







Idiomas
Páginas
Jurídico

Terapia dirigida anti-diana en el tratamiento
de los sarcomas
Mª Angeles Vaz Salgado
Hospital Universitario Ramón y Cajal
No tenemos: Trastuzumab Erlotinib Vemurafenib Cetuximab Nivolumab etc
Sí tenemos: Imatinib y otros en GIST Nuevos fármacos antidiana Ttos dirigidos en tumores infrecuentes etc
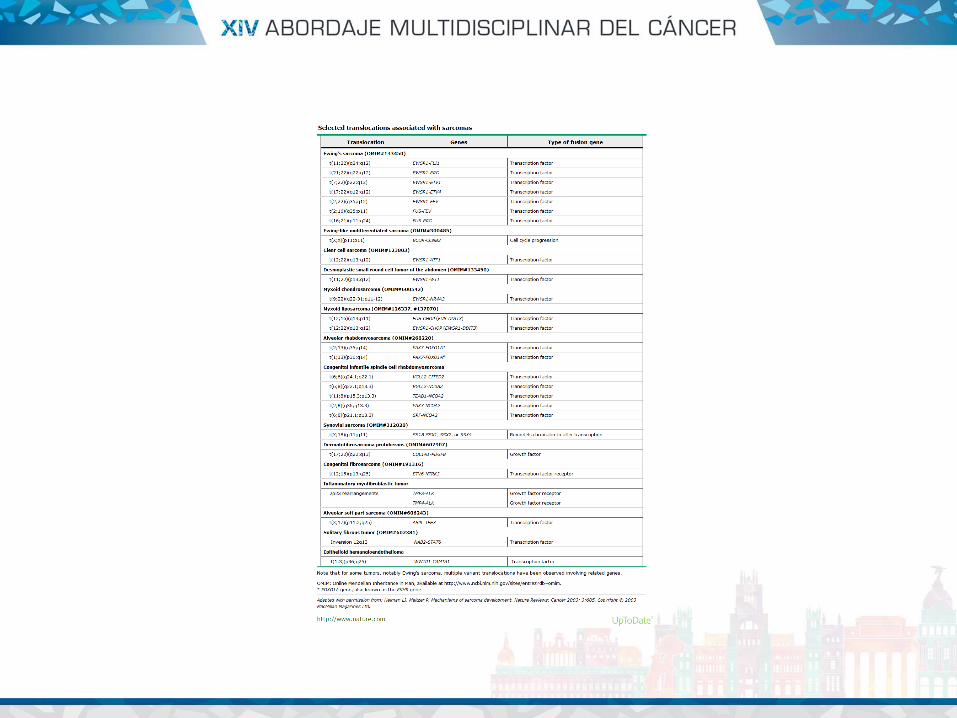
• Es una enfermedad rara
• Es una enfermedad heterogénea.
– 80 subtipos de sarcomas de hueso y partes blandas.
• Es una enfermedad de mal pronóstico en el contexto metastásico
• Del proyecto europeo RARECARE (n=45.568)
– Incidencia de 5.6/100.000 hab/año
• Para sarcomas de partes blandas 4.7/100.000 hab
• 84% sarcomas partes blandas, 14% óseos
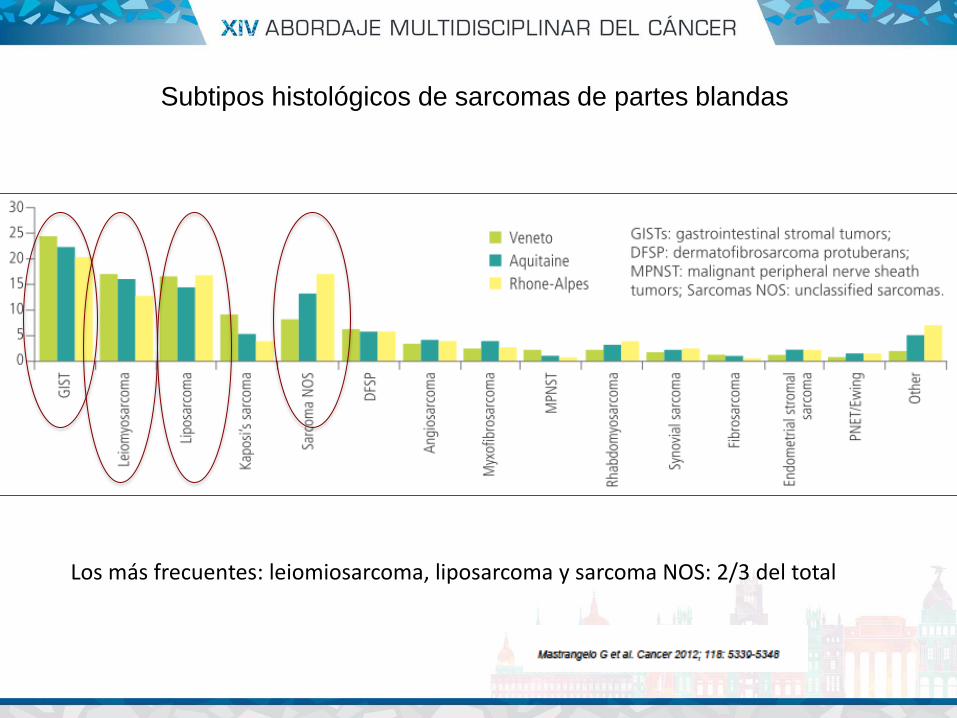
Subtipos histológicos de sarcomas de partes blandas
Los más frecuentes: leiomiosarcoma, liposarcoma y sarcoma NOS: 2/3 del total
• COMPLEJO – Alteraciones genéticas múltiples complejas.
• SIMPLE • Translocaciones específicas que generan genes de fusión
(sarcoma sinovial, liposarcoma mixoide, s ewing…)
• Mutaciones específicas de kinasas (GIST)
• Inactivación de genes (NF1 en MPNST, INI1 en tumor rabdoide, APC en tumor desmoide).
• Alteraciones genéticas simples (amplificación de MDM2/CDK4 en liposarcoma bien diferenciado/desdiferenciado).
SARCOMAS. GRUPOS BIOLOGICOS

• Antes: “una mismo fármaco para todos igual”
• Ahora: avances genéticos y biológicos indican que los sarcomas son diferentes enfermedades.
• Los tratamientos pueden seleccionarse por histotipos y/o por dianas moleculares
– tratamientos dirigidos por histotipos.
– Tratamientos antidiana
TRATAMIENTO SISTEMICO DIRIGIDO
TRATAMIENTO SISTEMICO DIRIGIDO
• Podemos considerar que la quimioterapia sigue siendo el pilar del tratamiento en los pacientes con enfermedad metastásica no resecable. – Antraciclinas – Ifosfamida
– Combinaciones de Gemcitabina (docetaxel/dacarbazina) – Pazopanib – Trabectedina – Eribulina
• Quimiosensibles: sarcoma sinovial, liposarcoma mixoide,
leiomiosarcoma uterino.
• Quimioresistentes: sarcoma alveolar de partes blandas,
sarcoma de células claras, sarcoma fibromixoide de bajo grado, condrosarcoma mixoide extraesquelético.
Tratamiento dirigido por histotipo
• Primera línea – Basado de antraciclinas:
• Doxorrubicina monoterapia • Doxorrubicina-ifosfamida • Doxorrubicina-olaratumab
• Segunda línea y sucesivas: Basado en subtipo histológico
– Leiomiosarcomas : trabectedina. combinaciones con gemcitabina y pazopanib
(eribulina no indicacion en leiomiosarcoma) – Liposarcoma mixoide: trabectedina, eribulina (pazopanib no aprobada en
liposarcoma) – Sarcoma pleomorfico: ifosfamida, combinaciones con gemcitabina/docetaxel
(pazopanib/trabectedina) – Sarcoma sinovial: trabectedina, pazopanib, ifos rechallenge – Angiosarcoma: doxorubicina o taxol, combinaciones con gemcitabina
Tratamiento dirigido por histología
• Sarcomas de partes blandas más habituales – Aprobados: olaratumab, pazopanib
• Sarcomas de partes blandas “raros/infrecuentes” – Dermatofibrosarcoma protuberans: imatinib – Tumor miofibroblastico inflamatorio: Inh ALK – Sarcoma alveolar de partes blandas:
sunitinib/pazopanib/cediranib Sarcomas óseos
• Inmunoterapia • GIST
– Imatinib
TRATAMIENTOS DIRIGIDOS ANTIDIANA
TRATAMIENTOS DIRIGIDOS ANTIDIANA
• Sarcomas de partes blandas más habituales –Aprobados: olaratumab, pazopanib
• Sarcomas de partes blandas “raros”
– Dermatofibrosarcoma protuberans: imatinib – Tumor miofibroblastico inflamatorio: Inh ALK – Sarcoma alveolar de partes blandas: sunitinib/pazopanib/cediranib
• Sarcomas óseos • GIST
– Imatinib
• El título de la charla nos lleva a ver con más detenimiento este fármaco de reciente introducción:
– OLARATUMAB
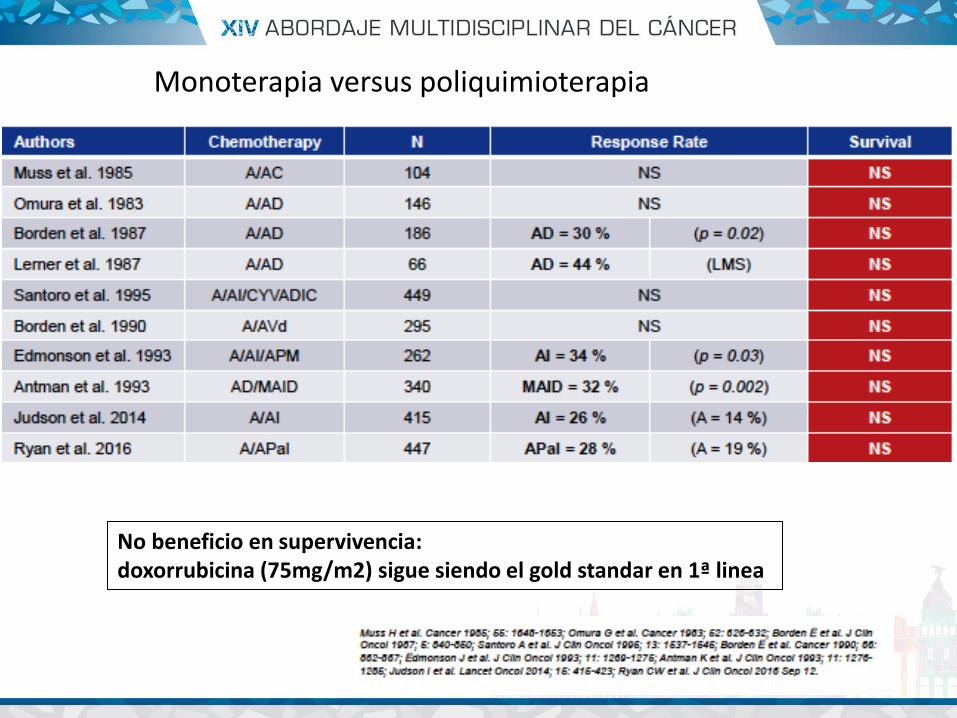
Monoterapia versus poliquimioterapia
No beneficio en supervivencia: doxorrubicina (75mg/m2) sigue siendo el gold standar en 1ª linea
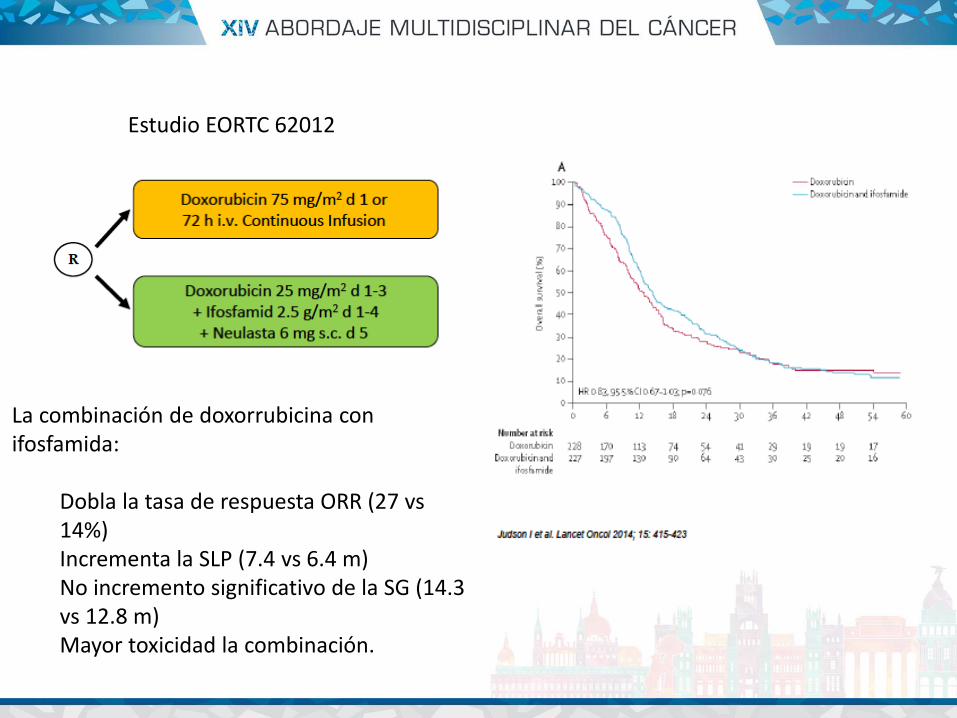
Estudio EORTC 62012
La combinación de doxorrubicina con ifosfamida:
Dobla la tasa de respuesta ORR (27 vs 14%) Incrementa la SLP (7.4 vs 6.4 m) No incremento significativo de la SG (14.3 vs 12.8 m) Mayor toxicidad la combinación.
