurrent and Future eadership in ealth Care
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
50/116
Find fun away from workFind fun away from work
Association workAssociation workGive something backGive something backAdvocacy programsAdvocacy programs
Education programsEducation programsBusiness travelBusiness travel
n
EAo
A
E
E
A
z
A
EG
E
urrent and Future eadership in ealth areurrent and Future eadership in ealth areurrent and Future eadership in ealth areurrent and Future eadership in ealth are
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
51/116
Health care is a circusHealth care is a circus
Why join the circus?Why join the circus? Be enchanted by the ability to perform theBe enchanted by the ability to perform the
impossibleimpossible
Ability to lift the human spiritAbility to lift the human spirit
Thrill to feats of courageThrill to feats of courage
{
|
A}
T~
A |
|
AT
T
AT|
|
urrent and Future eadership in ealth areurrent and Future eadership in ealth areurrent and Future eadership in ealth areurrent and Future eadership in ealth are
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
52/116
Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)
H H
R
P
I
R
I
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
53/116
Early IntegrationEarly Integration
Primary care physicians had many suitors withPrimary care physicians had many suitors withsome very attractive offerssome very attractive offers
Hospitals pursued strategies to affiliate withHospitals pursued strategies to affiliate with
PCPs for both offensive and defensive reasonsPCPs for both offensive and defensive reasons Keep physicians from joining a practiceKeep physicians from joining a practice
management company or competing hospitalmanagement company or competing hospital
Gain negotiating leverage against payersGain negotiating leverage against payers
Positioning to accept global capitationPositioning to accept global capitation Gain market share through a PCP networkGain market share through a PCP network
C
C
P
G
Physician ospital ntegration ( etain or Divest?)Physician ospital ntegration ( etain or Divest?)Physician ospital ntegration ( etain or Divest?)Physician ospital ntegration ( etain or Divest?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
54/116
Top ten common hospital mistakesTop ten common hospital mistakes
1. High guaranteed salaries, no incentive to continue to work1. High guaranteed salaries, no incentive to continue to work2. Hospital signs bad managed care contracts2. Hospital signs bad managed care contracts3. Hospital business office does billing for physicians3. Hospital business office does billing for physicians4. Removed ancillaries from practices4. Removed ancillaries from practices
5. Excess plant capacity5. Excess plant capacity--Hired too many new physiciansHired too many new physicians6. Dont worry well manage your practice6. Dont worry well manage your practice7. Poor physician governance structure7. Poor physician governance structure8. Amortized the cost of the practice back to the network8. Amortized the cost of the practice back to the network9. Employees are provided with hospital salaries and benefits9. Employees are provided with hospital salaries and benefits10. Paid too much for the practice10. Paid too much for the practice
HEA TH
ARE
PE
AT
TRATE
E
Physician Hospital ntegration (Retain or Divest?)Physician Hospital ntegration (Retain or Divest?)Physician Hospital ntegration (Retain or Divest?)Physician Hospital ntegration (Retain or Divest?)
h l ( )h l ( )h l ( )h l ( )
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
55/116
< $25,000
17%N L ss
16%
>$100,00014%
$75,0001 -
$100,000
14%
$50,001 -
$75,000
16%
$25,001 -$50,000
19%N/A
4%
Percentage of Hospitals Reporting Losseson Physician Practices (per PCP)
Source: Health Care Advisory Board 1999
HEALTHCARE
COMPENSATION
STRATEGIES
PhysicianHospital Integration (Retain or Divest?)PhysicianHospital Integration (Retain or Divest?)PhysicianHospital Integration (Retain or Divest?)PhysicianHospital Integration (Retain or Divest?)
h i i i l i ( i i )h i i i l i ( i i )h i i i l i ( i i )h i i i l i ( i i )
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
56/116
35%
60%
5%
Considering Divesting
Keeping Practice
Divesting
InformalSurvey ofMembers (1999)InformalSurvey ofMembers (1999)InformalSurvey ofMembers (1999)InformalSurvey ofMembers (1999)
Source: Health Care Advisory Board 1999
Physician HospitalIntegration (Retain or Divest?)Physician HospitalIntegration (Retain or Divest?)Physician HospitalIntegration (Retain or Divest?)Physician HospitalIntegration (Retain or Divest?)
