Sistemas de Soporte a la decisión Clínica Luis...
32
Sistemas Sistemas de de Soporte Soporte a la a la decisión decisión Clínica Clínica (SSDC (SSDC) Sistemas Sistemas de de Soporte Soporte a la a la decisión decisión Clínica Clínica (SSDC (SSDC) Dr. Dr. Lluís Lluís Donoso Donoso Bach Bach Dr. Dr. Lluís Lluís Donoso Donoso Bach Bach
Transcript of Sistemas de Soporte a la decisión Clínica Luis...

SistemasSistemas de de SoporteSoporte a la a la decisióndecisión ClínicaClínica (SSDC(SSDC))
SistemasSistemas de de SoporteSoporte a la a la decisióndecisión ClínicaClínica (SSDC(SSDC))
Dr. Dr. LluísLluís DonosoDonoso BachBachDr. Dr. LluísLluís DonosoDonoso BachBach
Que es un SSDC? Que es un SSDC? Que es un SSDC? Que es un SSDC?
•Sistemas computarizados de gestión de la información diseñados para dar respuesta a problemas complejos en el proceso de toma de decisiones.
•Especialmente valiosos cuando la cantidad de información es excesiva para ser “procesada” a nivel individual
•Se aplica en múltiples campos (Negocios, militar, ingeniería..)
SSD
Base de conocimientos Base Datos
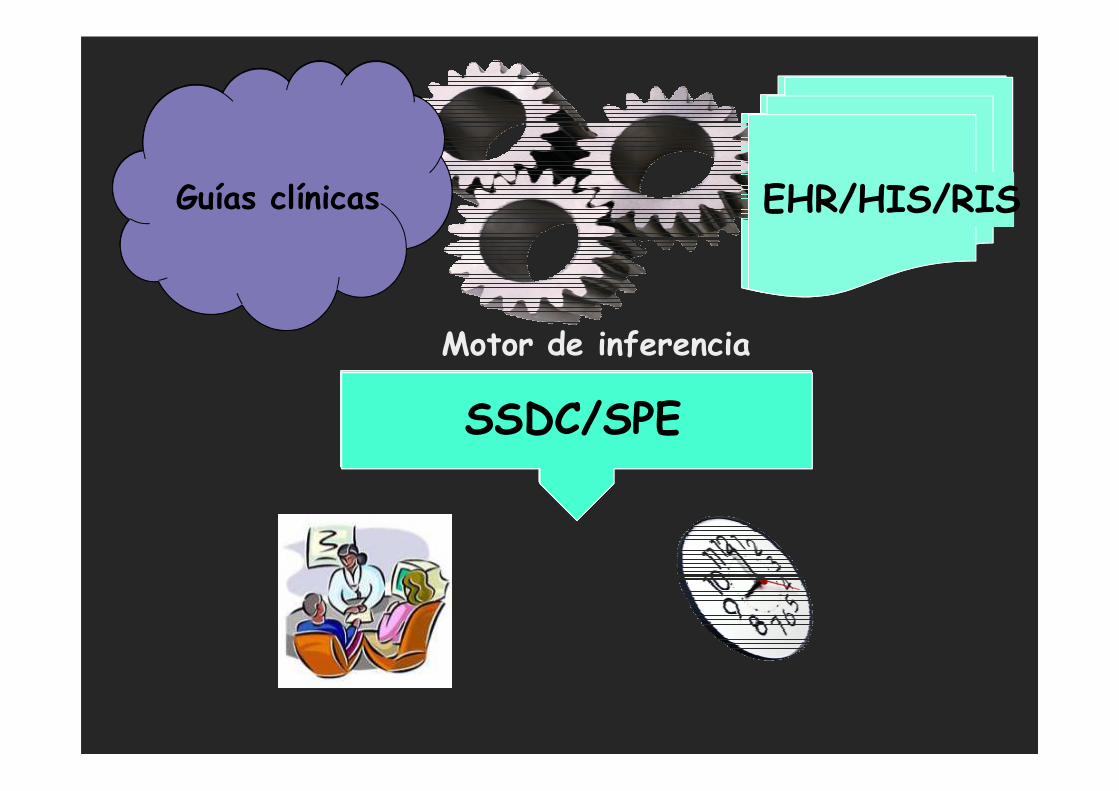
Motor de inferencia
SSDC/SPE
Guías clínicas EHR/HIS/RIS
SSDSSDC/SPE
SSDC. SSDC. AplicacionesAplicacionesSSDC. SSDC. AplicacionesAplicaciones
Básicas: alergias, duplicaciones, interacciones de fármacos, resultados críticos….
Avanzadas: Algoritmos inteligentes vías clínicas con información del paciente, integración con la petición electrónica, alertas proactivas…
Sobreutilización de la Imagen Sobreutilización de la Imagen médicamédica
Sobreutilización de la Imagen Sobreutilización de la Imagen médicamédica
•Tasa de crecimiento anual del 8%-16%
•Factores que influyen:
�Introducción de nuevas tecnologías (PET, MRA, CTA,
etc.)
