


![Ppt0000078 [Somente leitura]papp.seplag.ce.gov.br/papp/images/stories/BNDES/apresent... · 2020. 2. 7. · FORTALEZA, SEPLAG, 05 Fev 2020 6 CRIAR E CAPTURAR VALOR Rosário Macário](https://static.fdocuments.co/doc/165x107/60e88d053625c13b8861e412/ppt0000078-somente-leiturapapp-2020-2-7-fortaleza-seplag-05-fev-2020-6.jpg)

Idiomas
Páginas
Jurídico


FIBROSE ENDOMIOCÁRDICA
Por:
Maira Alexandra Mabica
PG Medicina Interna
2º ano
Setembro 2012

2
SUMÁRIO
Introducao Epidemiologia Anatomia e Fisiologia Etio-fisiopatologia Clinica Diagnostico Diagnosticos diferenciais Manejo e Tratatmento Prognostico Bibliografia

3
INTRODUÇÃO
Etiologia idiopática das zonas tropicais e subtropicais.
Restrita ás reg tropicais pobres Este, Centro e Oeste de África;
Patogénese pouco entendida; Geografia? Dieta? Infecções?++ Eosinofilia como factor perpetuador; Forma grave - mau prognóstico, sobrevida de
2 anos após o diagnóstico.

4
CMP: músculo cardíaco estrutural e funcionalmente anormal, na ausência de dça coronária, HTA, dça valvular ou congénita, suficiente p/ explicar as anormalidades observadas no miocárdio.
CMP restritiva: ventrículo rígido, ñ dilatado disfunção diastólica + restrição enchimento ventricular pressões de enchimento elevadas e dilatação da aurícula.

5
Miocárdica Infiltrativa
Amiloidose
Sarcoidose
Dça Gaucher
Dça Hurler
Infiltração Gorda
Miocárdica ñ infiltartiva
CM Idiopática
CM Familiar
CM hipertrófic
a
Esclerodermia
Pseudoxanthoma
elasticum
CM diabética
Dças Armazena
mento
Hemocromatose
Dça de Fabry
Dças armazenam
ento Glicogénio
Endomiocárdio
FEM
Sdm Hipereosinofíli
c
Dça Carcinóide do coração
Ca metastático
s
Ef. Tóx Antraciclina
Radiação
Drogas – Endocardite
fibrosa
CMR

6
EPIDEMIOLOGIA Descrita pela 1ª vez no Uganda em 1940 – 20% dos casos enviados p/
eco-cardíaca.
Vários termos usados inicialmente: Doença endomiocárdica Endocarditis parietalis fibroplástica Fibrose endocardial Endocardite constrictiva Fibroelastose endocardial
Parece CMP restrictiva mais comum, apesar da falta de dados; >ia dos casos: Uganda, Nigéria, Costa do Marfim, Índia sul e Brasil; mas tb em zonas
subtropicais.
++ jovens , pico bimodal aos 10 e 30 anos observado em Moçambique e no Uganda.
Ambos sexos
++ raça negra (é mesmo racial ou maior parte dos pobre são negros???)

7
Julho 2008
~20% de 1063.; só 22,7% eram sintomáticos! ++ entre 10-19 anos ++ homens ++biventricular;+ direita;- esquerda Alta concordância familiar!!

8
ANATOMIA E FISIOLOGIA

9
Processo primário causador de fibrose ainda não completamente compreendido.
ETIO-FISIOPATOLOGIA
Fibrose
compliance
Restrição enchiment
o ventricularIrregular
;++
apices e musc.
papilares
Afecção válv. AV Dilataçã
o auricularVel.
condução
electricaBloqueios/arritmias

10
No miocardio, geralmente, fibrose ligada a aumento de TGF-β1.
Não na FEM!!?? Teorias:
ETIO-FISIOPATOLOGIA
Hipereosinofilia
Infeccções
Imunologia
Exposição ambiental/
fact geoquímicos
Genética
Fact. dietéti
cos