Ph i i H i l I i (R i Di ?)Ph i i H i l I i (R i Di ?)Ph i i H i l I i (R i Di ?)Ph i i H i l I i (R i Di ?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
57/116
Retain or Divest?Retain or Divest?
Review initial strategy and current marketReview initial strategy and current marketconditioncondition
Review physician employment contractsReview physician employment contracts
Assess legal and political climateAssess legal and political climatePrimary networkPrimary network ---- assess impact onassess impact onspecialistsspecialists
Assess impact on hospital core programsAssess impact on hospital core programs
Retain or Divest?Retain or Divest?
Review initial strategy and current marketReview initial strategy and current marketconditioncondition
Review physician employment contractsReview physician employment contracts
Assess legal and political climateAssess legal and political climatePrimary networkPrimary network ---- assess impact onassess impact onspecialistsspecialists
Assess impact on hospital core programsAssess impact on hospital core programs
HEALTHCARE
COMPENSATION
STRATEGIES
PhysicianHospital Integration (Retain or Divest?)PhysicianHospital Integration (Retain or Divest?)PhysicianHospital Integration (Retain or Divest?)PhysicianHospital Integration (Retain or Divest?)
Ph i i H i l I i (R i Di ?)Ph i i H i l I i (R i Di ?)Ph i i H i l I i (R i Di ?)Ph i i H i l I i (R i Di ?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
58/116
Organization merit
bankable credit? Central to y tem
trategy Self perpetuating
organizational tructurewitha proven trackrecord and ufficient
ize? Economic model with
ufficientreturn tore erve forfutureuncertainty?
NO
YES
Source: Financing Sustainable Physician Organizations Tiber Group; February 9, 1999Source: Financing Sustainable Physician Organizations Tiber Group; February 9, 1999
Decision Rules for the FutureDecision Rules for the Futureof the Employed Medical Groupof the Employed Medical Group
Decision Rules for the FutureDecision Rules for the Futureof the Employed Medical Groupof the Employed Medical Group
INVESTINVEST
everage the strategiceverage the strategicbenefits ofbenefits of
the organization by using itthe organization by using itasabasis for futureasabasis for future
financingfinancingand growthand growth
Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)
Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
59/116
Do we have theresourcesand
commitmentto turnthe cornerfinancially?
EVOLVEEVOLVE
Implement financialImplement financialrestructuringrestructuring
Considersecond generationConsidersecond generationmodelsmodelsJoint Ventures/JointJoint Ventures/Joint
OperatingagreementsOperatingagreements
Management/FranchiseManagement/Franchise
AgreementsAgreementsMasterMaster--AffiliationAffiliation
AgreementsAgreements
CarveCarve--Outs/CarveOuts/Carve--InsIns
Venture CapitalVenture Capital
CorporationsCorporations
YES
Decision Rules for the FutureDecision Rules for the Future
of the Employed Medical Groupof the Employed Medical Group
Decision Rules for the FutureDecision Rules for the Future
of the Employed Medical Groupof the Employed Medical Group
NO
Source: Financing Sustainable Physician Organizations Tiber Group; February 9, 1999Source: Financing Sustainable Physician Organizations Tiber Group; February 9, 1999
Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)
Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
60/116
Isthe market safeto
turn the physiciansloose?
No cherry pickingby newcompetitors
No shiftto rival
hospitals
No physician
activism
DIVESTDIVEST
SpinSpin--offsome oroffsome orall ofthe physiciansall ofthe physicians
YES
NO
RETAIN, but make tough financial decisions.RETAIN, but make tough financial decisions.
Decision Rules for the FutureDecision Rules for the Future
of the Employed Medical Groupof the Employed Medical Group
Decision Rules for the FutureDecision Rules for the Future
of the Employed Medical Groupof the Employed Medical Group
Source: Financing Sustainable Physician Organizations Tiber Group; February 9, 1999Source: Financing Sustainable Physician Organizations Tiber Group; February 9, 1999
Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)
Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
61/116
Six key steps to follow:Six key steps to follow:
ReRe--assess organizational structure, managementassess organizational structure, managementmodelmodelEvaluate physician governance/medicalEvaluate physician governance/medical
leadershipleadership
Financial assessment of the practice to developFinancial assessment of the practice to developappropriate benchmarksappropriate benchmarksEvaluate physician staffingEvaluate physician staffingReinforce physician performance withReinforce physician performance with
compensationcompensationProvide performance reports and holdProvide performance reports and holdphysicians accountablephysicians accountable
Six key steps to follow:Six key steps to follow:
ReRe--assess organizational structure, managementassess organizational structure, managementmodelmodelEvaluate physician governance/medicalEvaluate physician governance/medical
leadershipleadership
Financial assessment of the practice to developFinancial assessment of the practice to developappropriate benchmarksappropriate benchmarksEvaluate physician staffingEvaluate physician staffingReinforce physician performance withReinforce physician performance with
compensationcompensationProvide performance reports and holdProvide performance reports and holdphysicians accountablephysicians accountable
Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)
HEALTHCARE
COMPENSATIONSTRATEGIES
Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)Ph i i H it l I t ti (R t i Di t?)