�Nuevos usos de tecnologías existentes�Nuevos usos de tecnologías existentes
�“Self-referral”
�Demanda de los pacientes
�Medicina defensiva
•Se estima que >10% de los estudios son innecesarios o están
duplicados
•Exposición innecesaria a la radiación
CLINICAL DECISION SUPPORT FORCLINICAL DECISION SUPPORT FORCLINICAL DECISION SUPPORT FORCLINICAL DECISION SUPPORT FOR
EUROPEAN IMAGING REFERRAL GUIDELINESEUROPEAN IMAGING REFERRAL GUIDELINESEUROPEAN IMAGING REFERRAL GUIDELINESEUROPEAN IMAGING REFERRAL GUIDELINES
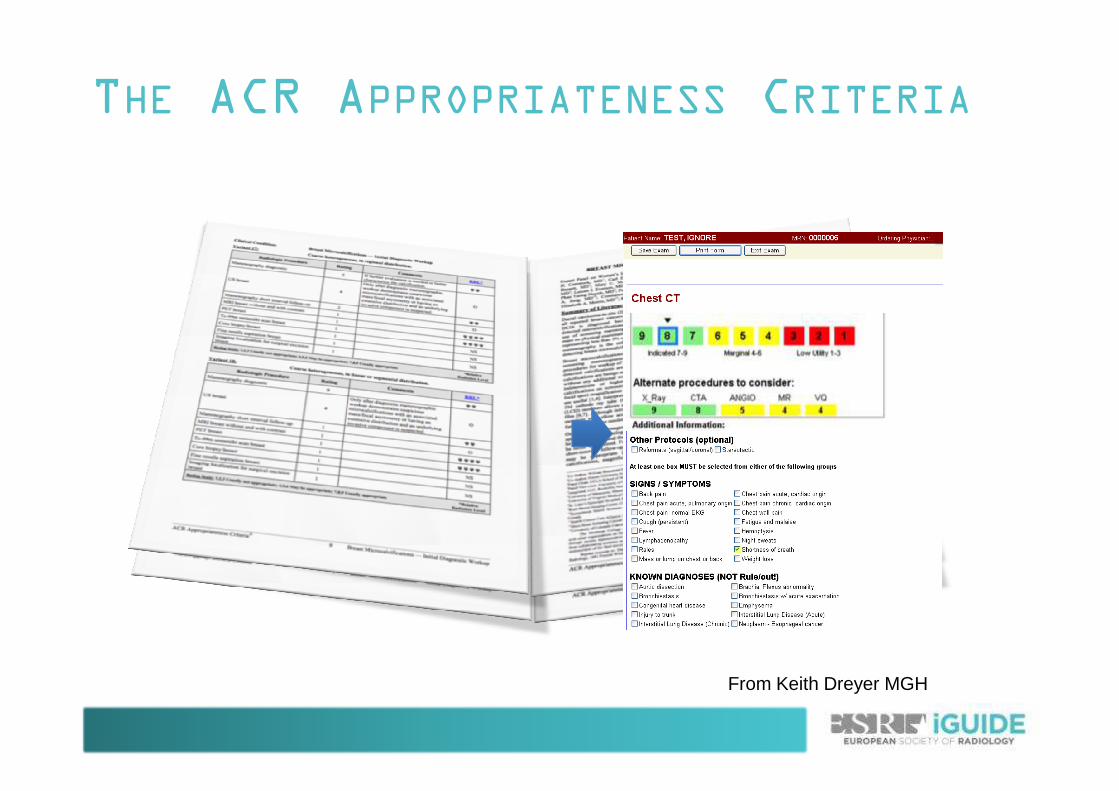
THE ACR APPROPRIATENESS CRITERIA
From Keith Dreyer MGH
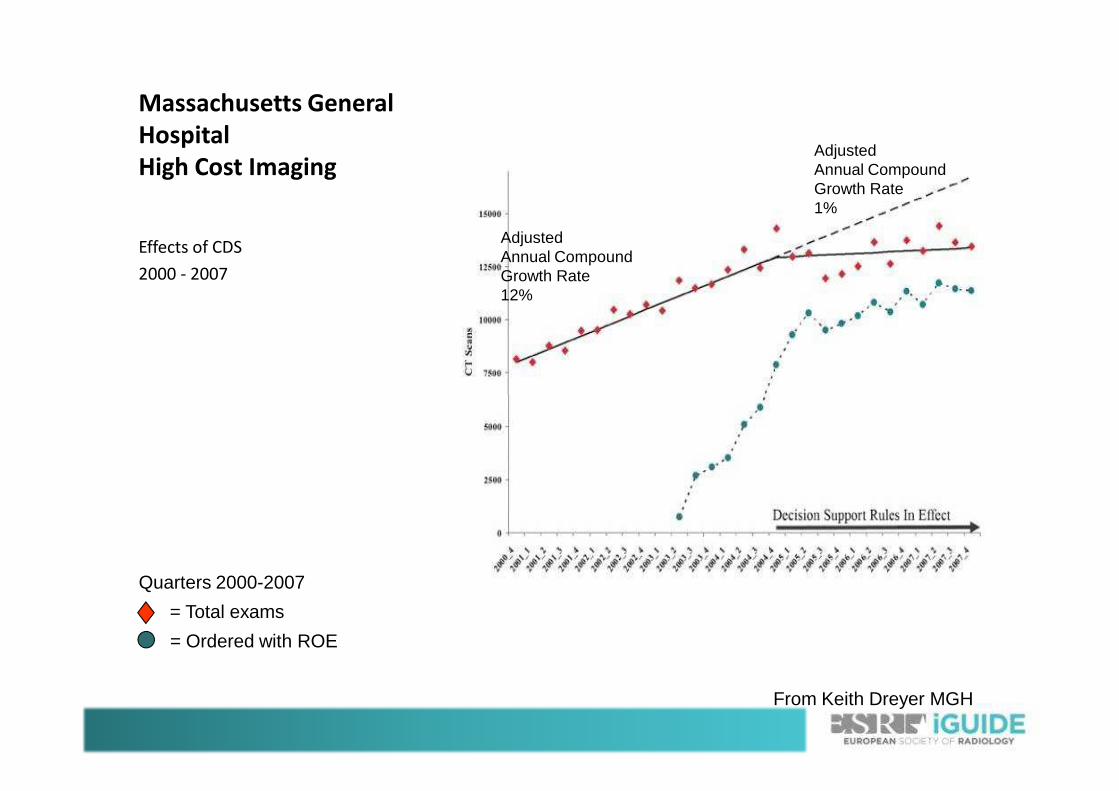
Massachusetts General
Hospital
High Cost Imaging
Effects of CDS
2000 - 2007
AdjustedAnnual CompoundGrowth Rate12%
AdjustedAnnual CompoundGrowth Rate1%
Quarters 2000-2007
= Ordered with ROE
= Total exams
From Keith Dreyer MGH

Legal Requirement For Use Of
Appropriateness Criteria In The
US

ACR SELECT
National Decision Support Company
ACR/NDSC RELATIONSHIP
• In July 2012, the American College of Radiology
(ACR) entered into an exclusive agency agreement
with National Decision Support Company (NDSC) to
provide the technical platform, support and
licensing of the ACR Appropriateness Criteria
under the name ACR Select. under the name ACR Select.