11
ETIO-FISIOPATOLOGIA
1. Teoria hipereosinofílicaPRÓS CONTRAS
FEM assemelha-se ao último estadio do sdm hipereosinofílico (Eosinofilia sustida)
Eosinofilia sérica e miocárdica não foi consistentemente demosntrada na FEM. (Mocumbi AO, Carrilho C, . Sarathchandra P, Ferreira B, Yacoub M, Burke M. Echocardiography accurately assesses the pathological, abnormalities of chronic endomyocardial fibrosis.Int J Cardiovasc Imaging, 2010)
Doentes com hipereosinofilia de várias etiologias passam pelas 3 fases ( inflamação endomiocárdica → formação de trombo → cicatrização)
Biópsias endomiocárdicas não demosntraram eosinofilia na FEM mesmo nos indivíduos com suspeita de doença inicial.

12
ETIO-FISIOPATOLOGIA
2. Teoria InfecciosaPRÓS CONTRAS
Ocorrência de FEM em pessoas da europa e Norte da América após curtas estadias em áreas endémicas
Não foi demonstrada associação consistente com nenhum organismo.
Várias infecções tem sido implicadas na fisiopatologia da FEM: Toxoplasmose; Febre reumática; Malária; Infecções helmínticas; Shistosomíase; Microfilária; Loa-loa; Filaríase
Muitos países com a mesma carga de Malária e Filaríase que o Uganda e Nigéria não têm FEM
Achados de lesões fibróticas endomiocárdicas em ratos infectados com Plasmodium berghei
Várias crianças estudadas c/ Malária por falciparum---- evidência insuficiente q ligasse as patologias.

13
ETIO-FISIOPATOLOGIA
3. Teoria fact. Ambientais/ geoquímicosPRÓS CONTRAS
“CERIUM”, elemento raro abundante no solo de áreas endémicas. • Induz FEM nos roedores. • Alto nivel sérico em ptes c/ FEM comparado
com controlos. • A incidência da FEM ↓ na Índia ( ↓ Cerium
no solo com a modernização). • ↑ nos dentes de leite das crianças do
Uganda nas regiões com alta prevalência de FEM comparando com crianças da Inglatera.
• Níveis aumentados de cerium foram encontrados nos corações de pessoas de regiões costeiras dos trópicos
• Cerium inicia a cura das feridas nos tecidos cardíacos dos ratos levando a fibrose cardíaca que pode ser um estímulo directo para os fibroblastos do endocárdio.
• FEM não pode ser explicada por uma só causa em todas as áreas reportadas
• Pensa-se que sejam vários factores ambientais actuando em indivíduos com predisposição genética.

14
ETIO-FISIOPATOLOGIA
4. Teoria ImunológicaPRÓS CONTRAS
Foi demosntrado a presença de auto-Ac anti-miosina na FEM. (Mocumbi AO, Latif N, Yacoub MH. Presence of circulating anti-myosin antibodies in endomyocardial fibrosis. PLoS Negl Trop Dis 2010; 4:e661.) • O papel da auto-imunidade é
sugerido pelos achados de altos títulos de AC contra Malária (anti-streptolisina, esplenomegália malárica hiperimune)
Esses Ac podem também ser detectados em outras formas de doença cardíaca como Síndrome de Dresser, doença cardíaca reumática e em pacientes com rejeição pós-transplante.

15
ETIO-FISIOPATOLOGIA
5. Teoria GenéticaPRÓS CONTRAS
Foi identificado uma ligação familiar em muitos estudos.
Não se sabe se a ligação familiar é devida a factores ambientais, genéticos ou ambos. (Mocumbi AO, Ferreira MB, Sidi D, Yacoub MH. A population study of endomyocardial fibrosis in a rural area of Mozambique. N Engl J Med 2008; 359:43.)

16
ETIO-FISIOPATOLOGIA
7. Teoria Fact. Dietéticos
Prolongada ingestão de Tuber cassava (mandioca) em associação com privação de proteínas (++ Triptofano) tem sido considerado factor de risco para FEM.