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
62/116
Divestiture process (key issues)Divestiture process (key issues)
Analyze employment contractsAnalyze employment contractsBuyBuy--out of remaining term (Economic Harm)out of remaining term (Economic Harm)Use of severance paymentsUse of severance paymentsAssess impact on nonAssess impact on non--physician employeesphysician employeesMethod for transfer of practices tangibleMethod for transfer of practices tangible
assetsassetsCoordinate divestiture process with legalCoordinate divestiture process with legal
counselcounsel
Evaluate impact to physician medical staffEvaluate impact to physician medical staffManage public relationsManage public relations
Divestiture process (key issues)Divestiture process (key issues)
Analyze employment contractsAnalyze employment contractsBuyBuy--out of remaining term (Economic Harm)out of remaining term (Economic Harm)Use of severance paymentsUse of severance paymentsAssess impact on nonAssess impact on non--physician employeesphysician employeesMethod for transfer of practices tangibleMethod for transfer of practices tangible
assetsassetsCoordinate divestiture process with legalCoordinate divestiture process with legal
counselcounsel
Evaluate impact to physician medical staffEvaluate impact to physician medical staffManage public relationsManage public relations
Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)Physician Hospital Integration (Retain or Divest?)
HEALTHCARE
COMPENSATIONSTRATEGIES
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
63/116
Credit CrunchCredit Crunch
HEALTHCARE
COMPENSATIONSTRATEGIES
C dit C hC dit C hC dit C hC dit C h
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
64/116
Leaders surveyLeaders survey
Phoenix Management ServicesPhoenix Management Services95 major leading organizations95 major leading organizations85% unwilling to lend to health care85% unwilling to lend to health care
industry; up from 69% and 55% in twoindustry; up from 69% and 55% in twoprevious quartersprevious quarters
Lowest rating of an industry in history orLowest rating of an industry in history orsurveysurvey
Leaders surveyLeaders survey
Phoenix Management ServicesPhoenix Management Services95 major leading organizations95 major leading organizations85% unwilling to lend to health care85% unwilling to lend to health care
industry; up from 69% and 55% in twoindustry; up from 69% and 55% in twoprevious quartersprevious quarters
Lowest rating of an industry in history orLowest rating of an industry in history orsurveysurvey
HEALTHCARE
COMPENSATIONSTRATEGIES
Credit CrunchCredit CrunchCredit CrunchCredit Crunch
C dit C hC dit C hC dit C hC dit C h
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
65/116
Moodys 2000 Credit ReportMoodys 2000 Credit Report
1999 downgrades affect $13.4 billion; upgrades1999 downgrades affect $13.4 billion; upgradesaffect $1.7 billionaffect $1.7 billion
Moodys 2000 Credit ReportMoodys 2000 Credit Report
1999 downgrades affect $13.4 billion; upgrades1999 downgrades affect $13.4 billion; upgradesaffect $1.7 billionaffect $1.7 billion
80
010
20
30
40
5060
70
90
100
1997 1998 1999
Downgrades Upgrades
Credit CrunchCredit CrunchCredit CrunchCredit Crunch
Credit CrunchCredit CrunchCredit CrunchCredit Crunch
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
66/116
Zimmerman & Associates study, February 2000Zimmerman & Associates study, February 2000
Hospitals bad debts equal $30 billionHospitals bad debts equal $30 billionHospitals aggregate operating profits equalHospitals aggregate operating profits equal
$10 billion$10 billion
20% of net revenues come from private pay; up20% of net revenues come from private pay; upfrom 10% ten years ago due to deductibles andfrom 10% ten years ago due to deductibles andallowancesallowances
Zimmerman & Associates study, February 2000Zimmerman & Associates study, February 2000
Hospitals bad debts equal $30 billionHospitals bad debts equal $30 billionHospitals aggregate operating profits equalHospitals aggregate operating profits equal
$10 billion$10 billion
20% of net revenues come from private pay; up20% of net revenues come from private pay; upfrom 10% ten years ago due to deductibles andfrom 10% ten years ago due to deductibles andallowancesallowances
HEALTHCARE
COMPENSATIONSTRATEGIES
Credit CrunchCredit CrunchCredit CrunchCredit Crunch
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
67/116
CRITICAL SUCCESS FACTORSCRITICAL SUCCESS FACTORS
HEALTHCARE
COMPENSATIONSTRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
68/116
If at first you dont succeed, try again.If at first you dont succeed, try again.Then quit. No sense being a damn foolThen quit. No sense being a damn foolabout it.about it.