ACRAppropriateness
Criteria (AC)
NDSCLicensing, Platform
and Support+ =
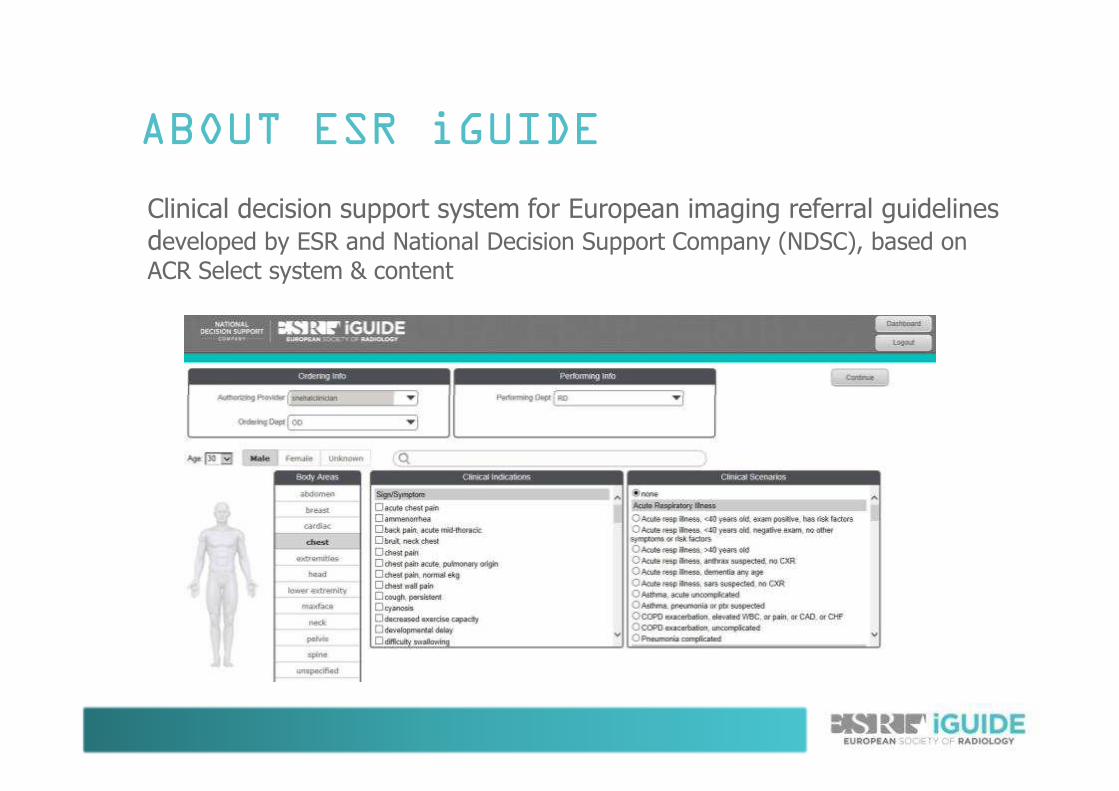
Clinical decision support system for European imaging referral guidelines developed by ESR and National Decision Support Company (NDSC), based on
ACR Select system & content
ABOUT ESR iGUIDE
NDSCLicensing, Platform
and Support+ =
Clinical decision support system for European imaging referral guidelines developed by ESR and National Decision Support Company (NDSC), based on
ACR Select system & content
ABOUT ESR iGUIDE
BACKGROUND
• ESR led European Commission study (2013) demonstrated inadequate status quo
– Availability of imaging referral guidelines in Europe is limited (70% of countries)
• only the UK and France fully develop guidelines; others adapt and adopt• only the UK and France fully develop guidelines; others adapt and adopt
– Imaging referral guidelines are hardly used in daily practice
• EURATOM basic safety standards directive (passed in 2013 and applicable from February 2018) mandates guideline availability in all member states
WHY CDS?
• Significant room to improve appropriateness in medical imaging