DOXORRUBICINA SIGUE SIENDO EL GOLD ESTANDAR
LA DECISIÓN DEBE BASARSE EN EL OBJETIVO DE TRATAMIENTO: - Si es el control de la enfermedad, Doxorrubicina sola es el tratamiento de
elección. - Si se busca reduccion de la enfermedad o respuesta, para aliviar síntomas o
ir a una cirugía, la combinación puede ser mejor.
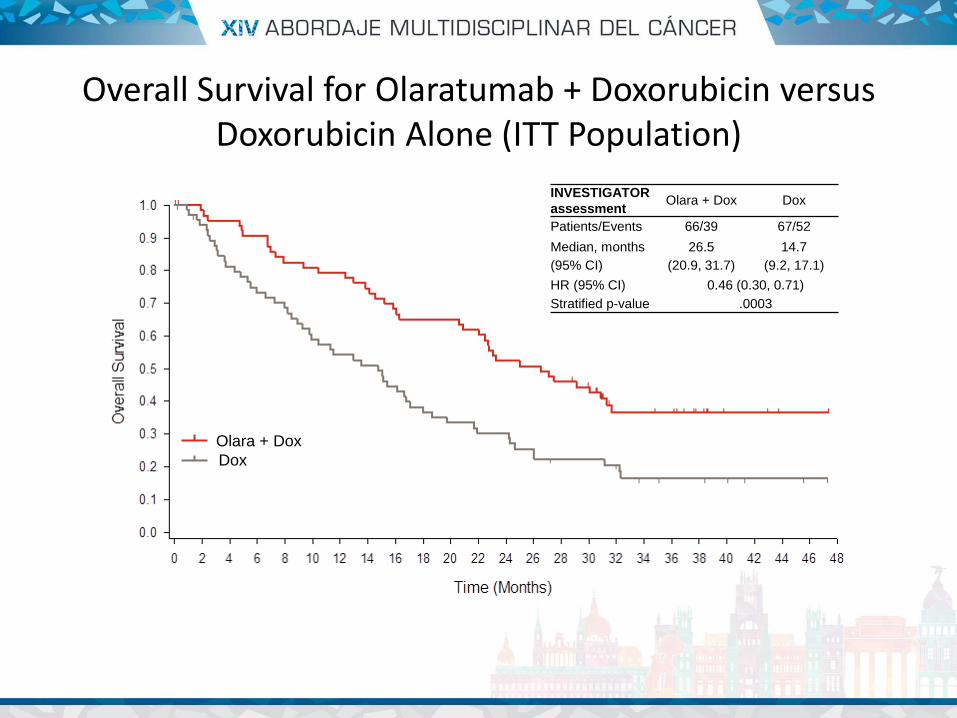
INVESTIGATOR
assessment Olara + Dox Dox
Patients/Events 66/39 67/52
Median, months
(95% CI)
26.5
(20.9, 31.7)
14.7
(9.2, 17.1)
HR (95% CI) 0.46 (0.30, 0.71)
Stratified p-value .0003
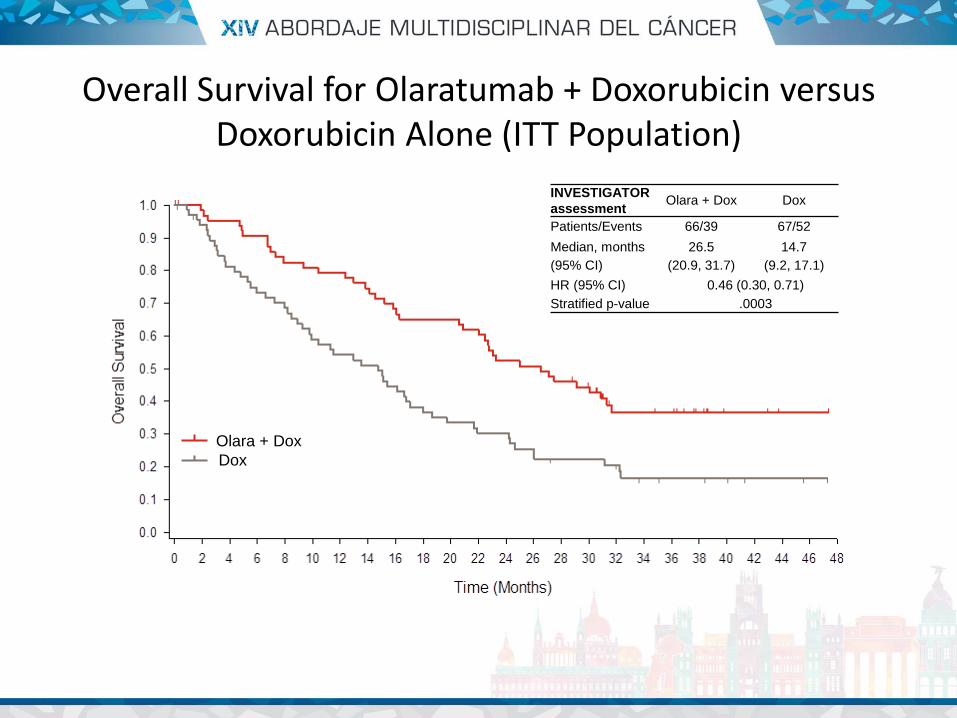
Overall Survival for Olaratumab + Doxorubicin versus Doxorubicin Alone (ITT Population)
Olara + Dox
Dox
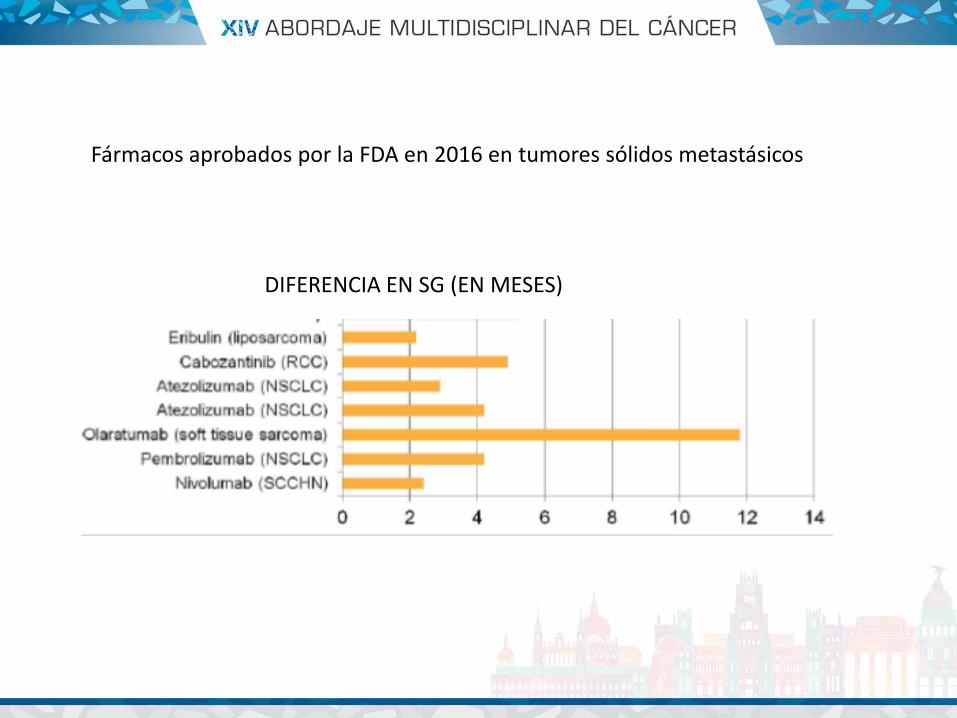
Fármacos aprobados por la FDA en 2016 en tumores sólidos metastásicos
DIFERENCIA EN SG (EN MESES)
• La señal de PDGF/PDGFR tiene un papel importante en la biologia mesenquimal normal – Promueve diferenciación en celulas stem mesenquimales, crecimiento de
células mesenquimales, angiogénesis y cicatrización.