If at first you dont succeed, try again.If at first you dont succeed, try again.Then quit. No sense being a damn foolThen quit. No sense being a damn foolabout it.about it.
Dilberts Wisdom and Laws
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
HEALTHCARE
COMPENSATIONSTRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
69/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
ReRe--establish trust with key stakeholdersestablish trust with key stakeholders
Visibly educate communities/leaders aboutVisibly educate communities/leaders abouthealth care industrys issues/problemshealth care industrys issues/problems
Actively participate in patient/consumerActively participate in patient/consumeradvocacy issue groups; e.g., service health,advocacy issue groups; e.g., service health,womens health, uninsuredwomens health, uninsured
All parts of the system need to participate;All parts of the system need to participate;Board members, physicians, nurses,Board members, physicians, nurses,technicians, managers, . . . everyonetechnicians, managers, . . . everyone
ReRe--establish trust with key stakeholdersestablish trust with key stakeholders
Visibly educate communities/leaders aboutVisibly educate communities/leaders abouthealth care industrys issues/problemshealth care industrys issues/problems
Actively participate in patient/consumerActively participate in patient/consumeradvocacy issue groups; e.g., service health,advocacy issue groups; e.g., service health,womens health, uninsuredwomens health, uninsured
All parts of the system need to participate;All parts of the system need to participate;Board members, physicians, nurses,Board members, physicians, nurses,technicians, managers, . . . everyonetechnicians, managers, . . . everyone
HEALTHCARE
COMPENSATIONSTRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
70/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Engage every employee in our solutionsEngage every employee in our solutions
Investment in training, education, andInvestment in training, education, andhuman resource development as a corehuman resource development as a corestrategystrategy
Dollars spent on retention may be moreDollars spent on retention may be moreeconomical than recruitingeconomical than recruiting
A sense of commitment felt by employeesA sense of commitment felt by employeesgenerates greater loyalty than any othergenerates greater loyalty than any otherfactorfactor
Engage every employee in our solutionsEngage every employee in our solutions
Investment in training, education, andInvestment in training, education, andhuman resource development as a corehuman resource development as a corestrategystrategy
Dollars spent on retention may be moreDollars spent on retention may be moreeconomical than recruitingeconomical than recruiting
A sense of commitment felt by employeesA sense of commitment felt by employeesgenerates greater loyalty than any othergenerates greater loyalty than any otherfactorfactor
HEALTHCARE
COMPENSATIONSTRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
71/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Make an extraordinary commitment toMake an extraordinary commitment to
innovationinnovationCase managementCase managementClaims managementClaims management
Complementary managementComplementary management
Disease managementDisease managementHealth risk assessmentsHealth risk assessmentsPhysician practice managementPhysician practice management
Hospitals/systems have not masteredHospitals/systems have not masteredany/many of theseany/many of theseBiotechnology is next new areaBiotechnology is next new area
Make an extraordinary commitment toMake an extraordinary commitment to
innovationinnovationCase managementCase managementClaims managementClaims management
Complementary managementComplementary management
Disease managementDisease managementHealth risk assessmentsHealth risk assessmentsPhysician practice managementPhysician practice management