– ESR considers imaging referral guidelines essential to achieve this
Availability is not enough – increased & effective use of • Availability is not enough – increased & effective use of guidelines can only be achieved through user-friendly IT-based solutions
• Clinical decision support: proven efficiency in literature
ESR PILOT PHASE
• ESR initiated pilot project (2013) to create European imaging referral guidelines for use in CDS
– merger of national European guidelines revealed significant discrepancies
– national approach deemed unfeasible– national approach deemed unfeasible
• ESR decided to develop generic, evidence-based guidelines for use in a CDS system with flexibility for localisation
TRANSATLANTIC PARTNERSHIP FOR
CDS
• American College of Radiology (ACR) and NDSC introduced ‘ACR Select’ in the United States in 2012– Content based on ACR Appropriateness Criteria
• Implementation provided promising results• Implementation provided promising results– Introduction of ACR Select at Hospital Clinic Barcelona/ES
• ESR entered a partnership with ACR & NDSC (announced at ECR 2014)– ‘Europeanisation’ of ACR Appropriateness Criteria for use
in re-branded NDSC platform
– Common ACR-ESR vision: common set of global imaging global imaging global imaging global imaging referral guidelinesreferral guidelinesreferral guidelinesreferral guidelines
DEVELOPMENT OF EUROPEAN
GUIDELINES
• Scientific review of ACR Select content by ESR experts started in November 2014– Overseen by dedicated methodologist
– Adaptation of ACR AC to European standards of practice; incorporating evidence from the latest European studiesincorporating evidence from the latest European studies
– generic European imaging referral guidelines: provide a common core standard across Europe for further localisation on national or institutional basis
• Periodic content updates of ESR iGuide and ACR Select in cooperation between ESR and ACR– content is also updated or adapted continuously with feedback
from users
DEVELOPMENT OF EUROPEAN
GUIDELINES
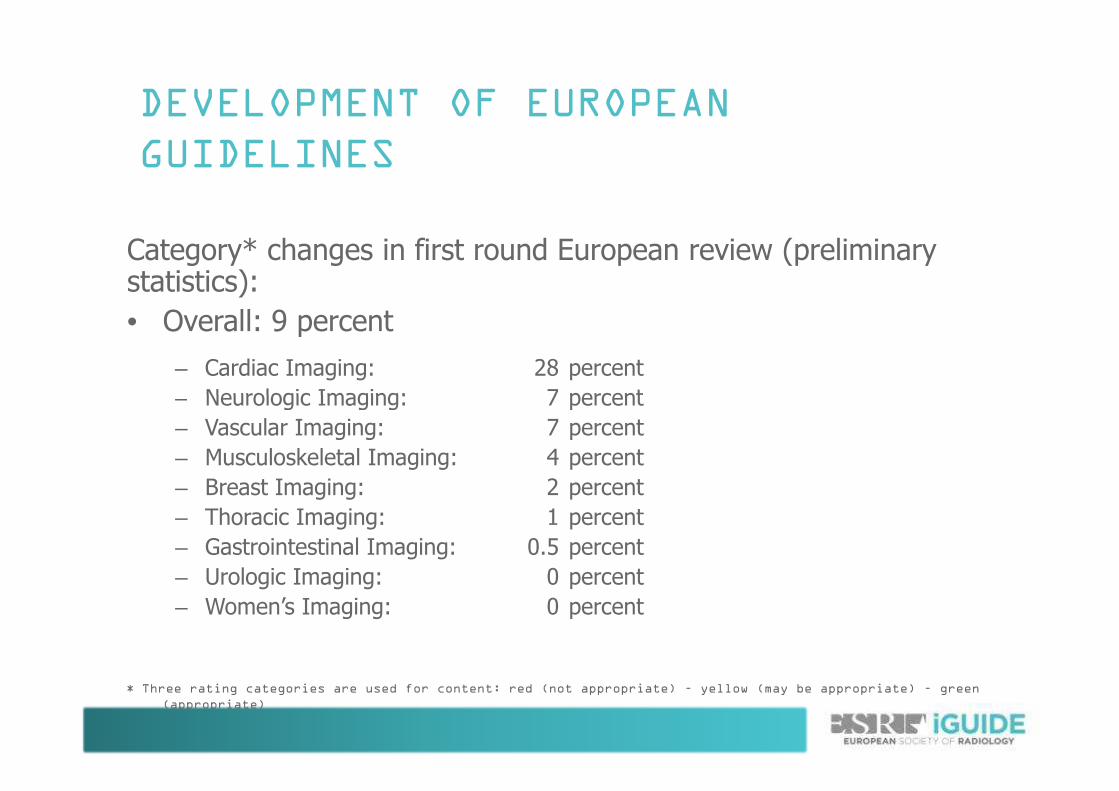
Category* changes in first round European review (preliminary statistics):
• Overall: 9 percent
– Cardiac Imaging: 28 percent
– Neurologic Imaging: 7 percent– Neurologic Imaging: 7 percent
– Vascular Imaging: 7 percent
