TEST RODILLA

of 6
Transcript of TEST RODILLA
-
8/7/2019 TEST RODILLA
1/6
Profile of bilateral anterior cruciate ligamentinjuries: A retrospective follow-up study
M MotohashiDepartment of Orthopedic Surgery, Yokohama Kowan Hospital, Yokohama, Japan
grou p th an in th e un ilateral injur y grou p (3.3 [1.4]versu s 2.2 [1.4] points; p
-
8/7/2019 TEST RODILLA
2/6
Vol. 12 No. 2, December 2004 Bilateral anterior cruciate ligament injuries 211
INTRODUCTION
Injur ies of the a nterior cruciate ligamen ts (ACL) canoccur d ur ing pa rticipation in spo rts, and are classifiedinto two types, depend ing on the mechanism of injury:
contact and non -contact. Non-contact injury is morecommon . Sour yal et al. 1 rep orted tha t 58 (79.5%) of 73 ACL injuries w ere non -conta ct. The aetiology o f ACL injur ies, how ever, is p robably mu ltifactorial. Byexamining p atients with injuries of the ACL wh ound erwent surgery at our hospital, we comp ared theage, act ivi ty level , injury mechanisms, surgicalresults, and r adiographic findings between those wh ohad bilateral injuries and those who had unilateralinjuries.
MATERIALS AN D METHOD S
Sur gical treatment of injur ies of the ACL in 458 kneeswas p erformed at Kowan H ospital in Japan b etweenJanu ary 1977 and December 1987. A total of 161pa tients54 males and 107 femaleshad un ilateralinjur ies and could be followed u p after surg ery. Themean age of 161 pa tients at the time of injur y w as19.8 years (range, 12.045.0 years). Injuries werebilater al in 11 patien ts (i.e. 22; 4.8% of kn ees), oneof whom was lost to follow-up. The mean age of the oth er 10 patientsall femalesat the time of
surgery was 18.2 years (range, 12.823.7 years). Thepatients were operated on on separate occasions.The mean follow-up du ration was 3.3 years (range,1.17.4 years) . Because the period of t reatmentspanned more than 10 years , d i ffe ren t surg ica lmethod s were used: for example, primar y sutu re of the ACL and reconstruction using the iliotibial bandin 7 knees, reconstruct ion u sing semi-tendinou smu sc les and the i l io t ib ia l band in 6 knees , andreconstru ction u sing semi-tend inous m uscles andthe gr acilis m uscle ligamen t in 2 kn ees. 2,3 Some injurieswere complicated, and involved the m edial meniscus
alone in 5 knees, the medial meniscus and posteriorcruciate ligament in one kn ee, the lateral men iscusand lateral collateral ligament in on e knee, and th emed ial and lateral menisci in one kn ee.
The author examined all patients and investigatedthe typ es of injuries and level of sports that causedthem . Pat ients w ere also classified according tohow they return ed to sp orting activities: group A,patients returning to the former level of sportingac t iv i t i es ; g roup B, those re tu rn ing to spor t ingact ivi t ies w ith a red uced abi li ty; group C, thoseturning to other sports ; and group D, those who
discontinued sports.2
J o i n t m o b i l i t y a n d o t h e r f a c t o r s w e r e a l s oevaluated. According to the Nakajima, Lachman, andanterior dr awer tests, instability w as d escribed assevere or definite, slight, and no instability. TheNa kajima test is a reverse p ivot sh ift test. The flexi-
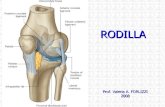
bility of 7 joints (w rist, knee, spine, elbow, shou lder,ankle, and hip) w as assessed w ith the joint laxity test(Fig. 1). 4 Each flexible joint w as given one p oint; a totalof 7 points w as th e full joint laxity score, signifyingmaximum flexibility.