Hospitals/systems have not masteredHospitals/systems have not masteredany/many of theseany/many of theseBiotechnology is next new areaBiotechnology is next new area
HEALTHCARE
COMPENSATIONSTRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
72/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Develop ability to coordinate care across theDevelop ability to coordinate care across the
continuumcontinuumSystems linkages to physician networks withSystems linkages to physician networks with
strong physician governance, management,strong physician governance, management,and ownershipand ownership
Risk sharingRisk sharingJoint ownership/management of servicesJoint ownership/management of services
Develop ability to coordinate care across theDevelop ability to coordinate care across the
continuumcontinuumSystems linkages to physician networks withSystems linkages to physician networks with
strong physician governance, management,strong physician governance, management,and ownershipand ownership
Risk sharingRisk sharingJoint ownership/management of servicesJoint ownership/management of services
HEALTHCARE
COMPENSATIONSTRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
73/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Focus on operations managementFocus on operations management
Costs, productivity, and qualityCosts, productivity, and qualityBenchmark against top 10% of systemsBenchmark against top 10% of systemsMultidisciplinary team approachMultidisciplinary team approach
Use experts to assistUse experts to assist Example of revenue cycle reExample of revenue cycle re--engineeringengineering
Focus on operations managementFocus on operations management
Costs, productivity, and qualityCosts, productivity, and qualityBenchmark against top 10% of systemsBenchmark against top 10% of systemsMultidisciplinary team approachMultidisciplinary team approach
Use experts to assistUse experts to assist Example of revenue cycle reExample of revenue cycle re--engineeringengineering
HEALTHCARE
COMPENSATIONSTRATEGIES
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
74/116
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
75/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
76/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Organization AnnualRevenue
AnnualIncome
Improvement
inancialBenefit toDate
niversity of California-Davis, CA
$1.6 billion $10 million $55 million
Vanderbilt niversityHospital and Clinic-
ashville, T
$550 million $9 million $40 million
Baystate Health Systems-Springfield, MA
$550 million $9 million $40 million
Providence Health
System-Portland, OR
$1 billion $3 million $8 million
Cedars-Sinai MedicalCenter-Los Angeles, CA
$1.3 billion $14 million $45 million
St. Josephs Hospital-Atlanta, GA
$350 million $10 million $35 million
Source: Stockamp & Associates, Inc.- References
Revenue Cycle ReRevenue Cycle Re--engineeringengineering
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
77/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Organization Annual
Revenue
Annual
IncomeImprovement
inancial
Benefit toDate
niversity of California-IrvineCA
$450 million $6 million $22 million
Oregon Health Sciencesniversity-Portland, OR
$400 million $6 million $27 million
Santa Clara Valley MedicalCenter-San Jose, CA
600 million $6 million $22 million
CS Stanford Health Care-CS Medical Center
$1.4 billion $7 million 39 million
niversity of Kansas Medical
Center-Kansas City, KS
350 million $7 million $22 million
Source: Stockamp & Associates, Inc.- References
HEALTHCARE
COMPENSATIONSTRATEGIES
Revenue Cycle ReRevenue Cycle Re--engineeringengineering
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
78/116
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Source: Stockamp & Associates Recent Project Highlights
roject Sco e
B C
roject
i e Fra e Jul 98 to
a 99 Ju 98 to
a 99 Ja 99 to
o 99
ec 98 to Se 99
ar 99 to Se 99
ri i al Be efit
rojectio sI co e State e t $4
to $6M $4 to $6M $6M to $8M $3M to $8MBala ce S
eet $11M to $16M $20M to 25M $25M to $35M $8M to $16M
B
ilot
ual I co e State e tI ro e e t $8M $7M $8M $6M $2M to $3M est.