– Musculoskeletal Imaging: 4 percent
– Breast Imaging: 2 percent
– Thoracic Imaging: 1 percent
– Gastrointestinal Imaging: 0.5 percent
– Urologic Imaging: 0 percent
– Women’s Imaging: 0 percent
* Three rating categories are used for content: red (not appropriate) – yellow (may be appropriate) – green
(appropriate)
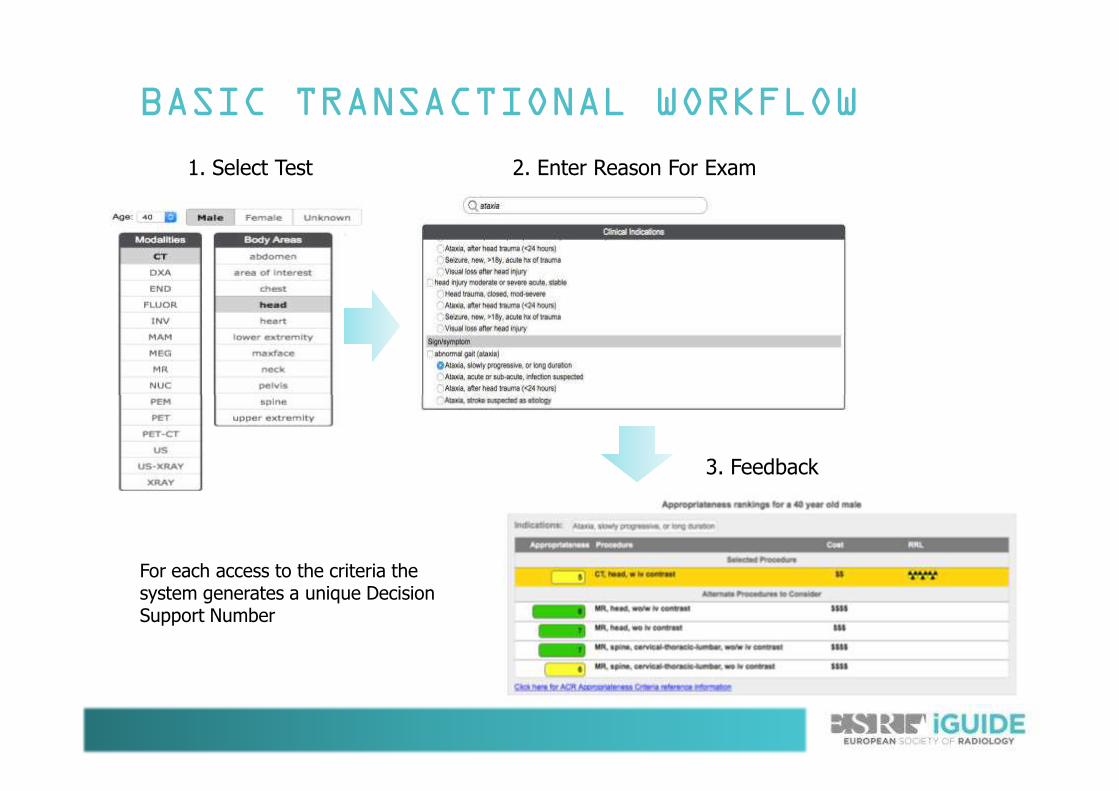
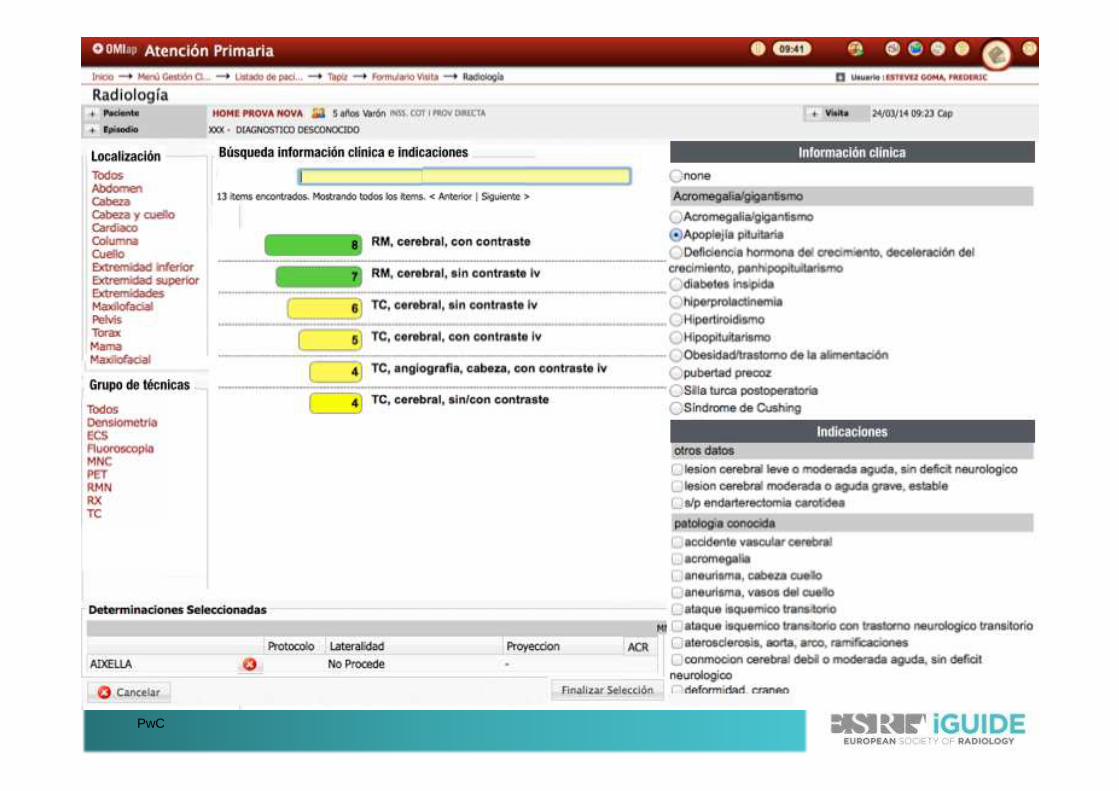
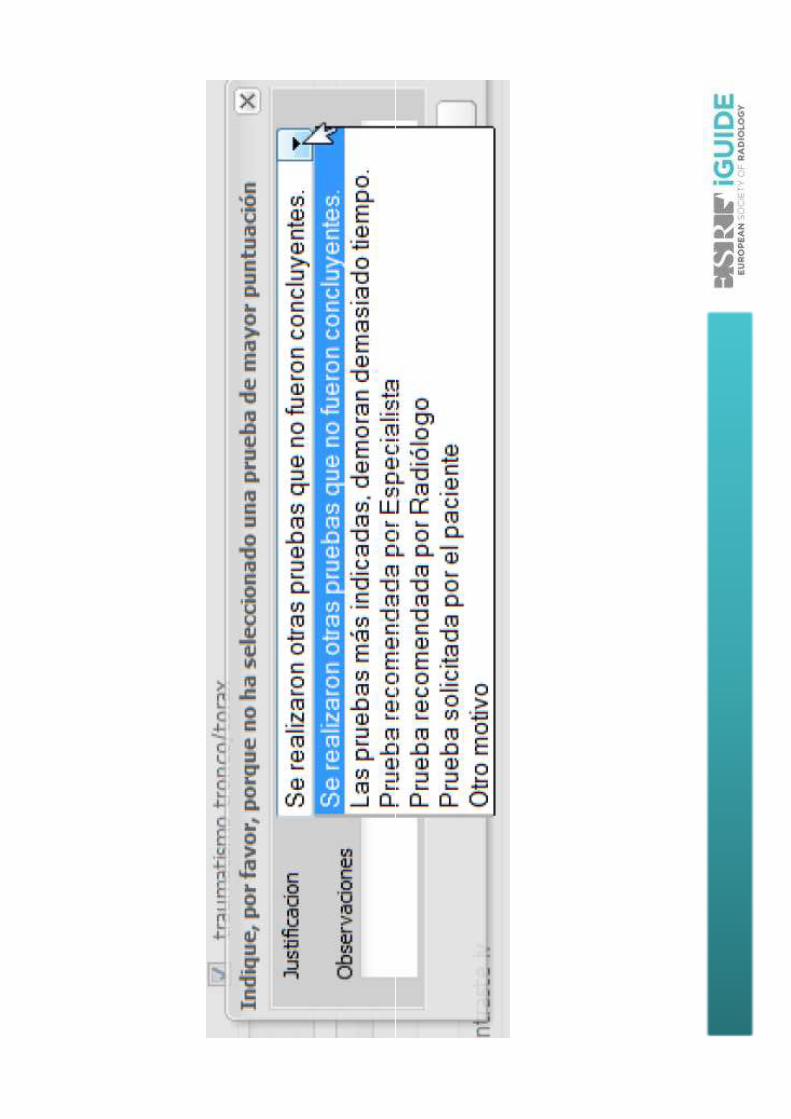
BASIC TRANSACTIONAL WORKFLOW
1. Select Test 2. Enter Reason For Exam
3. Feedback
For each access to the criteria the system generates a unique Decision Support Number
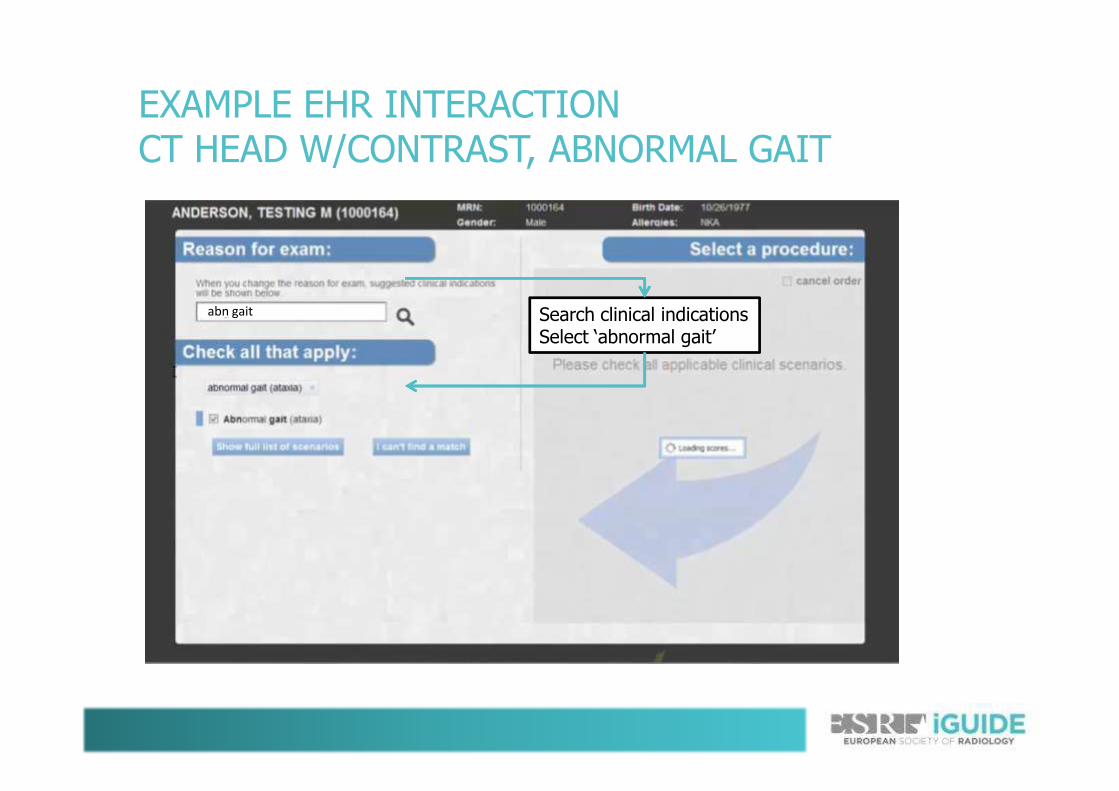
EXAMPLE EHR INTERACTION CT HEAD W/CONTRAST, ABNORMAL GAIT
Search clinical indicationsSelect ‘abnormal gait’
abn gait
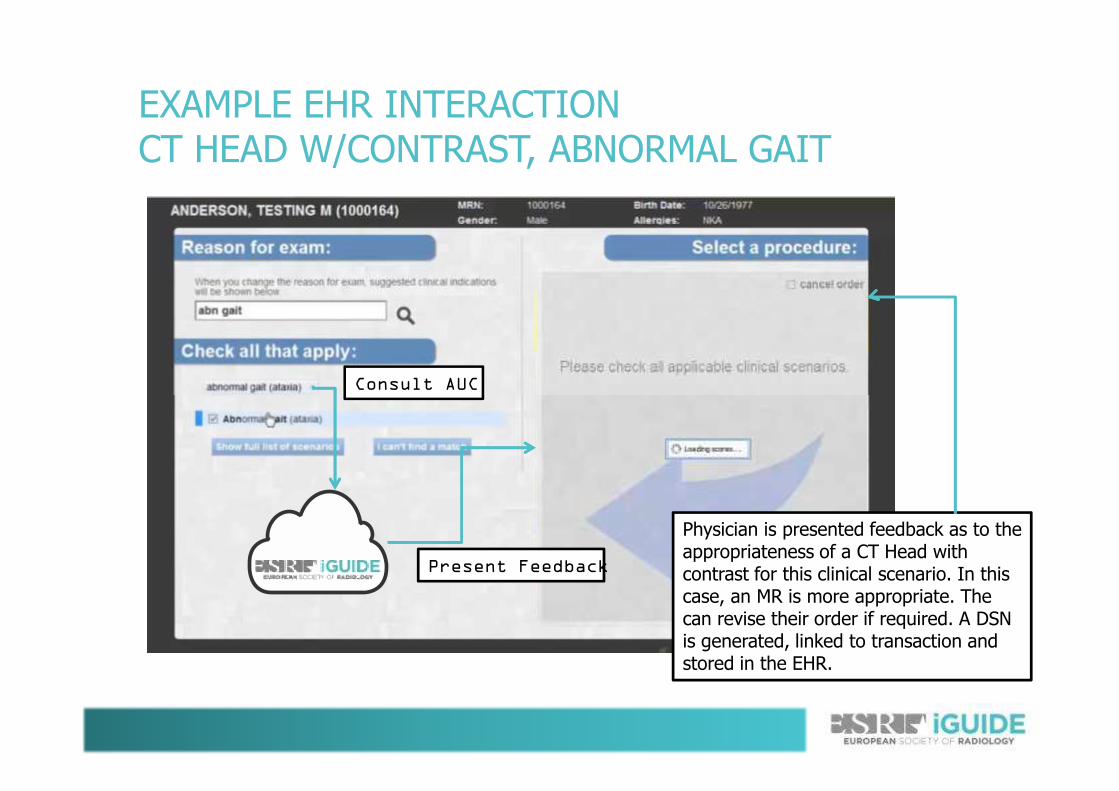
EXAMPLE EHR INTERACTION CT HEAD W/CONTRAST, ABNORMAL GAIT
Consult AUC
Physician is presented feedback as to the appropriateness of a CT Head with contrast for this clinical scenario. In this case, an MR is more appropriate. The can revise their order if required. A DSN is generated, linked to transaction and stored in the EHR.