The stand ing femorotibial anglethe lateral anglebetween axes of femoral and t ibial shaftswasmeasured by u sing anteroposterior radiographs of the knee in th e stand ing p osition. The inclination an gleof the tibial plateauthe average inclination of med ialand lateral tibial plateau to the tibial shaftwasmeasu red by using lateral rad iograph s. A line was
dr awn from the p opliteal groove parallel to the jointsurface on the ima ges of the intercond ylar fossa, andthe notch wid th ind exthe ratio of the w idth of theintercond ylar notch to that of the distal femur wasmeasu red (Fig. 2). This method was based on the on edescribed by Sourya l et al. 1 How ever, we consideredthat their method w ould give the anterior outlettheante r io r por t ion and the nar rowes t s i t eof thei n t e r c o n d y l a r f o s s a , w e m e a s u r e d t h e c l e a rosteosclerotic posterior arch and regarded it as thewid th of the intercondylar fossa.
The laxity score and femorotibial angle in th e
stand ing position in the bilateral injury group werecompared w ith those in the un ilateral injury grou p.Comp arisons of the inclination an gle of the tibia andnotch width ind ex were mad e among the bilateralinjur y, unilateral injury, and the healthy group of 21 fema les (23 knees) w ith n o ACL injur y. Stu d ents t test was u sed for statistical comparisons.
RESULTS
All bila teral ACL injur ies were su stained d uring
spor ting activities: basketball in 8 knees, gym nasticsin 6 knees, volleyball in 3 knees, han d ball in 2 kn ees,and javelin-throw ing in on e knee. All injuries w erespaced apart in time. The first injuries were of thenon-contact typ e in 8 knees and of the contact type in2 knees, whereas the second injuries in the otherknees w ere of the n on-contact typ e. Of the 20 injuredknees, 18 (90%) were of the non-contact type, themost common cause of wh ich w as landing from a jum p(10 knees) , fol lowed by sudden s topping duringbasketball games (3 knees), dashin g, cross-stepping ,s tepping, t reading, and fall ing from a horizontal
bar (one kn ee each). One of the 2 contact-type knee
-
8/7/2019 TEST RODILLA
3/6
212 M Motohashi Journal of Orthopaedic Surgery
injuries was du e to a crash with other players dur ingjum ping, and the other was caused by th e lateral knee
being treaded on by a player during shooting.
The mean a ge at the time of the first injur ies was16.2 years (ran ge, 12.719.3 years), and that at th etime of the second injur ies was 18.6 years (range,13.523.5 years). The mean interval between thefirst and the second injuries w as 2.4 years (range,0.36.2 years). After t he first injuries, 6 p atient sund erwent surgery as the primary treatment, wh ereas4 did not. In the 6 treated p atients, the m ean intervalbetween th e first and second injuries w as 3.3 years(range, 1.46.2 years); in th e 4 un treated pa tients, itwas 1.2 years (ran ge, 0.32.9 years) [Fig. 3].
After surgical treatmen t of the first injuries, and
on the basis of how sports w ere resum ed, 3 patientswere classified as grou p A, 6 as grou p B, and one asgroup C. After surgical t reatment of the secondinjuries, one p atient w as classified as grou p A, 7 asgroup B, one as group C, and one as group D.
The postoperative results of the N akajima testshowed no instabi l i ty in 16 (80%) knees, s l ightinstability in 3 (15%) knees, and definite instabilityin one (5%) knee. The results of the Lachman testshowed no instabi l i ty in 11 (55%) knees, s l ightinstability in 4 (20%) knees, and d efinite insta bility in5 (25%) knees. The resu lts of anterior d raw er tests
showed no instabi l i ty in 10 (50%) knees, s l ight
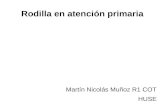
1. Wrist
4. Elbow
15
2. Knee
3. Spine
5. Shoulder 6. Ankle 7. Hip
10
45
1. Wrist-thumb test2. Knee hyperextension test3. Palm-to-floor test4. Elbow hyperextension test
5. Hand-to-hand on the back test6. Ankle dorsiflexion test7. Over pivot test
Figure 1 Joint laxity test: the laxity of 7 joints is examined; 7 points is the maximum score.
N
W
Figure 2 Calculation of the notch width index: a line isdrawn from the popliteal groove parallel to the joint surfaceon the X-ray image of the intercondylar fossa; the notch widthindex i s the width of the osteosclerotic posterior arch of theintercondylar notch (N) divided by the width of the distal femur(W).