• Efecto tumoral – PDGFRa está geneticamente alterado o sobreexpresado en multiples tumores
(incluido sarcoma) – La expresión de PDGFRa se asocia a un aumento del potencial metastasico – Funciona como una via autocrina o paracrina facilitando el crecimiento de los
tumores
• Efectos sobre el estroma – Su efecto en las células estromales contribuye a la angiogénesis – Al unirse el ligando al receptor en las células estromales promueve el
crecimiento celular
Datos preclinicos
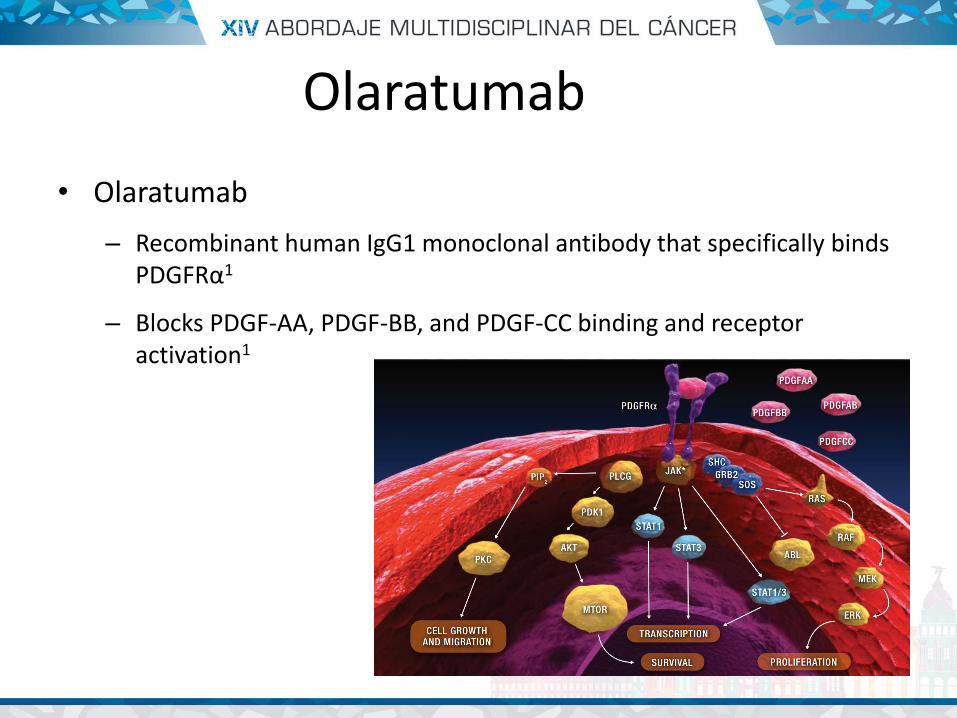
• Olaratumab
– Recombinant human IgG1 monoclonal antibody that specifically binds PDGFRα1
– Blocks PDGF-AA, PDGF-BB, and PDGF-CC binding and receptor activation1
Olaratumab
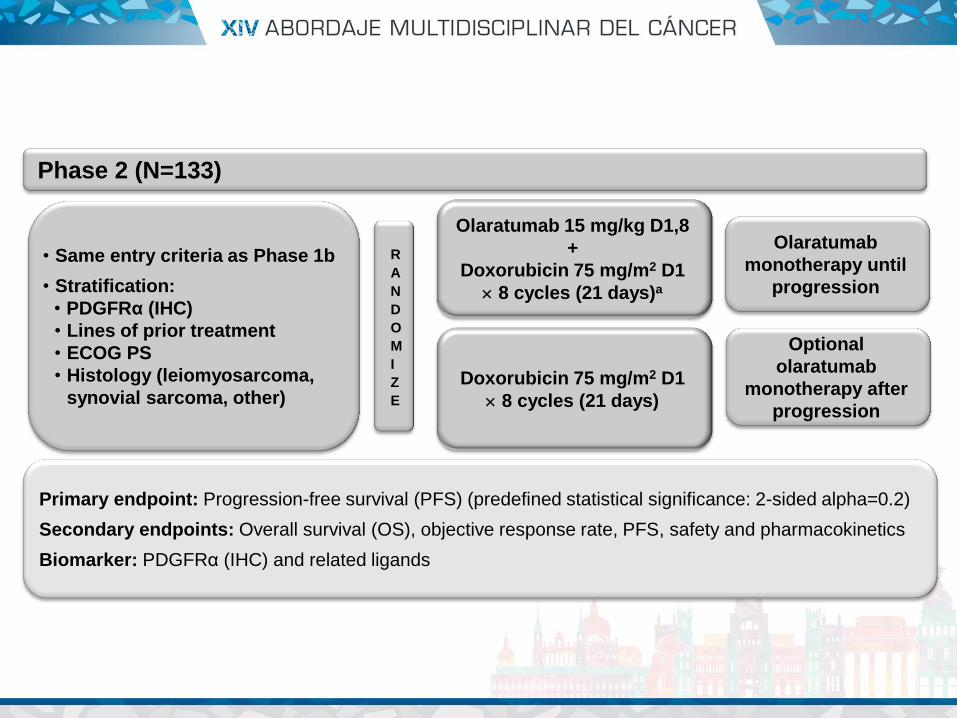
R
A
N
D
O
M
I
Z
E
Olaratumab
monotherapy until
progression
Olaratumab 15 mg/kg D1,8
+
Doxorubicin 75 mg/m2 D1
8 cycles (21 days)a
Optional
olaratumab
monotherapy after
progression
Doxorubicin 75 mg/m2 D1
8 cycles (21 days)
• Same entry criteria as Phase 1b
• Stratification:
• PDGFRα (IHC)
• Lines of prior treatment
• ECOG PS
• Histology (leiomyosarcoma,
synovial sarcoma, other)
Phase 2 (N=133)
Primary endpoint: Progression-free survival (PFS) (predefined statistical significance: 2-sided alpha=0.2)
Secondary endpoints: Overall survival (OS), objective response rate, PFS, safety and pharmacokinetics
Biomarker: PDGFRα (IHC) and related ligands
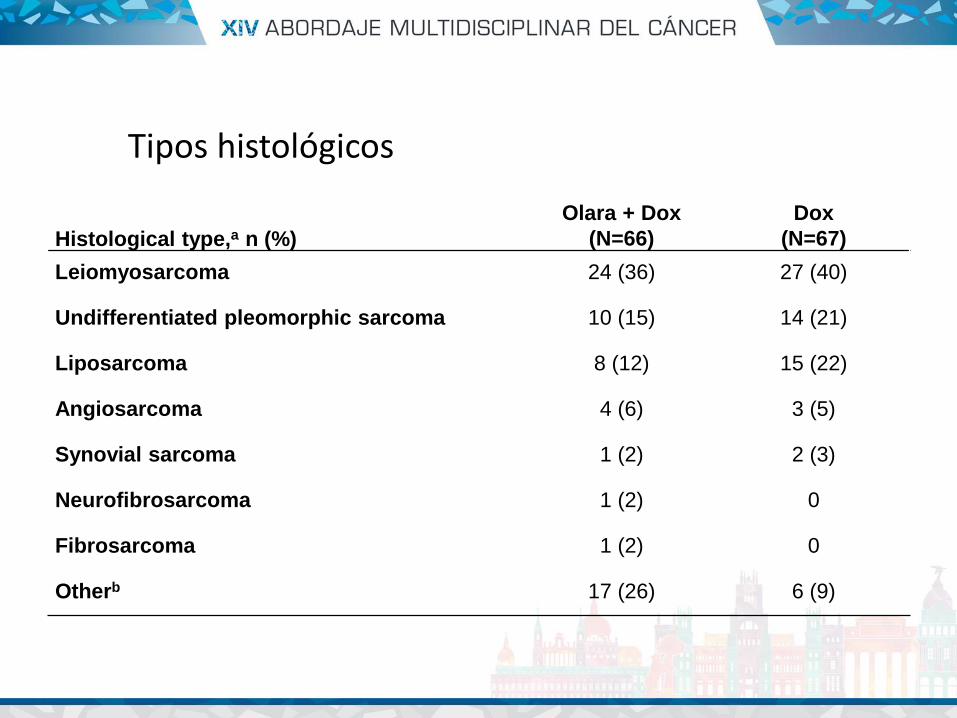
Histological type,a n (%)
Olara + Dox
(N=66)
Dox
(N=67)
Leiomyosarcoma 24 (36) 27 (40)
Undifferentiated pleomorphic sarcoma 10 (15) 14 (21)
Liposarcoma 8 (12) 15 (22)
Angiosarcoma 4 (6) 3 (5)
Synovial sarcoma 1 (2) 2 (3)
Neurofibrosarcoma 1 (2) 0
Fibrosarcoma 1 (2) 0
Otherb 17 (26) 6 (9)
Tipos histológicos
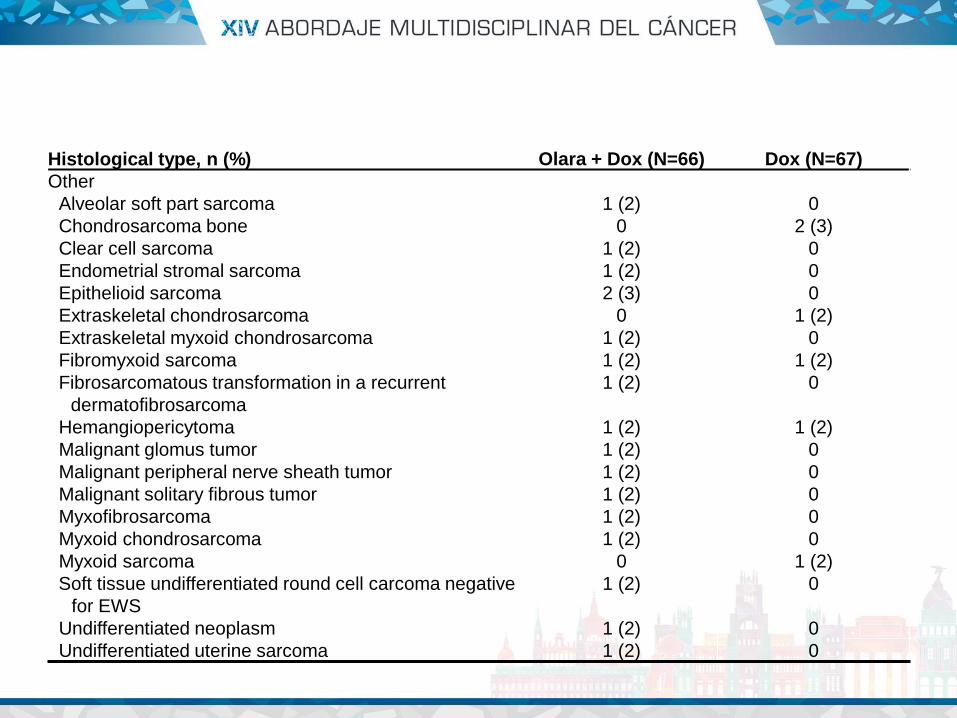
Histological type, n (%) Olara + Dox (N=66) Dox (N=67)
Other
Alveolar soft part sarcoma 1 (2) 0
Chondrosarcoma bone 0 2 (3)
Clear cell sarcoma 1 (2) 0
Endometrial stromal sarcoma 1 (2) 0
Epithelioid sarcoma 2 (3) 0
Extraskeletal chondrosarcoma 0 1 (2)