Present Feedback
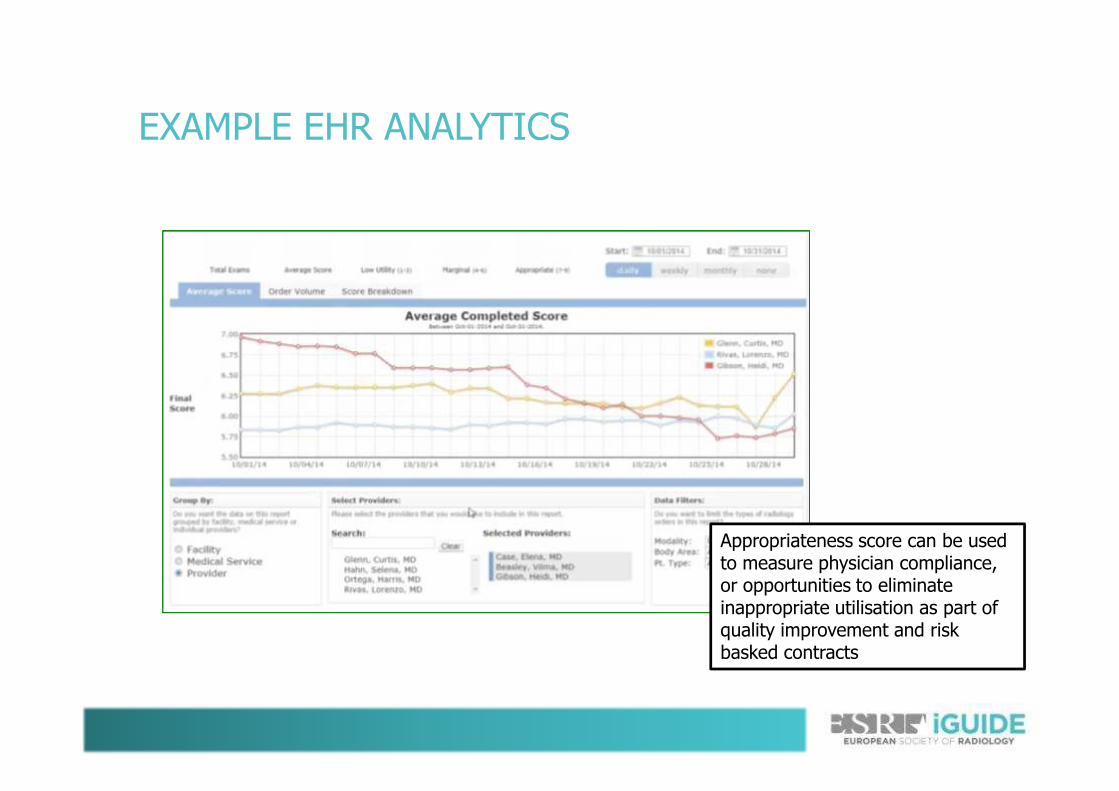
EXAMPLE EHR ANALYTICS
Appropriateness score can be used to measure physician compliance, or opportunities to eliminate inappropriate utilisation as part of quality improvement and risk basked contracts
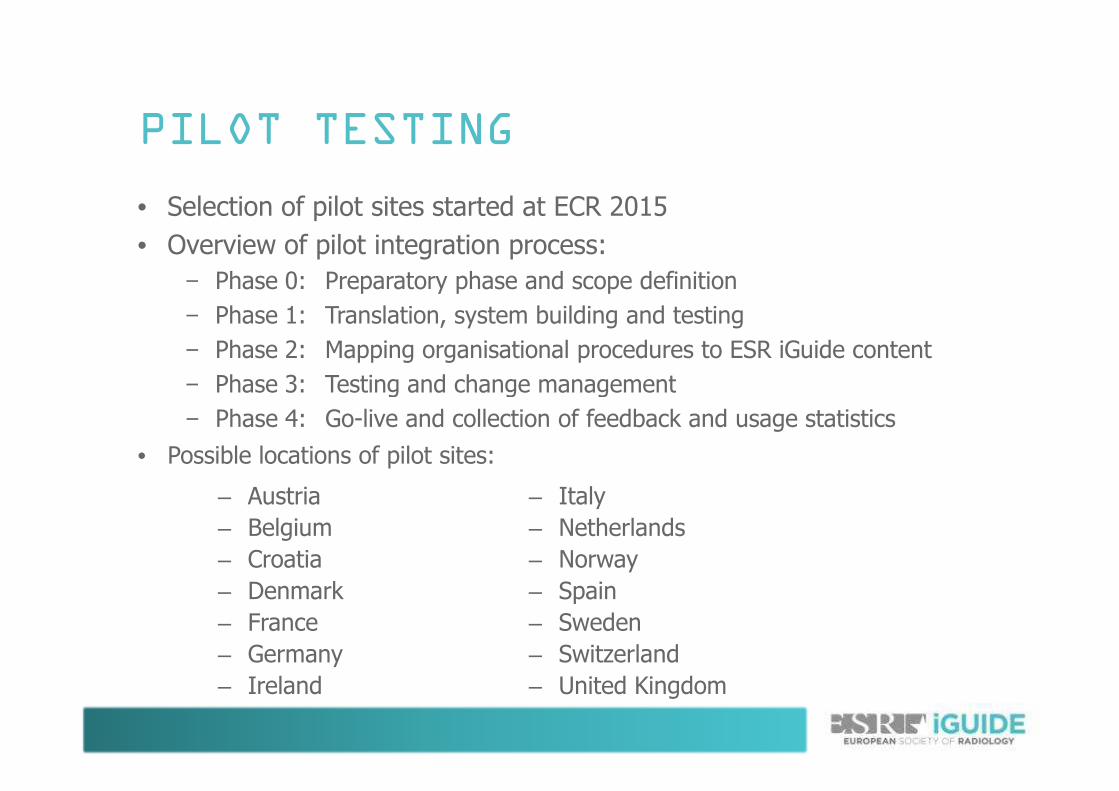
PILOT TESTING
• Selection of pilot sites started at ECR 2015
• Overview of pilot integration process:
− Phase 0: Preparatory phase and scope definition
− Phase 1: Translation, system building and testing
− Phase 2: Mapping organisational procedures to ESR iGuide content
− Phase 3: Testing and change management
– Austria
– Belgium
– Croatia
– Denmark
– France
– Germany
– Ireland
– Italy
– Netherlands
– Norway
– Spain
– Sweden
– Switzerland
– United Kingdom
− Phase 3: Testing and change management
− Phase 4: Go-live and collection of feedback and usage statistics
• Possible locations of pilot sites:
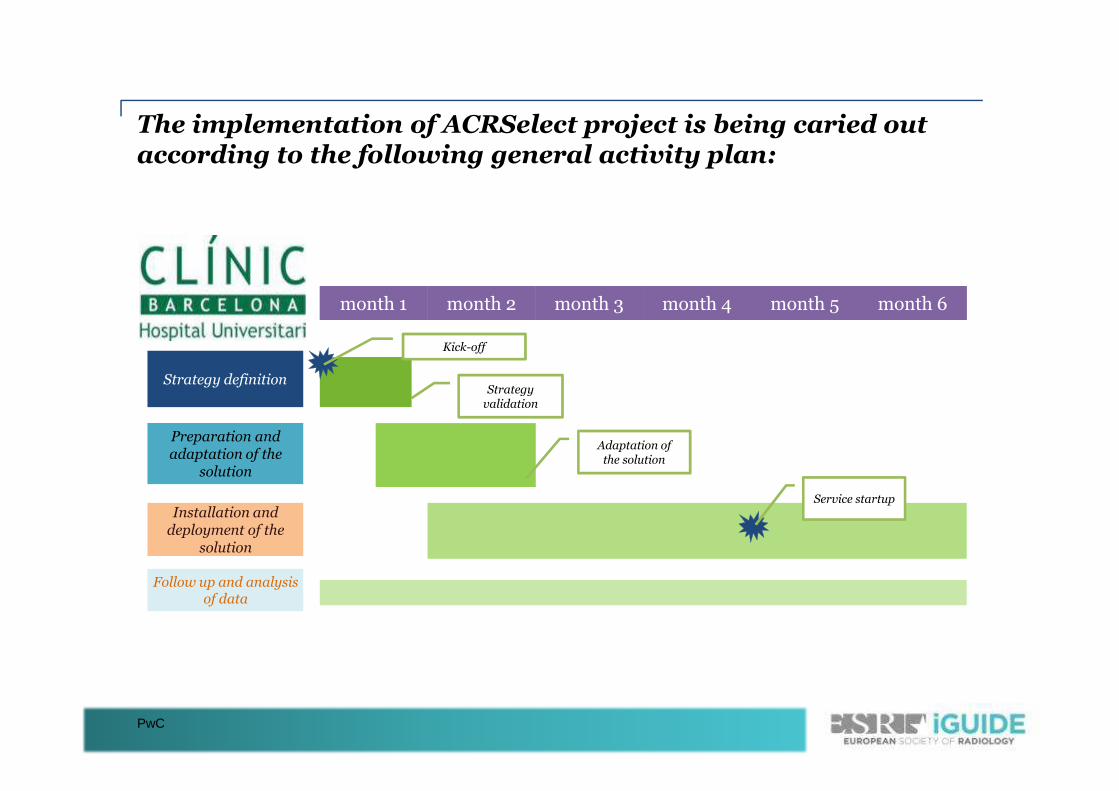
The implementation of ACRSelect project is being caried out according to the following general activity plan:
month 1month 1 month 2month 2 month 3month 3 month 4month 4 month 6month 6
Strategy definition
month 5month 5
Strategy
Kick-off
PwC
Preparation and adaptation of the
solution
Installation and deployment of the
solution
Follow up and analysisof data
Service startup
Adaptation of the solution
Strategyvalidation
PwC
ResultadosResultadosResultadosResultados
•• Diciembre 2014 Implantación definitiva Diciembre 2014 Implantación definitiva del SSDCdel SSDC
•• 89% 89% de las pruebas solicitadas con el de las pruebas solicitadas con el SSDC tenían una cualificación SSDC tenían una cualificación de de idoneidad adecuadaidoneidad adecuada
•• Diciembre 2014 Implantación definitiva Diciembre 2014 Implantación definitiva del SSDCdel SSDC
•• 89% 89% de las pruebas solicitadas con el de las pruebas solicitadas con el SSDC tenían una cualificación SSDC tenían una cualificación de de idoneidad adecuadaidoneidad adecuadaSSDC tenían una cualificación SSDC tenían una cualificación de de idoneidad adecuadaidoneidad adecuada