17
MACRO HISTOLOGIA
• Espessamento fibroso do endocárdio ventricular D e/ou E ++ no ápice e espessamento dos músculos papilares c/ regurgitação valvular;
• Geralmente trombo subjacente;
• Auricula dilatada ++;• Ventriculo pequeno;• 50% ambos ventriculos,
40% apenas o esq e 10% apenas o dir.
• Espessamento pronunciado do endocárdio formado por deposição de colágeno TI cobrindo o endocárdio normal;
• Enfarte subendocárdio;• Degeneração da média, depósitos de
fibrina e fibrose nas artérias coronárias; • Infiltrado crónico inflamatório na interface
entre o miocárdio e endocárdio e á volta dos vasos intersticiais;
• Em mtas necrópsias há falta de celularidade inflamatória no último estadio não há inflamação.
ETIO-FISIOPATOLOGIAPATOLOGIA

18
Dça febril + Pancardite
Hipereosinofilia •Edema facial e periorbital •Prurido corporal •Urticária •Neurological features
Trombose ventricular (++ Ápices e aparelho subvalvular)
Obliteração da cavidade ventricular Interferência com o mecanismo valvular
ETIO-FISIOPATOLOGIAPROGRESSÃO FISIOPATOLÓGICA

19
Organização do Trombo + Fibrose endocárdica (mural e endocárdio valvular)
Dificulta o enchimento ventricular Distorção das válvulas
Fisiologia restritiva •Regurgitação A-V •Ventrículos pequenos • Átrios muito dilatados
IC com: •Congestão venosa •DC persistentemente baixo
ETIO-FISIOPATOLOGIAPROGRESSÃO FISIOPATOLÓGICA

20
CLÍNICA
Depende: Actividade da doença Câmara afectada Gravidade das lesões
Doença activa é sugerida por: Episódio febril recente IC + urticária e edema facial

21
CLÍNICA
FEM VD
Proptose, edema facial Cianose, distensão da veia jugulare hipocratismo digital Atraso de crescimento Caracteres sexuais subdesenvolvidos Icterícia
FA Pulsação paraesternal Sopro de regurgitação tricúspide, S3 Ascite HEM

22
CLÍNICA
FEM VE
Bom estado geral„RDispneia e ortopneia pronunciada„RPequeno deslocamento do apice„RSopro sistolico leve precoce
Estalido de abertura P2 aumentado Sinais de embolismo sistémico

23
CLÍNICA
FEM Bi-ventricular
++ Achados do FEM do VD + sopro de IM HTP (quando envolvimento extenso do VE) Embolização sistémica (15%) Endocardite infecciosa (2%)

24

25
The clinical manifestations of EMF are largely related to the presence of right and/or left heart failure. Patients may report dyspnea on exertion, paroxysmal nocturnal dyspnea, orthopnea, lower extremity, and abdominal swelling. A history of a febrile illness with or without urticaria is occasionally obtained [31].
In Africans with EMF in particular, there is often dramatic ascites (figure 3). Ascites may or may not be accompanied by other signs of right-sided heart failure, such as elevated jugular venous pressure and/or lower extremity edema [32-35]. The high prevalence of malnutrition and hypoalbuminemia may explain the predilection for ascites in this population. In one series, the ascitic fluid protein content was described as exudative in 35 of 47 patients with EMF, and the authors concluded that an inflammatory process might also be contributing [33]. The serum albumin to ascites gradient (which is a more accurate indicator of portal hypertension such as my result from heart failure) was not reported

26
Patients with EMF often also have large pleural and pericardial effusions (picture 1). Severe atrial enlargement leads to the appearance of cardiomegaly on chest radiography. Atrial fibrillation is common in end-stage disease and predicts a poor prognosis [36].