First
ear Cas
Flo
I ro e e t $25M $32M $25M $15M 12
i crease i
. Mo t
l
Cas
erall Cas
Be efits o er 5- ear erio
$65M $80M $60M $45M $15M to $25M est
/
e
uctio 24
21
20
17
36
U bille
or
-i -
ro ress
e
uctio 90
64
70
75
42
e e ue C cle ee e ue C cle e--e i eerie i eeri
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
79/116
Analysis ObjectiveAnalysis ObjectiveTo assess the effectiveness of billing andTo assess the effectiveness of billing and
collection activitiescollection activities
Sample SizeSample SizeApproximately 150 accounts greater than 90 daysApproximately 150 accounts greater than 90 days
from dischargefrom discharge
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
HEALTHCARE
COMPENSATIONSTRATEGIES
Revenue Cycle ReRevenue Cycle Re--engineeringengineering---- AccountAccount
FollowFollow--up Sampling Analysisup Sampling Analysis
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
80/116
Summary FindingsSummary Findings
No or little followNo or little follow--up occurring on majority ofup occurring on majority ofoutstanding A/Routstanding A/R
FollowFollow--up frequencyup frequency
83% of A/R balance reviewed had no or randomly83% of A/R balance reviewed had no or randomlydocumented followdocumented follow--upup
12% of A/R balance reviewed had regular but no12% of A/R balance reviewed had regular but notimely followtimely follow--upup
Quality and effectiveness of followQuality and effectiveness of follow--upup
74% of A/R balance reviewed had no or reactive and74% of A/R balance reviewed had no or reactive andineffective followineffective follow--upup
19% of A/R balance reviewed had proactive but19% of A/R balance reviewed had proactive butineffective followineffective follow--upup
7% of A/R balance reviewed had proactive and7% of A/R balance reviewed had proactive andeffective followeffective follow--upup
Summary FindingsSummary Findings
No or little followNo or little follow--up occurring on majority ofup occurring on majority ofoutstanding A/Routstanding A/R
FollowFollow--up frequencyup frequency
83% of A/R balance reviewed had no or randomly83% of A/R balance reviewed had no or randomlydocumented followdocumented follow--upup
12% of A/R balance reviewed had regular but no12% of A/R balance reviewed had regular but notimely followtimely follow--upup
Quality and effectiveness of followQuality and effectiveness of follow--upup
74% of A/R balance reviewed had no or reactive and74% of A/R balance reviewed had no or reactive andineffective followineffective follow--upup
19% of A/R balance reviewed had proactive but19% of A/R balance reviewed had proactive butineffective followineffective follow--upup
7% of A/R balance reviewed had proactive and7% of A/R balance reviewed had proactive andeffective followeffective follow--upup
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----AccountAccount
FollowFollow--up Sampling Analysisup Sampling Analysis
Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
81/116
Summary Findings (contd)Summary Findings (contd)
Account documentation and activity does notAccount documentation and activity does notsupport effective management and followsupport effective management and follow--upup
Lack of standard followLack of standard follow--up procedures andup procedures andguidelines in placeguidelines in place Appears highly probable that numerousAppears highly probable that numerous
accounts were adjusted and/or written off toaccounts were adjusted and/or written off tocontractual allowances rather than bad debt,contractual allowances rather than bad debt,administrative and charity writeadministrative and charity write--off categoriesoff categories
Summary Findings (contd)Summary Findings (contd)
Account documentation and activity does notAccount documentation and activity does notsupport effective management and followsupport effective management and follow--upup
Lack of standard followLack of standard follow--up procedures andup procedures andguidelines in placeguidelines in place Appears highly probable that numerousAppears highly probable that numerous
accounts were adjusted and/or written off toaccounts were adjusted and/or written off tocontractual allowances rather than bad debt,contractual allowances rather than bad debt,administrative and charity writeadministrative and charity write--off categoriesoff categories
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
HEALTHCARE
COMPENSATIONSTRATEGIES
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----AccountAccount
FollowFollow--up Sampling Analysisup Sampling Analysis
Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
82/116
Representative ExamplesRepresentative Examples Representative ExamplesRepresentative Examples
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
$481,675
$463,549
$405,721
$232,357$206,918
$157,020
$127,931
$117,066
$104,735
$65,371$58,349
$21,878
$20,163
$10,485
$9,209
134
267
288
124159
139
338
162
115
274281
309
177
153
348
o follow-up since initial follow-up to bill pro fee
Billed timely, no follow-up activity
Rebilled after first bill to Medicare, no follow-up
Rebilled 112 days after first bill to Medicare, no follow-upMedicare denied for overlap, no follow-up for 156 days
Billed 48 days post discharge, one follow-up in 90 days
Billed 15 days post discharge, one follow-up in 180 days
Billed 30 days post discharge, no follow-up
Billed 15 days post discharge, no follow-up
Billed 90 days post discharge, no follow-upMedicare; overlap with S ; no follow-up for 90+ days
Billed 20 days post discharge, no follow-up
Billed 60 days post discharge, billed to wrong payer, no rebill
Blue Cross, no follow-up
Billed, new payer found 279 days later, no follow-up
Total ChargesDays fromDischarge Findings
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Account FollowAccount Follow--upupSampling AnalysisSampling Analysis
Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
83/116
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt,Bad Debt,