-
8/7/2019 TEST RODILLA
4/6
Vol. 12 No. 2, December 2004 Bilateral anterior cruciate ligament injuries 213
instability in 6 (30%) knees, and definite instabilityin 4 (20%) knees. Upright sitting was possible for8 patients and imp ossible for 2. Comp lete extensiono f t h e k n e e w a s p o s s i b l e f o r a l l p a t i e n t s , b u thyp erextension w as observed in 4 patients. Fixed
flexion deformity was absent from all patients. Nopa t ien t had symptoms in the meniscus , such asMcMurrays sym ptom . Prepatellar sensory d isorderwas observed in 5 knees, and mu scular hernia aftercollecting the iliotibial band in 4 knees.
The mean laxity score was 3.3 points (ran ge, 26points; stand ard d eviation [SD], 1.4 poin ts) for th e10 females in the bilateral injur y grou p, w hereas itwas 2.2 point s (range, 06 po ints; SD, 1.4 points ) amon g38 females in the u nilateral injury group wh o couldbe examin ed for joint laxity test. The laxity score wassignificantly higher in the bilateral injury grou p than
in the un ilateral injur y grou p (p
-
8/7/2019 TEST RODILLA
5/6
214 M Motohashi Journal of Orthopaedic Surgery
injured du ring landing from a jum p. There were nopatients with injuries caused by a cutting m otion.
Sou ryal et al. 1 reported th at the mean age of pa-tients w ith bilateral ACL injur ies at the tim e of theirfirst injur ies was 19.8 years an d th at the m ean interva l
to the injuries in th e second knee w as 3.9 years. Incomparison, because m ost patients in our series werefemale jun ior and senior high school studen ts, theywere, on average, much you nger at th e time of theirfirst injuries (16.2 years); the mean interval to thesecond injur ies in the oth er knees was also shorter2.4 years overall and 3.3 years for those whose firstinjuries were treated. In the p atients with u ntreatedfirst injuries, the m ean interval betw een the first andsecond injur ies was p articularly short, at 1.2 years.Hence, patients with ACL injuries wh o are you ngerthan 16 years shou ld be careful abou t the occur rence
of injur ies in the other knee. Female junior andsenior high school s tudents with uni lateral ACLinjur ies may hav e a higher risk of sustaining injuriesin the other knee wh en landing or jum ping, whenreturn ing to club activities and ph ysical edu cation,irrespective of wheth er the first inju ries are surgicallytreated.
Nicholas 5 examined th e relationship betw een jointflexibility an d the incid ence of injur ies. We p reviouslyreported that the flexibility of joints was closelycorrelated with the occurrence of bi la teral ACLinjuries. 2 In our stu dy, the laxity score was significant ly
h igher in the b i la te ra l in ju ry group than in theuni lateral injury group. We considered that thisd ifference reflected n ot on ly the relaxation of jointsbut also the relaxation of connective tissue in theentire bod y, includ ing th e ACLs. This relaxation w asconsidered to be a factor of ACL injuries. 6
Palmer 7 repor ted in 1938 that th e ACL is extend edin the externally rotated p osition by the bend ing of the knee, and is injured by impingement with theintercond ylar fossa. Norw ood an d Cross 8 also reportedthat the extended ACL becomes imp inged in theanterior par t of the intercond ylar fossa. Hou seworth
et al.9
suggested that ACL injuries are caused by thenarrowing of the posterior arch of the intercond ylarfossa. Furthermore, Anderson et al. 10 reported thatstenosis of the anter ior openin g of the intercond ylarfossa, wh ich w as observed by compu ted tomograp hy(CT), is related to ACL injur ies. Using CT, Ha rn er
et al. 11 had found significant evidence of intercondylarnotch stenosis second ary to increased lateral cond ylarwid th am ong bilateral ACL-injured patients comp aredwith non-injured ind ividuals.