•• 5,8% 5,8% con un con un beneficio marginalbeneficio marginal
•• 5,2%5,2% como como no adecuadano adecuada
SSDC tenían una cualificación SSDC tenían una cualificación de de idoneidad adecuadaidoneidad adecuada
•• 5,8% 5,8% con un con un beneficio marginalbeneficio marginal
•• 5,2%5,2% como como no adecuadano adecuada
Navarro M, Pérez A, Pinyol M, Grau M, Navarro M, Pérez A, Pinyol M, Grau M, DonosoDonoso L, Ruiz L, Ruiz RR..
CAPSBECAPSBE--Hospital Clínic BarcelonaHospital Clínic Barcelona
RecomendacionesRecomendacionesRecomendacionesRecomendaciones
•Accesible en el puesto de trabajo
•Interface “clínico”
•La recomendación en términos de
probabilísticos
Stivaros S.M. et al. British Journal of Radiology, 83 (2010), 904–914
probabilísticos
•Explicación y Justificación accesibles
•No pretender sustituir al clínico!
•Hay que saber cuando romper las reglas!
TIMELINE
• December 2013: publication of ESR-led European Commission study on referral guidelines
• ESR-ACR-NDSC partnership announced at ECR 2014
• November 2014: start of guideline Europeanisation• November 2014: start of guideline Europeanisation
• Launch of prototype at ECR 2015
• Autumn 2015: finalisation of content
• Pilot tests in European countries from late 2015

EXPECTED BENEFITS
• Improved appropriateness
• Reduction in unnecessary radiation exposure
• More reliable justification process, better accountability through structured workflow– roles & responsibilities are adaptable to users’ requirements
• Streamlined clinical workflow• Streamlined clinical workflow
• More patient-centric treatment
• Educational benefits: feedback on appropriateness of selected exam, new insights through data collection & reporting
• Demonstrating utility of imaging equipment and potentially highlighting lack in quality or availability
THANK YOU!
www.ESRiGuide.org www.EuroSafeImaging.org