Administrative and Charity WriteAdministrative and Charity Write--off Samplingoff SamplingAnalysisAnalysis
Analysis ObjectiveAnalysis Objective
To assess whether overall writeTo assess whether overall write--off levels canoff levels canbe reduced in the areas of bad debt,be reduced in the areas of bad debt,administrative and charity writeadministrative and charity write--offoffcategoriescategories
Sample SizeSample Size
Approximately 175 accounts written off toApproximately 175 accounts written off torepresentative transaction codesrepresentative transaction codes
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt,Bad Debt,
Administrative and Charity WriteAdministrative and Charity Write--off Samplingoff SamplingAnalysisAnalysis
Analysis ObjectiveAnalysis Objective
To assess whether overall writeTo assess whether overall write--off levels canoff levels canbe reduced in the areas of bad debt,be reduced in the areas of bad debt,administrative and charity writeadministrative and charity write--offoffcategoriescategories
Sample SizeSample Size
Approximately 175 accounts written off toApproximately 175 accounts written off torepresentative transaction codesrepresentative transaction codes
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
HEALTHCARE
COMPENSATIONSTRATEGIES Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
84/116
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt,Bad Debt,Administrative and Charity WriteAdministrative and Charity Write--off Samplingoff SamplingAnalysisAnalysis
Summary FindingsSummary Findings Probability of preventable writeProbability of preventable write--offsoffs
41% of write41% of write--off amounts review wereoff amounts review were
preventable with better processes andpreventable with better processes andcontrolscontrols
39% of write39% of write--off amounts reviewed mayoff amounts reviewed mayhave been prevented with better processeshave been prevented with better processes
and controlsand controls 20% of write20% of write--off amounts reviewed appearedoff amounts reviewed appeared
appropriate, but unclear due to lack ofappropriate, but unclear due to lack ofdocumentationdocumentation
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt,Bad Debt,Administrative and Charity WriteAdministrative and Charity Write--off Samplingoff SamplingAnalysisAnalysis
Summary FindingsSummary Findings Probability of preventable writeProbability of preventable write--offsoffs
41% of write41% of write--off amounts review wereoff amounts review were
preventable with better processes andpreventable with better processes andcontrolscontrols
39% of write39% of write--off amounts reviewed mayoff amounts reviewed mayhave been prevented with better processeshave been prevented with better processes
and controlsand controls 20% of write20% of write--off amounts reviewed appearedoff amounts reviewed appeared
appropriate, but unclear due to lack ofappropriate, but unclear due to lack ofdocumentationdocumentation
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
85/116
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt,Bad Debt,Administrative and Charity WriteAdministrative and Charity Write--off Samplingoff Sampling
AnalysisAnalysis Summary Findings (contd)Summary Findings (contd)
Areas of writeAreas of write--off preventionoff prevention 48% of accounts required better quality and48% of accounts required better quality and
more timely followmore timely follow--up by financial counselingup by financial counseling 16% of write16% of write--offs sampled were related tooffs sampled were related to
absent or late checking of patient benefitsabsent or late checking of patient benefits
Majority of accounts were poorly documentedMajority of accounts were poorly documentedpreventing effective followpreventing effective follow--up to take placeup to take place
Patient payment plans were rarely initiated, inPatient payment plans were rarely initiated, inelective cases where patients made oneelective cases where patients made onepayment (less than 20% of charges), thepayment (less than 20% of charges), theaccounts were written off immediatelyaccounts were written off immediately
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt,Bad Debt,Administrative and Charity WriteAdministrative and Charity Write--off Samplingoff Sampling
AnalysisAnalysis Summary Findings (contd)Summary Findings (contd)
Areas of writeAreas of write--off preventionoff prevention 48% of accounts required better quality and48% of accounts required better quality and
more timely followmore timely follow--up by financial counselingup by financial counseling 16% of write16% of write--offs sampled were related tooffs sampled were related to
absent or late checking of patient benefitsabsent or late checking of patient benefits
Majority of accounts were poorly documentedMajority of accounts were poorly documentedpreventing effective followpreventing effective follow--up to take placeup to take place
Patient payment plans were rarely initiated, inPatient payment plans were rarely initiated, inelective cases where patients made oneelective cases where patients made onepayment (less than 20% of charges), thepayment (less than 20% of charges), theaccounts were written off immediatelyaccounts were written off immediately
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
86/116
Representative ExamplesRepresentative Examples
$75,732
$61,834$55,360
$46,921
$40,886
$34,176
$34,212
$27,345
$23,376$22,514
$21,595
$20,169
235
33281
189
391
270
330
240
364174
261
310
Inpatient service coded four months post discharge, denied for timely filing
Slow application process, Medicaid granted, billed 90 days later, no follow-upSlow financial counseling follow-up, billing delays
o follow-up on Medicaid eligibility for over four months
Poor collection of patient information, no verification, no follow-up
Insurance eligibility check during visit but no follow-up, billed four months post disch.