S c h i c k e n d a n t z a n d We i k e r 12 m e a s u r ed t h e
intercond ylar notch by including th e notch width atthe most narrow d istal opening of the notch and thecondylar w idth at its greatest width above the jointline. In contrast, we measured the notch wid th ind exaccord ing to the meth od of Sour yal et al. 1 wh ich givesmeasu rements of the narrowest anterior outlet of theintercond ylar fossa. The ad vantages of this method areas follow s:(1) Imaging of the intercond ylar fossa is easier than
condu cting CT and magn etic resonance imaging;(2) The popliteal groove can be used as a marker for
measu ring the wid th of the intercondylar fossa;
(3) Being a ratio, the notch wid th ind ex is not affectedby th e shap e of the intercond ylar fossa itself; and
(4) The width of the intercondylar fossa can beeasily measured, and accurate comparisons arepossible.As in the study of Hou seworth et al., 9 we con-
sidered th at ACL injur ies are caused by the p osteriorarch of the intercond ylar fossa, and measu red thewidth of the clear osteosclerotic posterior arch onX-ray images of the intercond ylar fossa. It was sh ow nthat a small notch width ind exthe narrow ing of theposterior archwas closely related to th e occurren ce
of ACL injuries.Hus ton e t a l . 6 repor ted ACL in jur ies among
female athletes in 2000. A female athlete w ith ananterior cruciate injury may be an ind ividu al whoseQ-angle is significantly larger than average, has anotch wid th s ignif icant ly smaller than most , hasjoints classified as ligam entou s lax, and is weaker thanher m ale coun terparts. A large proportion of ACLinjuries occur wh en an a thlete land s from a jum p.Landing imposes forces on the body that must beabsorbed prim arily by the low er extremity. If loadsbecome too great for the body to a ccomm oda te, or if
imp act absorption fails, an injury w ill occur . Ourresults suggest that several factors are involved inthe occurren ce of ACL injuries. Fu rth er invest igationis necessary to elucidate the m echanism of injury andthus formulate prevention strategies for people wh oplay sports.
REFERENCES
1. Souryal TO, Moore HA, Evans JP. Bilaterali ty in anterior cruciate ligament injuries: associated intercondylar notch stenosis.
Am J Sports Med 1988;16:44954.
-
8/7/2019 TEST RODILLA
6/6
Vol. 12 No. 2, December 2004 Bilateral anterior cruciate ligament injuries 215
2. Motohashi M, U ematsu H, Takemura K. Anterior cruciate ligament reconstruction using semitendinosus and gracil is tendonswi th a modified over-the-top method. J Orthop Surg (Hong Kong) 1999;7:4750.
3. Takazawa H, Takao R, Motohashi M, Shimada N, Mitsuhashi S. Anterior cruciate ligament reconstruction using semitendinosusand gracil is tendons [in Japanese]. Kotsu Kansetsu Jintai 1989;2:106572.
4. Fukubayashi T. Patell a dislocation. Subluxation. In: Nakajima N, editor. Sports orthopaedic surgery. Tokyo: Nankoudou Co;1987:24861.
5. Nicholas JA. Injuries to knee ligaments. Relationship to looseness and tightness in football players. JAMA 1970;212:2236 9.6. Huston LJ, Greenfield ML, Wojtys EM. Anterior cruciate ligament injuries in the female athlete. Potential risk factors. Clin
Orthop 2000;372:5063.7. Palmer I. On the injuries to the ligament of the knee joints. A clinical study. Acta Chir Scand 1938;81(Suppl):S1282.8. Norwood LA Jr, Cross MJ. The intercondylar shelf in the anterior cruciate ligament. Am J Sports Med 1977;5:1716.9. Houseworth SW, Mauro VJ, Mellon BA, Kieffer DA. The intercondylar notch in acute tears of the anterior cruciate ligament:
a computer graphics study. Am J Sports Med 1987;15:2214.10. Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB. Analysis of the intercondylar notch by computed tomography. Am
J Sports Med 1987;15:54752.11. Harner CD, Paulos LE, Greenwald AE, Rosenberg TD, Cooley VC. Detail ed analysis of patients wi th bi lateral anterior
cruciate ligament inj uries. Am J Sports Med 1994;22:3743.12. Schickendantz MS, Weiker GG. The predictive value of radiographs in the evaluation of uni lateral and bil ateral anterior
cruciate ligament injuries. Am J Sports Med 1993;21:1103.