Extraskeletal myxoid chondrosarcoma 1 (2) 0
Fibromyxoid sarcoma 1 (2) 1 (2)
Fibrosarcomatous transformation in a recurrent
dermatofibrosarcoma
1 (2) 0
Hemangiopericytoma 1 (2) 1 (2)
Malignant glomus tumor 1 (2) 0
Malignant peripheral nerve sheath tumor 1 (2) 0
Malignant solitary fibrous tumor 1 (2) 0
Myxofibrosarcoma 1 (2) 0
Myxoid chondrosarcoma 1 (2) 0
Myxoid sarcoma 0 1 (2)
Soft tissue undifferentiated round cell carcoma negative
for EWS
1 (2) 0
Undifferentiated neoplasm 1 (2) 0
Undifferentiated uterine sarcoma 1 (2) 0
Olara + Dox
Dox
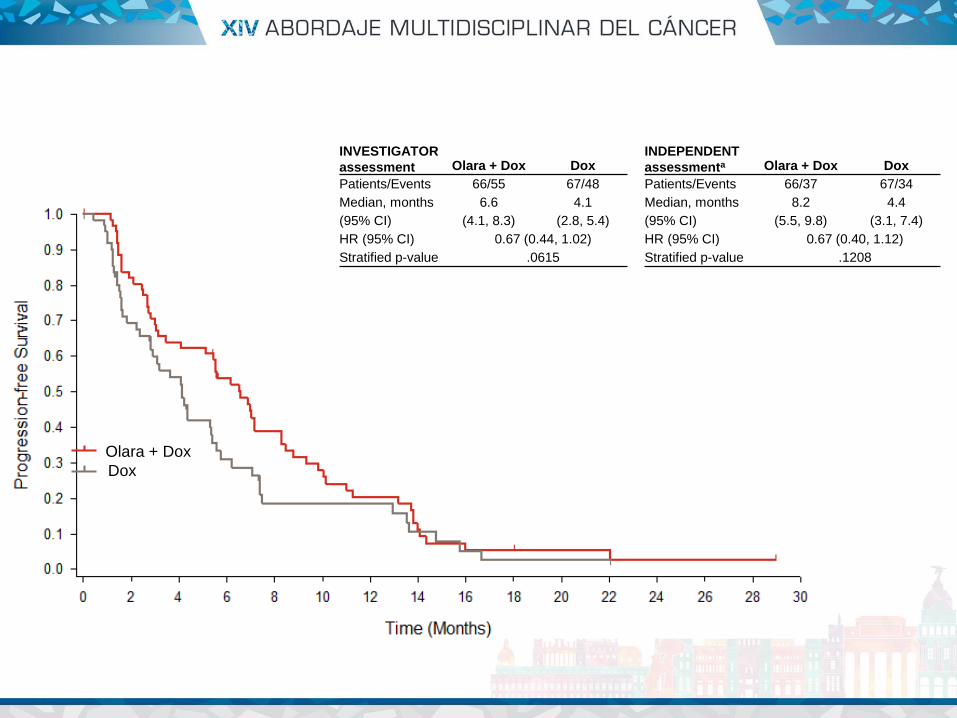
INVESTIGATOR
assessment Olara + Dox Dox
Patients/Events 66/55 67/48
Median, months
(95% CI)
6.6
(4.1, 8.3)
4.1
(2.8, 5.4)
HR (95% CI) 0.67 (0.44, 1.02)
Stratified p-value .0615
INDEPENDENT
assessmenta Olara + Dox Dox
Patients/Events 66/37 67/34
Median, months
(95% CI)
8.2
(5.5, 9.8)
4.4
(3.1, 7.4)
HR (95% CI) 0.67 (0.40, 1.12)
Stratified p-value .1208
Olara + Dox
Dox
INVESTIGATOR
assessment Olara + Dox Dox
Patients/Events 66/39 67/52
Median, months
(95% CI)
26.5
(20.9, 31.7)
14.7
(9.2, 17.1)
HR (95% CI) 0.46 (0.30, 0.71)
Stratified p-value .0003
Overall Survival for Olaratumab + Doxorubicin versus Doxorubicin Alone (ITT Population)
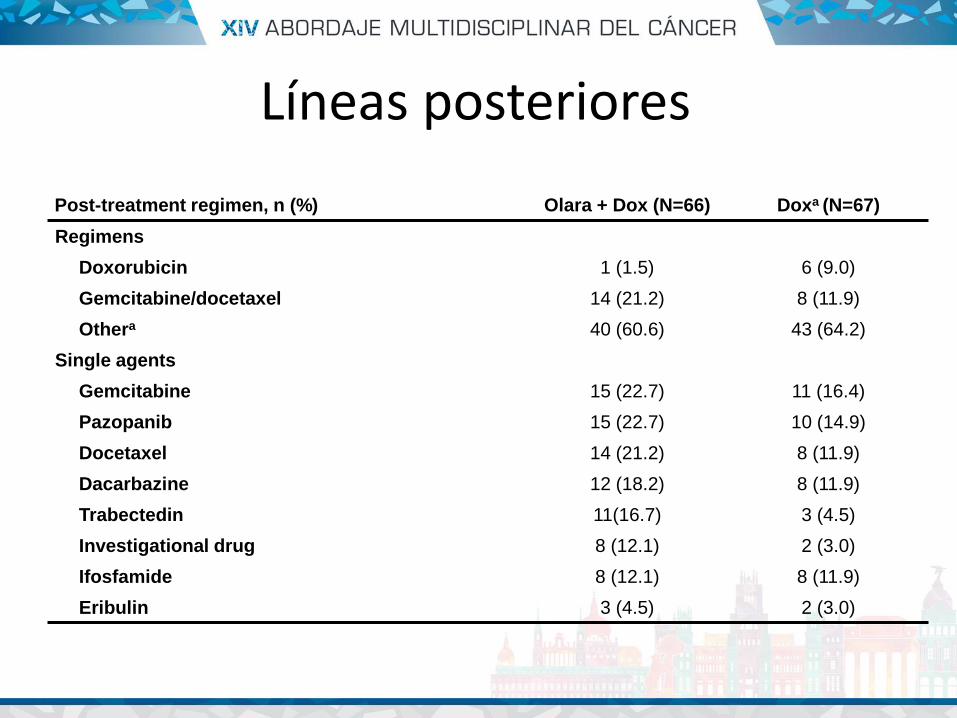
Post-treatment regimen, n (%) Olara + Dox (N=66) Doxa (N=67)
Regimens
Doxorubicin 1 (1.5) 6 (9.0)
Gemcitabine/docetaxel 14 (21.2) 8 (11.9)
Othera 40 (60.6) 43 (64.2)
Single agents
Gemcitabine 15 (22.7) 11 (16.4)
Pazopanib 15 (22.7) 10 (14.9)
Docetaxel 14 (21.2) 8 (11.9)
Dacarbazine 12 (18.2) 8 (11.9)
Trabectedin 11(16.7) 3 (4.5)
Investigational drug 8 (12.1) 2 (3.0)
Ifosfamide 8 (12.1) 8 (11.9)
Eribulin 3 (4.5) 2 (3.0)
Líneas posteriores
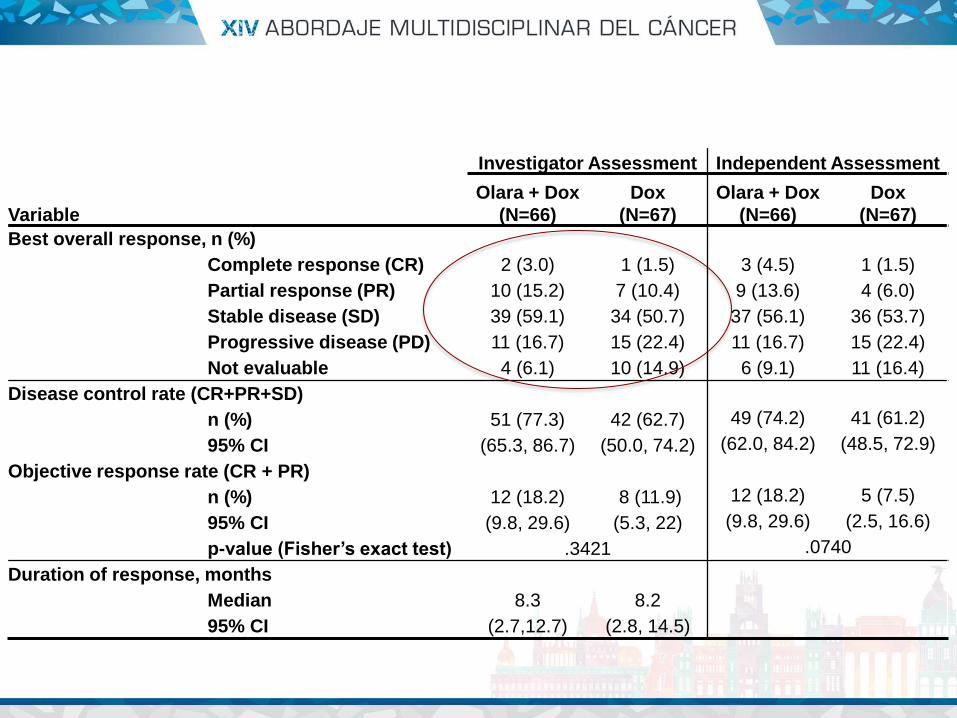
Investigator Assessment Independent Assessment
Variable
Olara + Dox
(N=66)
Dox
(N=67)
Olara + Dox
(N=66)
Dox
(N=67)
Best overall response, n (%)
Complete response (CR) 2 (3.0) 1 (1.5) 3 (4.5) 1 (1.5)
Partial response (PR) 10 (15.2) 7 (10.4) 9 (13.6) 4 (6.0)
