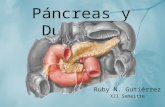
Trauma de Páncreas y Duodeno
17
TRAUMA DE PÁNCREAS Y DUODENO LUDWIN FERNEY ROJAS ESPINOSA
description
ppt
Transcript of Trauma de Páncreas y Duodeno

TRAUMA DE PÁNCREAS Y DUODENO
LUDWIN FERNEY ROJAS ESPINOSA

EPDEMIOLOGÍA
Representa el 4% de las lesiones traumáticas abdominales
0,4% de las admisiones hospitalarias por trauma

GENERALIDADES
ÓRGANOS RETROPERITONEALES
TRAUMA DE PÁNCREAS (20% COMPROMETE DUODENO)
TRAUMA DE DUODENO (30% COMPROMETE PÁNCREAS)
MORTALIDAD DEL 30%
LA CABEZA Y CUELLO DEL PÁNCREAS ESTÁN COMPROMETIDOS EN UN 37%, EL CUERPO EN UN 36%, LA COLA EN UN 26% Y LAS LESIONES SON MÚLTIPLES EN UN 3%
LAS LESIONES DE LOS CONDUCTOS PANCREÁTICOS ESTÁN PRESENTES EN EL 15% DE LOS CASOS Y SON MÁS FRECUENTES EN EL TRAUMA PENETRANTE.

CLASIFICACIÓN
Las lesiones grados I y II se presentan con una frecuencia de 60 y 20%, respectivamente. Las lesiones grado III representan el 15%, y las lesiones grado IV son poco frecuentes, con sólo 5%.

MECANISMO DE LESIÓN
TRAUMAS PENETRANTES 70%
SECUNDARIOS A ARMA BLANCA O POR ARMAS DE FUEGO
TRAUMAS CERRADOS 30%
SEGÚN DONDE SE LOCALICE LA MAYOR FUERZA DEL IMPACTO SERÁ LA ZONA PANCREÁTICA LESIONADA

DIAGNÓSTICO
ANAMNESIS Y EXÁMEN FÍSICO empleo de cinturón de seguridad, choque frontal de vehículos, aplastamiento, caídas
la signología indica necesidad de exploración quirúrgica inmediata
LABORATORIOS son poco específicos
AMILASEMIA
LPD poco específico porque el trauma pancreático es una lesión retroperitoneal
ULTRASONOGRAFÍA
TAC permite distinguir todas las lesiones pancreáticas desde un páncreas contundido hasta una profunda
laceración con compromiso del conducto pancreático

TAC
Fractura glandular con o sin separación de los fragmentos
Hematoma intraglandular
Hematoma retroperitoneal
Disminución importante del contorno graso peripancreático
Colecciones dentro y fuera del páncreas
Adelgazamiento de la fascia renal anterior izquierda
Colección líquida interpuesta entre el páncreas y la vena esplénica

TRATAMIENTO
La principal causa de muerte en el trauma pancreático es el sangrado masivo desde grandes vasos u otros órganos
La lesión del conducto pancreático determina mayor morbimortalidad, especialmente cuando no se diagnostica.
La ruptura duodenal asociada empeora el pronóstico más si el paciente presenta fístula biliar, duodenal y pancreática.
Aun cuando se puede extirpar hasta el 90% del páncreas sin gran repercusión de la suficiencia pancreática, es necesario ser prudente al resecar tejido pancreático cuando los pacientes son diabéticos o presentan pancreatitis crónica

TRATAMIENTO NO QX
Internados en Unidades de Cuidados Intensivos donde se adoptan las siguientes medidas: Monitoreo de parámetros vitales.
Revaluación clínica frecuente.
Exámenes imagenológicos como tomografía, pancreatografía y endosonografía
Indicación de cirugía inmediata si hay inestabilidad hemodinámica y signos de irritación peritoneal

TRATAMIENTO QX
CIRUGÍAS DE URGENCIA IRRITACIÓN PERITONEAL + DISTENSIÓN ABDOMINAL
HIPOTENSIÓN
REPOSICIÓN ENÉRGICA DE LA VOLEMIA
ANTIBIOTICOTERAPIA CON CEFALOSPORINAS 2G
LAPAROTOMÍA MEDIA AMPLIADA
SANGRADO: PACKING COMPRESIVOS

PANCREATORRAFIA

DERIVACIONES PANCREÁTICAS

DIVERTICULIZACIÓN DUODENAL

EXCLUSIÓN PILÓRICA

RESECCIÓN PANCREÁTICA

MORBILIDAD
APARECEN EN HASTA UN 42%
PRINCIPALES COMPLICACIONES FÍSTULAS PANCREÁTICAS
ABSCESOS INTRAABDOMINALES
PANCREATITIS
PSEUDOQUÍSTES

MORTALIDAD
9 AL 54%