27
Echo — Although clinically similar to Loffler’s endocarditis, the diagnosis of EMF should be reserved for patients from endemic regions without a clearly identified cause for sustained eosinophilia with the classic echo features listed below [37,38]:
Apical fibrosis of the RV, LV, or both ventricles (figure 4 and figure 1 and figure 5)
Tethering the AV valve papillary muscles, leading to mitral and/or tricuspid regurgitation (figure 1)
Giant atrial enlargement (figure 4 and figure 1)
A restrictive filling pattern on Doppler recordings of mitral valve inflow (figure 6)
DIAGNÓSTICO

28
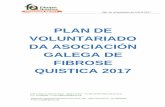
Endomyocardial fibrosis echo
A) Surface echocardiogram with fibrosis and thrombus in the left ventricular apex. B) Transesophageal echocardiogram with biventricular apical fibrosis with involvement of the posterior mitral papillary muscle and a small pericardial effusion.
Schematic of the two-dimensional, four-chamber apical view findings in 10 patients with endmyocardial disease. Numbers on the right and left indicate the number of patients with each finding. IVC: inferior vena cava; MOT: preserved or increased inward motion of the obliterative process; OBL: obliteration; RFL: increased reflectance of the obliterative surface; THICK: increased thickening of the basal inflow tract papillary muscle and/or posterior atrioventricular valve.

29
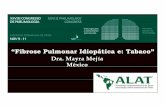
Doppler in restrictive cardiomyopathy
The pulse wave Doppler in a patient with an idiopathic restrictive cardiomyopathy demonstrates an increased E/A ratio (2.4), with shortened deceleration time (DT = 128 milliseconds).
In addition, apical thrombi are often present (figure 7). In EMF, the apex maintains inward systolic contractile motion which may help to differentiate EMF from other causes of apical thrombi associated with an akinetic or dyskinetic apex such as myocardial infarction or Chagas disease [39].

30
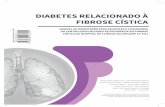
Cardiovascular magnetic resonance imaging of eosinophilic endomyocardial fibrosis
(A) Steady state free precession MRI transverse view through both ventricles two minutes after 0.2-mmol/kg Gd-DTPA infusion. Note the apical filling of the left ventricle by thrombus (*) exhibiting lower signal than adjacent myocardium. (B) Delayed enhanced sequence in the same axis 10 minutes after Gd-DTPA infusion. Subendocardium exhibited high signal (arrows) close to the ventricular thrombus (*).

31
Echo staging of disease — An echocardiographic screening study in Mozambique included echocardiographic criteria for the diagnosis and staging of EMF. As the natural history of EMF is not well defined, these criteria will likely aid in defining the stages of this disease and in determining the clinical significance of the early EMF.
Cardiac catheterization — Cardiac catheterization is not required for the diagnosis of EMF. However on hemodynamic studies a restrictive pattern is observed with diastolic dip and plateau pressure tracings. Depending on the ventricle involved, mitral and tricuspid regurgitation may be demonstrated. Ventricular angiography reveals apical obliteration of the affected ventricle (figure 4) [40].
Cardiovascular magnetic resonance imaging — Cardiovascular magnetic resonance (CMR) imaging with contrast demonstrates myocardial fibrosis (figure 7) [41,42]. However, the utility of this information in addition to echocardiography is unclear, and this modality is generally unavailable in areas with the highest burden of disease. In early disease where there is suspicion for active inflammation, CMR may be useful in identifying patients who may benefit from steroid therapy

32
Endomyocardial fibrosis was diagnosed in the presence of two major criteria or one major criterion associated with two minor criteria was classified as biventricular, right-sided, or left-sided according to whether the structural lesions involved both ventricles without predominance of one side, only or predominantly the right ventricle, or only or
predominantly the left ventricle, respectively. Possible scores ranged from 0 to 35; cases with scores of 8 or less were classified as mild, those with scores of 8 to 15 as moderate, and those with scores of 15 or more as severe.

33
TESTES LABORATORIAIS
Não há testes especícos Hipereosinofilia é variável e mais frequente
nos estadios iniciais da doença ou nas doenças parasitárias.
Hipoalbuminémia mais comum nos estadios avançados da doença
Alterações bioquímicas da disfunçao hepática e/ou renal
Hypoalbuminaemia is Presença de procoagulantes esta em
investigação cá.