Stable disease (SD) 39 (59.1) 34 (50.7) 37 (56.1) 36 (53.7)
Progressive disease (PD) 11 (16.7) 15 (22.4) 11 (16.7) 15 (22.4)
Not evaluable 4 (6.1) 10 (14.9) 6 (9.1) 11 (16.4)
Disease control rate (CR+PR+SD)
n (%) 51 (77.3) 42 (62.7) 49 (74.2) 41 (61.2)
95% CI (65.3, 86.7) (50.0, 74.2) (62.0, 84.2) (48.5, 72.9)
Objective response rate (CR + PR)
n (%) 12 (18.2) 8 (11.9) 12 (18.2) 5 (7.5)
95% CI (9.8, 29.6) (5.3, 22) (9.8, 29.6) (2.5, 16.6)
p-value (Fisher’s exact test) .3421 .0740
Duration of response, months
Median 8.3 8.2
95% CI (2.7,12.7) (2.8, 14.5)
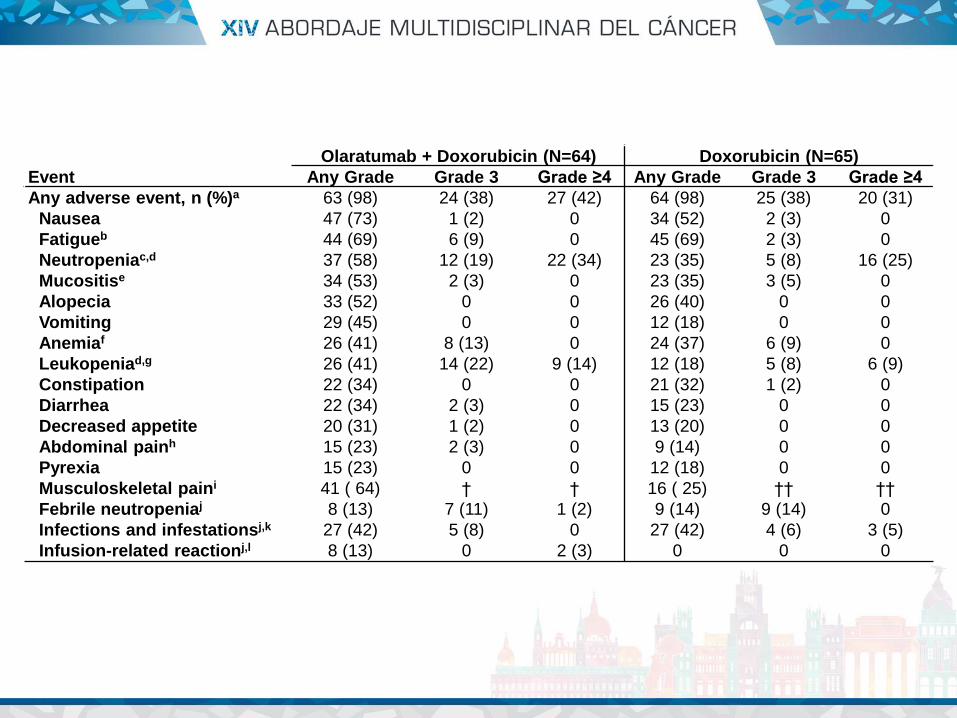
Event
Olaratumab + Doxorubicin (N=64) Doxorubicin (N=65)
Any Grade Grade 3 Grade ≥4 Any Grade Grade 3 Grade ≥4
Any adverse event, n (%)a 63 (98) 24 (38) 27 (42) 64 (98) 25 (38) 20 (31)
Nausea 47 (73) 1 (2) 0 34 (52) 2 (3) 0
Fatigueb 44 (69) 6 (9) 0 45 (69) 2 (3) 0
Neutropeniac,d 37 (58) 12 (19) 22 (34) 23 (35) 5 (8) 16 (25)
Mucositise 34 (53) 2 (3) 0 23 (35) 3 (5) 0
Alopecia 33 (52) 0 0 26 (40) 0 0
Vomiting 29 (45) 0 0 12 (18) 0 0
Anemiaf 26 (41) 8 (13) 0 24 (37) 6 (9) 0
Leukopeniad,g 26 (41) 14 (22) 9 (14) 12 (18) 5 (8) 6 (9)
Constipation 22 (34) 0 0 21 (32) 1 (2) 0
Diarrhea 22 (34) 2 (3) 0 15 (23) 0 0
Decreased appetite 20 (31) 1 (2) 0 13 (20) 0 0
Abdominal painh 15 (23) 2 (3) 0 9 (14) 0 0
Pyrexia 15 (23) 0 0 12 (18) 0 0
Musculoskeletal paini 41 ( 64) † † 16 ( 25) †† ††
Febrile neutropeniaj 8 (13) 7 (11) 1 (2) 9 (14) 9 (14) 0
Infections and infestationsj,k 27 (42) 5 (8) 0 27 (42) 4 (6) 3 (5)
Infusion-related reactionj,l 8 (13) 0 2 (3) 0 0 0


• Tratamiento de segunda línea (sarcomas más habituales)
– Pazopanib
– Trabectedina (Yondelis)
– Eribulina
– Dobletes con gemcitabina (dacarbazina/docetaxel)
• Los pacientes con SPB tienen elevada expresión de VEGF
• Expresión aumentada a mayor grado tumoral y peor supervivencia libre de mts y SG
PAZOPANIB
Potti et al. J Cancer Res Clin Oncol 2004:52 Pakoset al. Anticancer Res 2005:3591 Yudoh et al Br J Cancer 2001:1610 Yoon SS et al Ann Oncol 2004:1261