Auth. or Medicaid 150 days post discharge, no follow-up, no pay for seven months
o verification, denied for no benefits remaining, no follow-up
Denied for no pre-cert; no appeal attempts even though auth. attempt documented
Elective referral; admitted without pre-auth; eventually approved for charity w/o
o verification, denied for no benefits remaining
o screening, no collection of patient deposit, no follow-up
TotalCharges
Daysfrom
Discharge Findings
Source: Stockamp & Associates
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----Bad Debt, AdministrativeBad Debt, Administrativeand Charity Writeand Charity Write--off Sampling Analysisoff Sampling Analysis
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
87/116
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----ContractualContractual
Allowance Sampling AnalysisAllowance Sampling Analysis Analysis ObjectiveAnalysis Objective
To assess if contractual allowance writeTo assess if contractual allowance write--offofflevels can be reduced by determining iflevels can be reduced by determining ifavoidable, administrative writeavoidable, administrative write--offs areoffs arebeing classified inappropriatelybeing classified inappropriately
Sample SizeSample Size
Approximately 150 accountsApproximately 150 accounts
HEALTHCARE
COMPEN
SATION
STRATEGIES Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
88/116
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----ContractualContractual
Allowance Sampling Analysis (Contd)Allowance Sampling Analysis (Contd) Summary FindingsSummary Findings
Numerous accounts were immediately reducedNumerous accounts were immediately reducedto a zero balance once a zero payment wasto a zero balance once a zero payment was
received by the payerreceived by the payer Significant improvement opportunities forSignificant improvement opportunities for
accounts written off to bad debt, administrativeaccounts written off to bad debt, administrativeand charity writeand charity write--off codes, as well as misoff codes, as well as mis--
classified contractual allowancesclassified contractual allowances Majority of accounts lacked documentation toMajority of accounts lacked documentation tosupport any type of write offssupport any type of write offs
Clear that many of these writeClear that many of these write--offs are avoidableoffs are avoidableHEALTHCARE
CO
MPE
NSATIO
NSTRATEGIES Source: Stockamp & Associates
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
89/116
Revenue Cycle ReRevenue Cycle Re--engineeringengineering----ContractualContractualAllowance SamplingAllowance Sampling
Representative ExamplesRepresentative Examples
$25,728
$24,518$21,733
$18,723
$17,354
$12,751
$12,020
$10,891$9,322
$4,802
61
72228
24
87
323
28
16947
60
HMO claim denied for timely filing; balance written off to provider contractual
Medicaid application filed, no follow-up, w/o to Medicaid denialo authorization on elective service, denied, w/o to Medicaid denial
Payer denied for no authorization, total charges to contractual
Blue Cross denied for no pre-cert, written off to denial appeal
Account written off to C/A, later approved for Medicaid, Medicaid never billed
Zero payment received from managed care plan, total charges w/o to contractual
Medicaid rejected as non-covered service, entire balance to Medicaid contractualPatient eventually approved for Medicaid, Medicaid never billed, w/o to contractual
HMO payer denied for no pre-cert, account written off to payer contractual
TotalCharges
Daysfrom
Discharge Findings
Source: Stockamp & Associates
HEALTHCARE
COMPENSA
TION
STRATEGIES
Critical Success FactorsCritical Success FactorsCritical Success FactorsCritical Success Factors
-
8/8/2019 Scottsdale Instit Presentation- Wegmiller
90/116
Achieve a certain critical mass and geographicAchieve a certain critical mass and geographic
reach to effectively achieve the first five factorsreach to effectively achieve the first five factorsMarket share and capital access are crucial toMarket