34
DIAGNÓSTICOS DIFERENCIAIS

35
MANEJO E TRATAMENTO
The natural history of EMF is not fully defined, and there are few data available to guide therapeutic decisions. Most present to medical care with end-stage disease and suffer an annual mortality as high as 25 percent despite medical treatment [36,43]. Surgical management has led to long-term survival in some patients with EMF [6]; however, this option is unavailable in regions with a high disease burden.
Medical therapy — Available literature is limited to case series that do not fully define treatment regimens [36,43]. A general approach can be extrapolated from the treatment of patients with heart failure due to restrictive diastolic dysfunction from other causes. (See "Treatment and prognosis of diastolic heart failure" and "Definition and classification of the cardiomyopathies", section on 'Restrictive cardiomyopathy'.)
Diuretics and rate control for atrial fibrillation are currently the mainstays of therapy.
Pleural, pericardial or ascitic fluid removal may alleviate symptoms, but these often reaccumulate. In patients with suspected acute carditis, prednisone may be of benefit. (See "Natural history and therapy of myocarditis in adults", section on 'Eosinophilic myocarditis'.)
Surgery — Endomyocardial resection with valve replacement or repair has gained prominence at many centers, especially in subjects in advanced heart failure [6,44,45]. Immediate postoperative mortality is high, ranging from 15 to 30 percent, but surgery offers the possibility of long-term survival [45]. A surgical series of 83 patients from Brazil all in NYHA functional class grade III-IV, and with a mean follow-up of 7.6 years had a survival probability at 17 years of 55 percent [6]. Published series have been small, overall experience is limited, and questions remain about the appropriate timing, peri-operative mortality, and long-term prognosis (figure 2 and figure 8). Cardiac surgery is not routinely available in areas with high EMF prevalence.

36
TTO MEDICO
Baseado em série de casos
Abordagem geral extrapolada do tratamento dos pacientes com IC devido a disfunção diastólica restritiva por outras causas
O tratamento é baseado no uso de diuréticos (Espirinolactona) e controle da FC nos doentes com FA (Digoxina e β-bloqueadores), IECAS
Toracocentese, Pericardiocentese, paracentese Prednisolona (7 – 10 dias) em doentes com
suspeita de Cardite aguda AAS

37
TTO CIRURGICO
Ressecção endomiocárdica + substituição ou reparação valvular
Recomendado a todos pacientes em classe funcional III-IV (NYHA)
Mortalidade pós-operatória imediata alta (15 – 30%)
▪< se não for necessário substituição valvular
Sobrevivência a longo termo alta Fibrose pode re-ocorrer

38
Endomyocardial fibrosis surgery
A) Surface echocardiogram with left ventricular apical fibrosis and severe left and right atrial enlargement. B) Postoperative.

39
PROGNÓSTICO
1/3 – ½ dos doentes com doença avançada morrem em 2 anos. Pouco sintomáticos teem maior sobrevida.
FA e Ascite são sinais de mau prognóstico. Doentes morrem por IC progressiva, morte
súbita cardíaca (TE e Arritmias) e complicações cirúrgicas.

40
BIBLIOGRAFIA
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed., volume 1, 2007
Mocumbi AO, Yacoub S, Yacoub M. Myocardial disease. Neglected tropical cardiomyopathies II – Endomyocardial fibrosis. Heart 2008;000:1–8. doi:10.1136/hrt.2007.136101
Rebecca Cogswell, MD, Gene Bukhman, MD, PhD, Nelson B Schiller, MD Harry Acquatella, MD, FACC, FAHA: Endomyocardial fibrosis.
www.uptodate.com Mocumbi AO, Ferreira MB, Sidi D, yacoub MH. A
population study of endomyocardial fibrosis in rural area of Mozambique. N Engl J Med 2008; 359:43

41
Leslie T Cooper, Jr, MD: Definition and classification of the cardiomyopathies
www.uptodate.com Mocumbi AO, Carrilho C, . Sarathchandra P,
Ferreira B, Yacoub M, Burke M. Echocardiography accurately assesses the pathological,abnormalities of chronic endomyocardial fibrosis.Int J Cardiovasc Imaging, 2010; DOI 10.1007/s10554-010-9753-6,
Mocumbi AO, Latif N, Yacoub MH. Presence of circulating anti-myosin antibodies in endomyocardial fibrosis. PLoS Negl Trop Dis 2010; 4:e661
Top Related