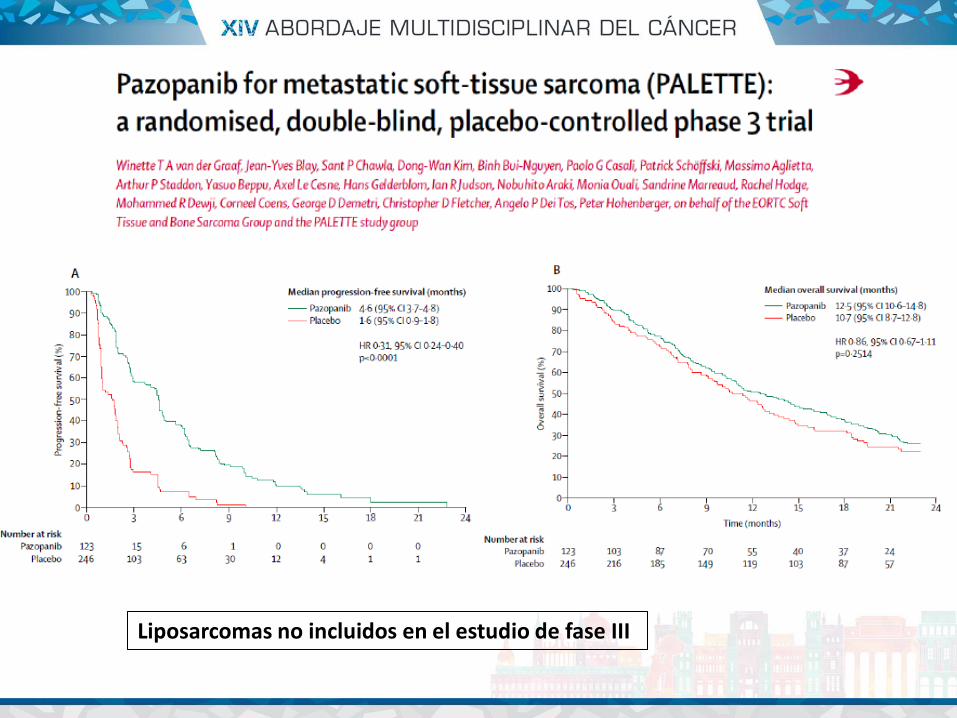
Liposarcomas no incluidos en el estudio de fase III
• Tambien se ha testado la eficacia de pazopanib en liposarcomas en un estudio de fase II (GEIS-ASCO2016) – SLP 3 meses: 43.2% (WD/DD; N=37) – SLP 3 meses: 13.3 % (LPS mixoide/RC; N=15)
• Conclusiones: pazopanib fue bien tolerado y puede ser activo en WD/DD como en otros subtupos de sarcomas (pero no en LPS mixoide/RC) Sleifer S, et al. J Clin Oncol 2009;27:3126-32.
Penel N, et al. J Clin Oncol 34, 2016 (suppl; abstr 11003)
Valverde C, et al. J Clin Oncol 34; 2016 (suppl: abst 11039)
• Sarcomas de partes blandas más habituales – Aprobados: olaratumab, pazopanib
• Sarcomas de partes blandas “raros” – Dermatofibrosarcoma protuberans: imatinib – Tumor miofibroblastico inflamatorio: Inh ALK – Sarcoma alveolar de partes blandas:
sunitinib/pazopanib/cediranib • Sarcomas óseos • GIST
– Imatinib
TRATAMIENTOS DIRIGIDOS ANTIDIANA
• Soporte científico
– ¿el agente antidiana es capaz de actuar directamente en su diana? Datos preclínicos
– ¿qué datos clínicos tenemos? ¿qué tipo de estudios?
• Retrospectivo
• Prospectivo controlado (P-C)
• Prospectivo no controlado (P-NC)
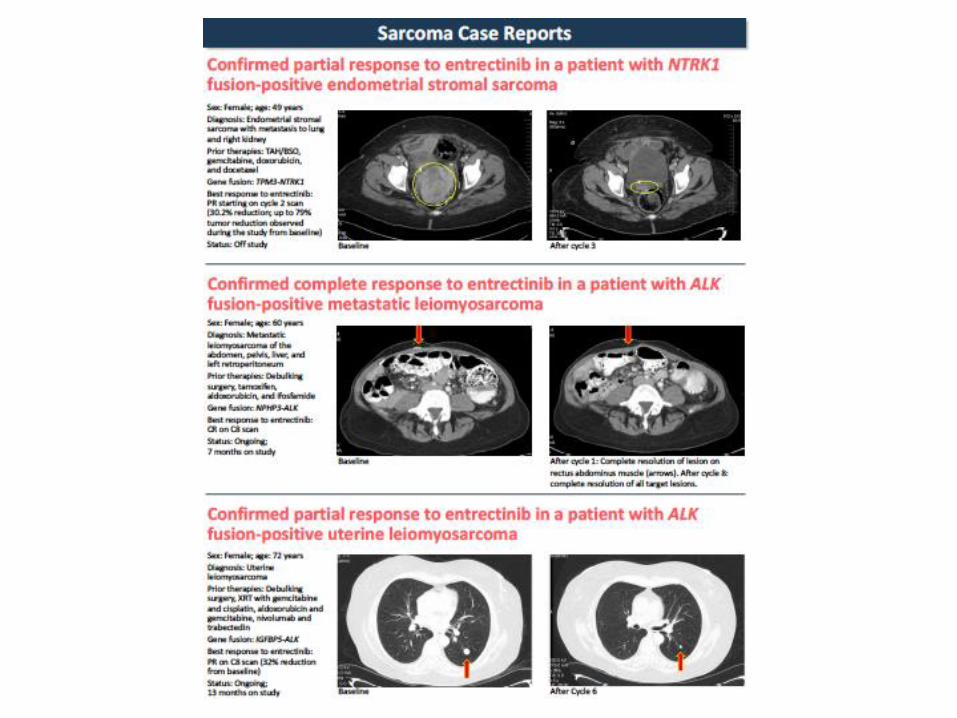
Agentes antidiana en sarcomas infrecuentes
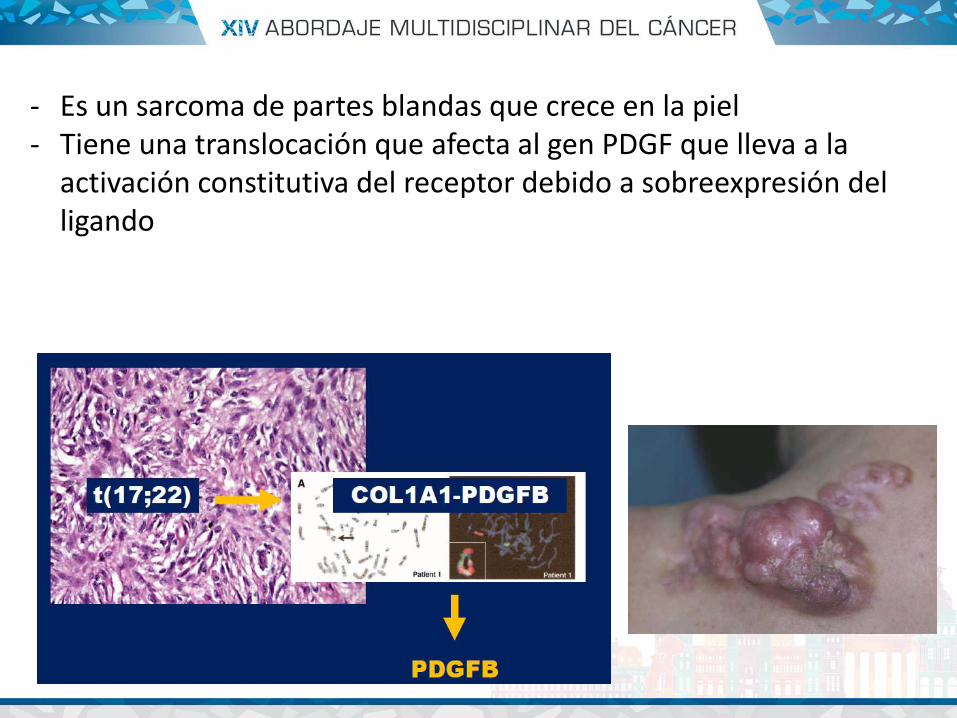
- Es un sarcoma de partes blandas que crece en la piel - Tiene una translocación que afecta al gen PDGF que lleva a la
activación constitutiva del receptor debido a sobreexpresión del ligando
IMATINIB N=24 Tasa respuesta: 50% SLP (mediana): 1.7 años P-NC
IMATINIB N=16 Fase II RR: 50% No mejoria de margenes qx P-NC. Neoadyuvancia
IMATINIB N= 10. Retrospectivo RP:8/10 EE:1/10 Retrospectivo
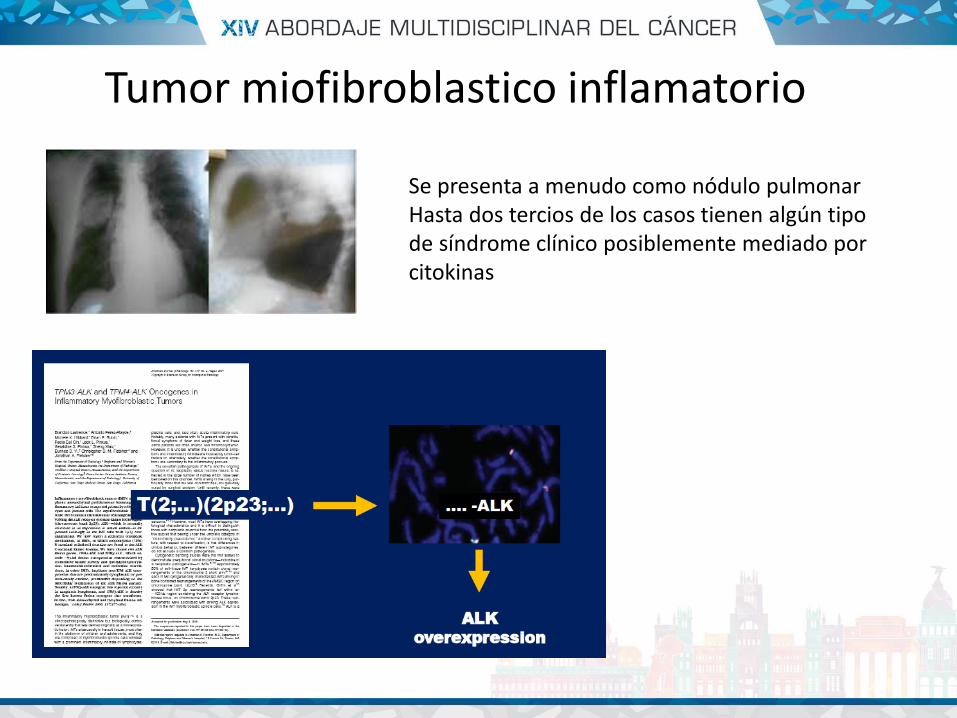
Se presenta a menudo como nódulo pulmonar Hasta dos tercios de los casos tienen algún tipo de síndrome clínico posiblemente mediado por citokinas
Tumor miofibroblastico inflamatorio
CRIZOTINIB A la espera de EC prospectivo N= 20 pac Retrospectivos
CERITINIB Respuesta en PG a crizotinib Fase II en marcha

Tumor raro <1% de todos los sarcomas - Curso clinico indolente pero alto potencial metastásico - Translocación específica: t(X;17); (p11;q25) - Quimioresistente
SARCOMA ALVEOLAR DE PARTES BLANDAS
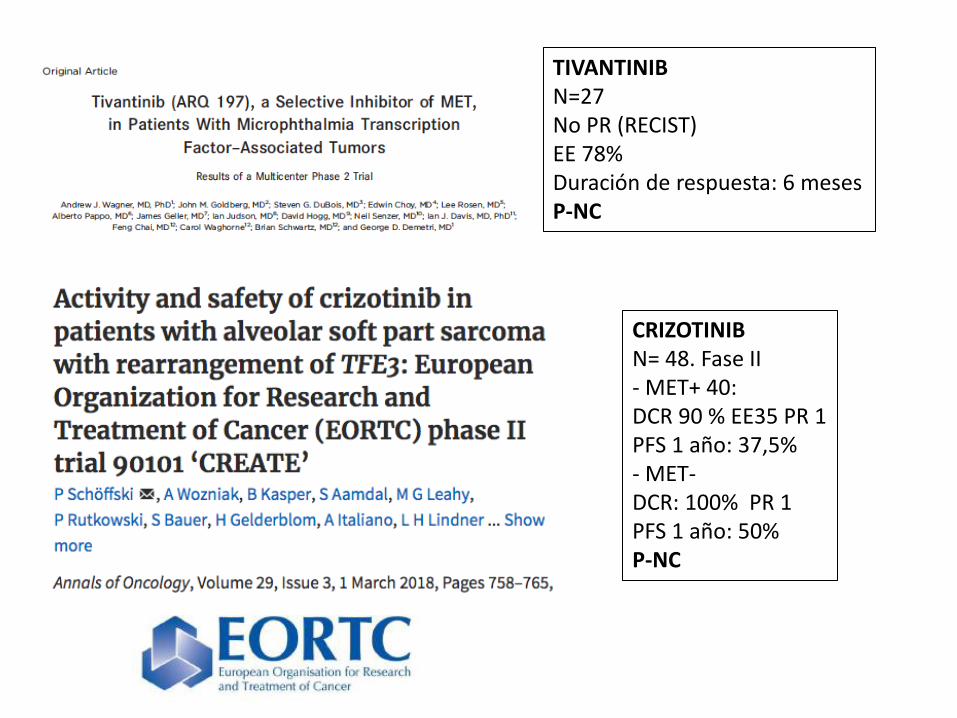
TIVANTINIB N=27 No PR (RECIST) EE 78% Duración de respuesta: 6 meses P-NC
CRIZOTINIB N= 48. Fase II - MET+ 40: DCR 90 % EE35 PR 1 PFS 1 año: 37,5% - MET- DCR: 100% PR 1 PFS 1 año: 50% P-NC
Antiangiogénicos
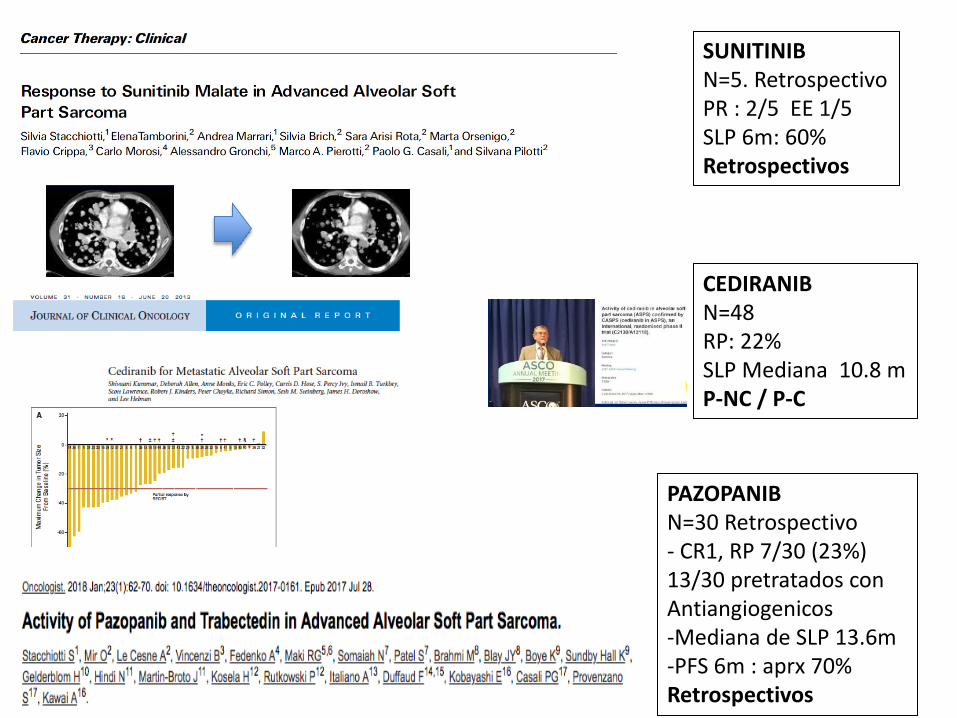
SUNITINIB N=5. Retrospectivo PR : 2/5 EE 1/5 SLP 6m: 60% Retrospectivos
CEDIRANIB N=48 RP: 22% SLP Mediana 10.8 m P-NC / P-C
PAZOPANIB N=30 Retrospectivo - CR1, RP 7/30 (23%) 13/30 pretratados con Antiangiogenicos -Mediana de SLP 13.6m -PFS 6m : aprx 70% Retrospectivos
• Hemangioendotelima epitelioide: t(1;3)(p36;q25): CAMTA1 (no tratamiento dirigido) – Bevacizumab – Sorafenib – pazopanib
• Tumor fibroso solitario: inv (12)(q13): sobreexpresión de STAT6 (no tratamiento dirigido) – Temozolomida-bevacizumab – Sunitinib – Sorafenib – Pazopanib – axitinib
Otros
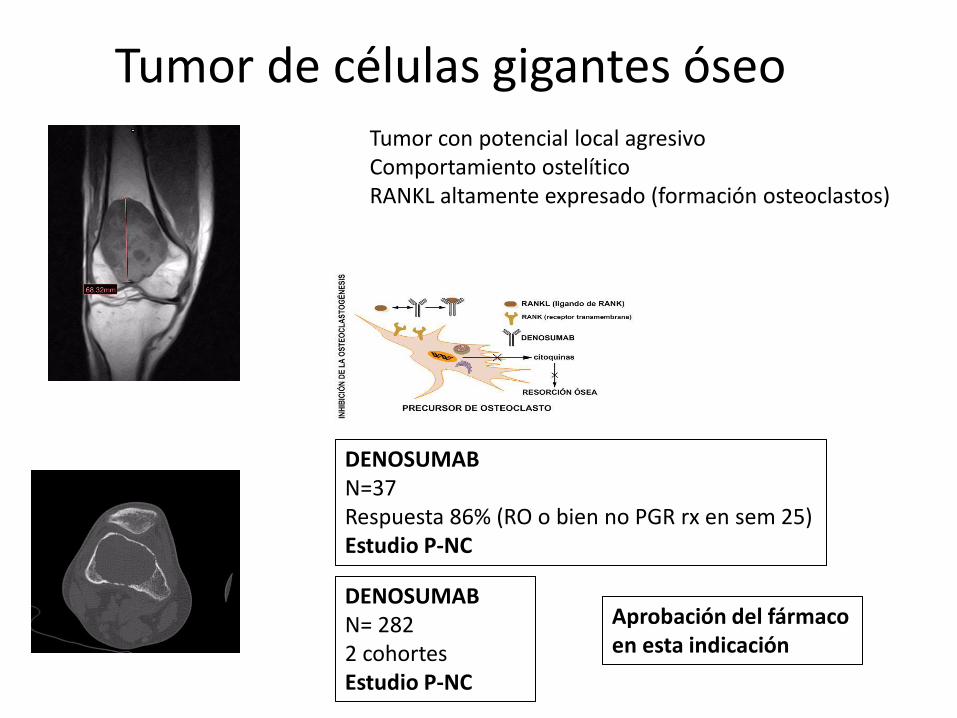
Tumor de células gigantes óseo Tumor con potencial local agresivo Comportamiento ostelítico RANKL altamente expresado (formación osteoclastos)
DENOSUMAB N=37 Respuesta 86% (RO o bien no PGR rx en sem 25) Estudio P-NC
DENOSUMAB N= 282 2 cohortes Estudio P-NC
Aprobación del fármaco en esta indicación
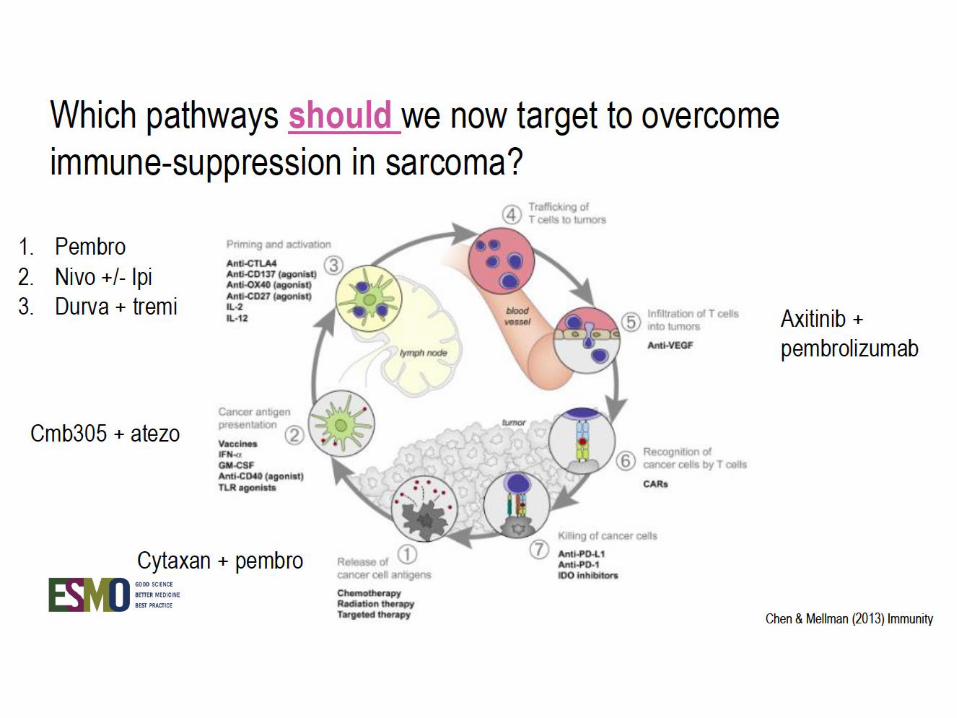
Inmunoterapia
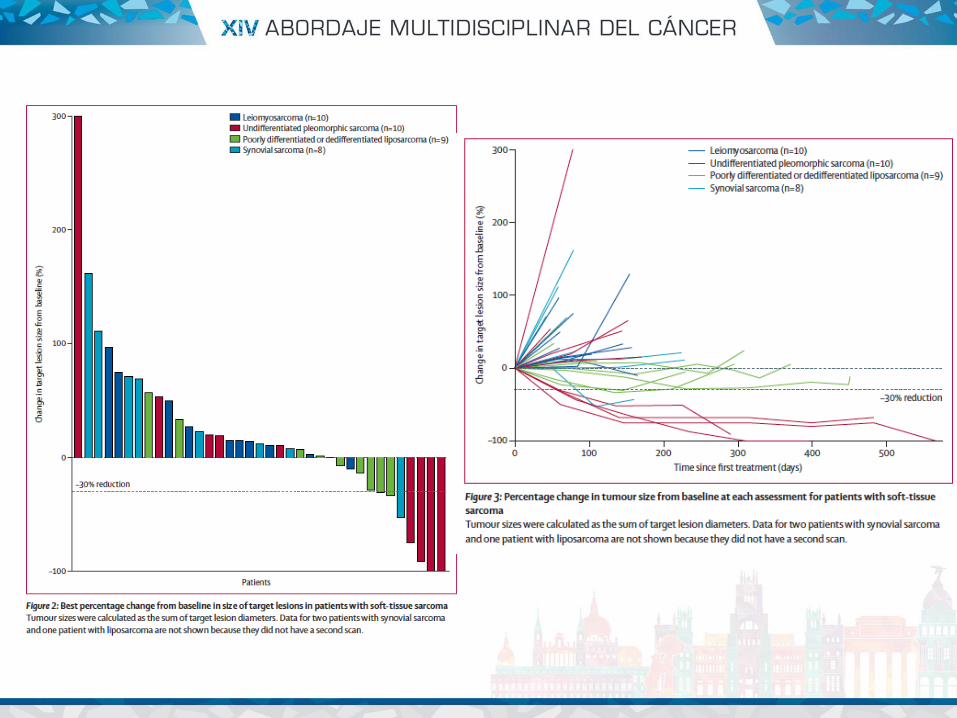

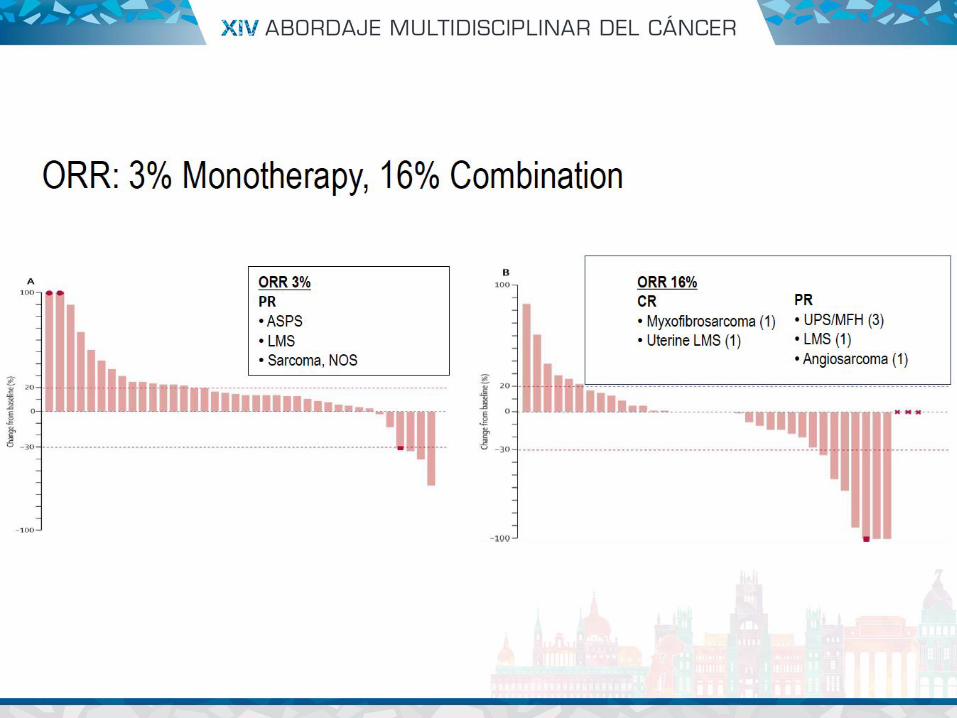
• Hay un papel para bloqueo de PD-1 monoterapia en algunas histologías: UPS (sarcoma pleomorfico indiferenciado) y otros- liposarcoma
• En LMS datos desfavorables en estudios previos (pérdida de PTEN)
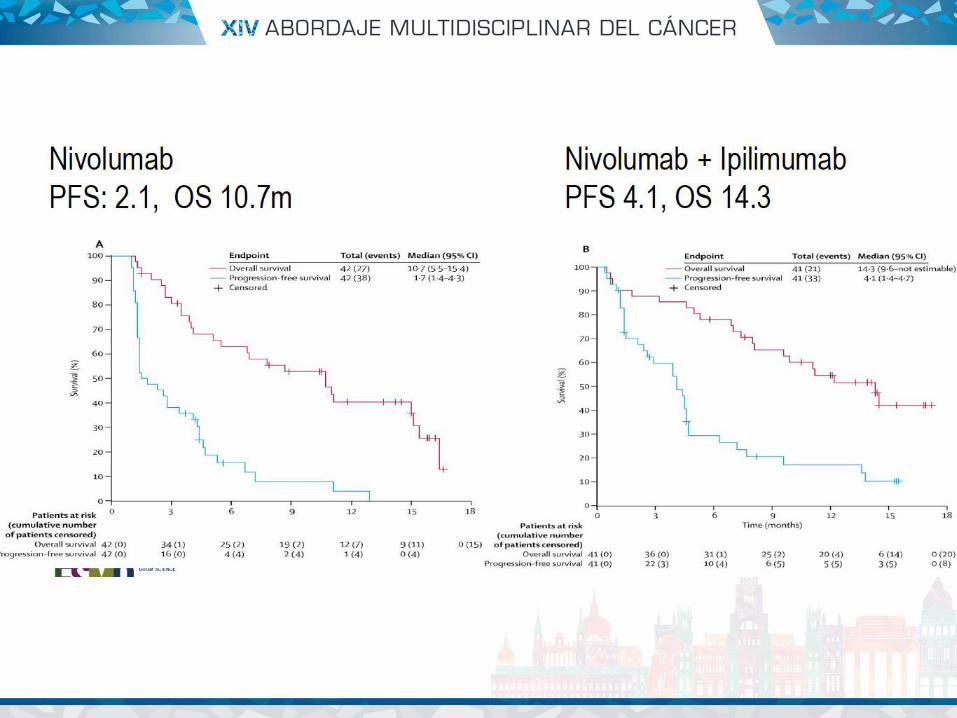
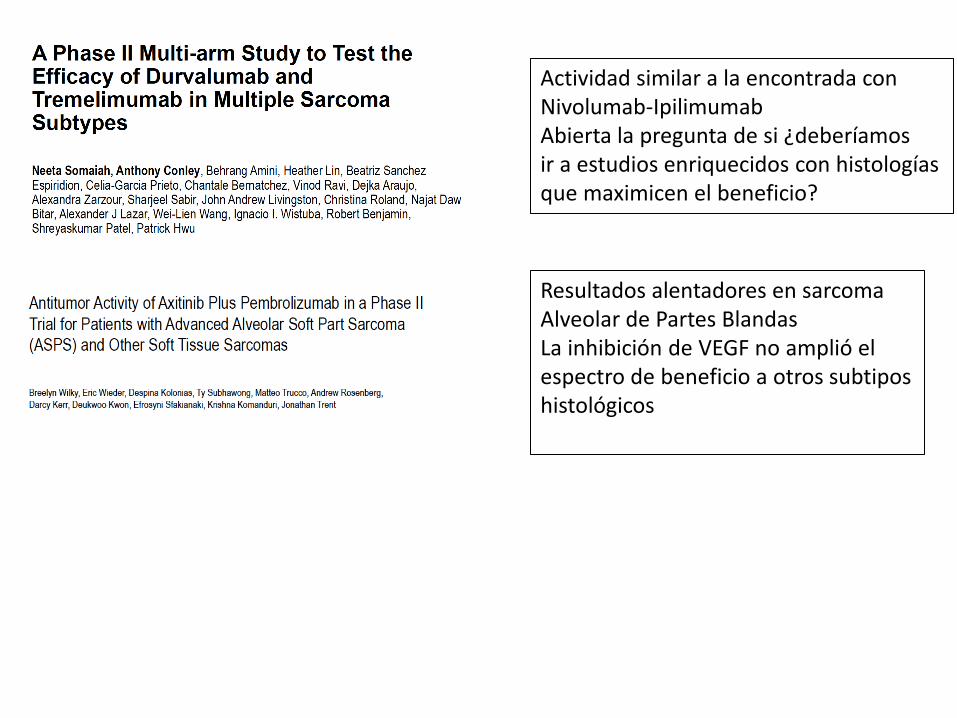
Actividad similar a la encontrada con Nivolumab-Ipilimumab Abierta la pregunta de si ¿deberíamos ir a estudios enriquecidos con histologías que maximicen el beneficio?
Resultados alentadores en sarcoma Alveolar de Partes Blandas La inhibición de VEGF no amplió el espectro de beneficio a otros subtipos histológicos
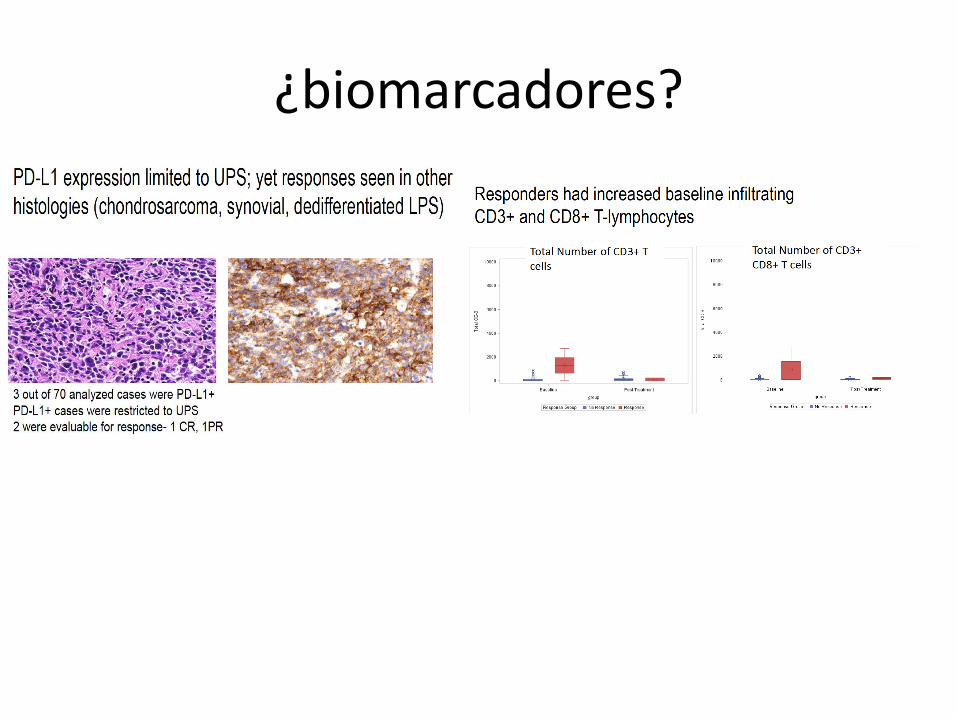
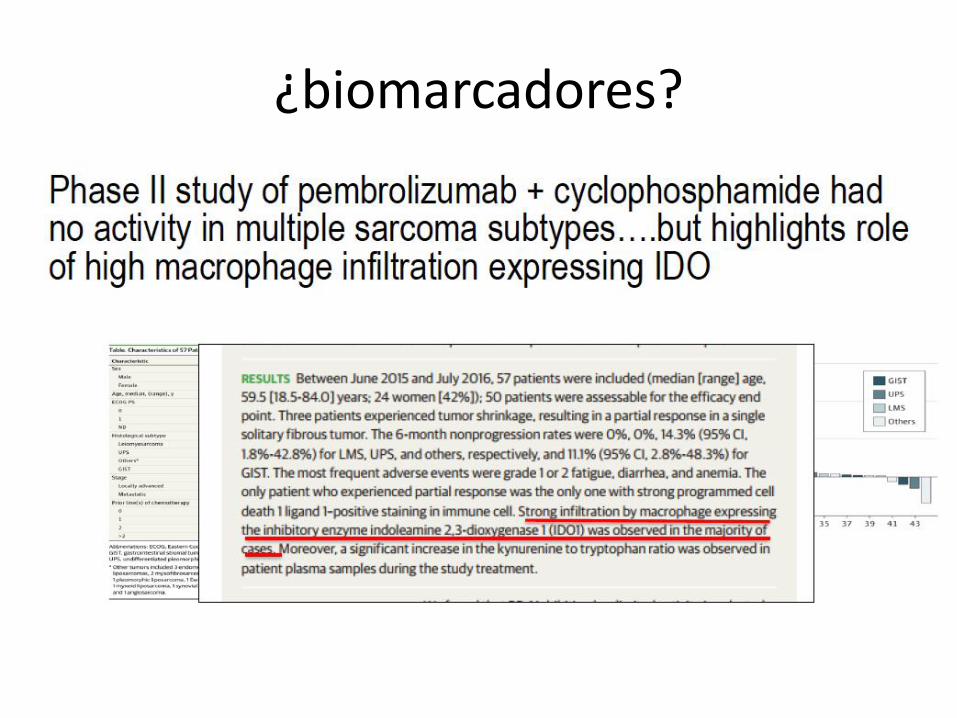
¿biomarcadores?
• Estudios muy heterogéneos • Monoterapia antiPD1: UPS, liposarcoma desdiferenciado • Combinaciones de inmunoterapia: en otros sarcomas • En sarcoma alveolar de partes blandas: combinación inmunoterapia
y anti VEGF? • Para poder avanzar, es necesario buscar una biología tumoral entre
los subtipos histológicos para poder definir estrategias
¿cual es la situación actual en inmunoterapia?
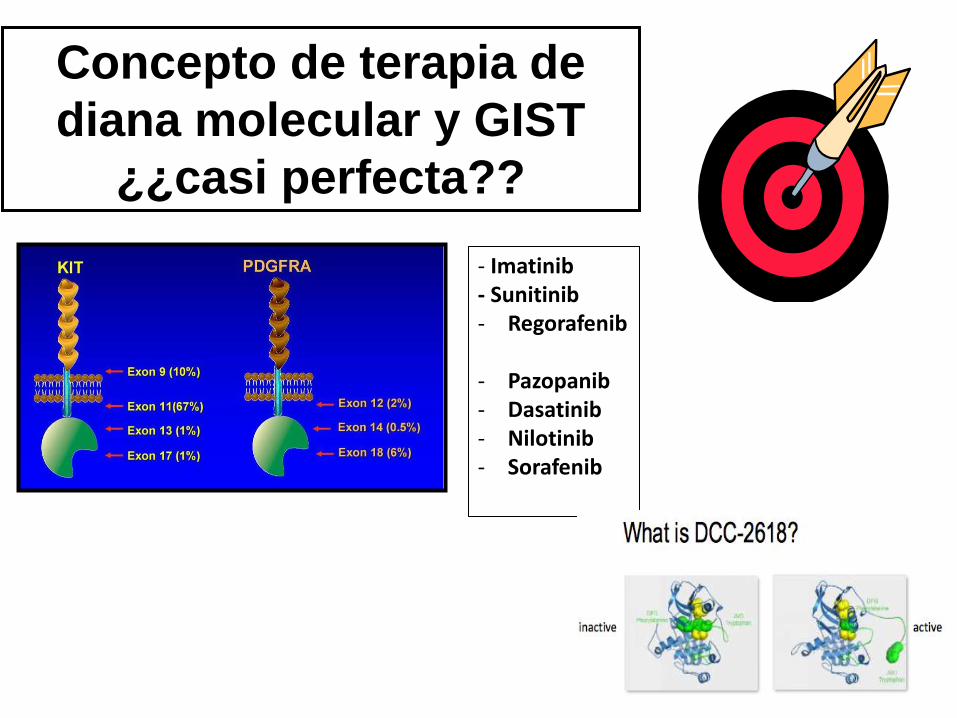
- Imatinib - Sunitinib - Regorafenib
- Pazopanib - Dasatinib - Nilotinib - Sorafenib
Concepto de terapia de
diana molecular y GIST
¿¿casi perfecta??

MUCHAS GRACIAS

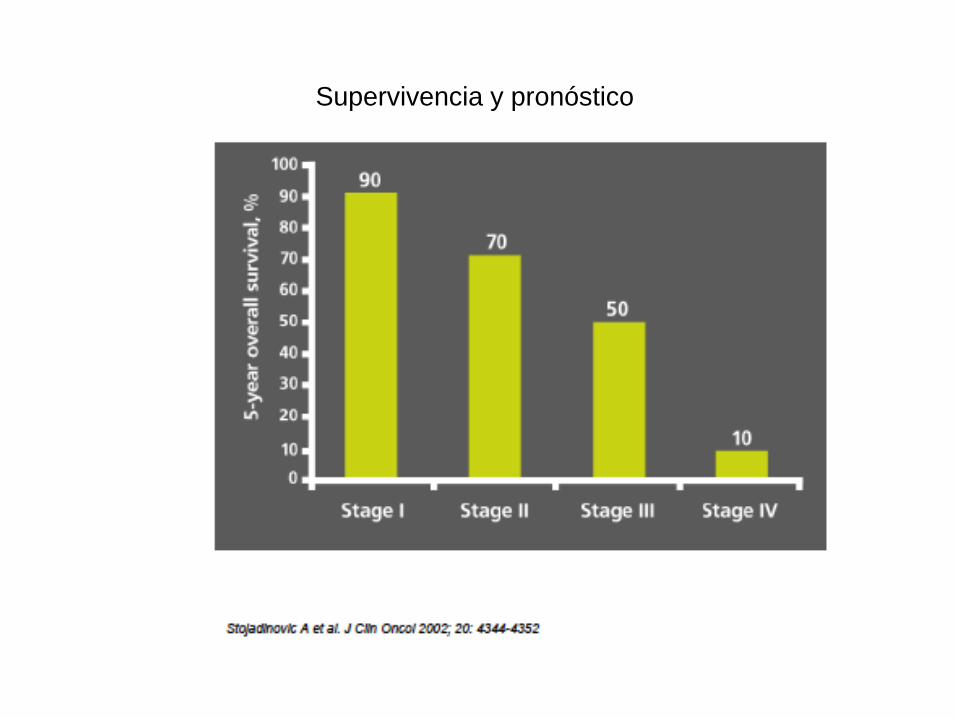
Supervivencia y pronóstico
• Debido a su rareza y heterogeneidad
– Estudios pequeños
– Estudios con representación de diferentes subgrupos (mas Qt sensibles/resistentes)
– Diferentes esquemas y dosis
– Diferentes end point: OS, ORR, CBR
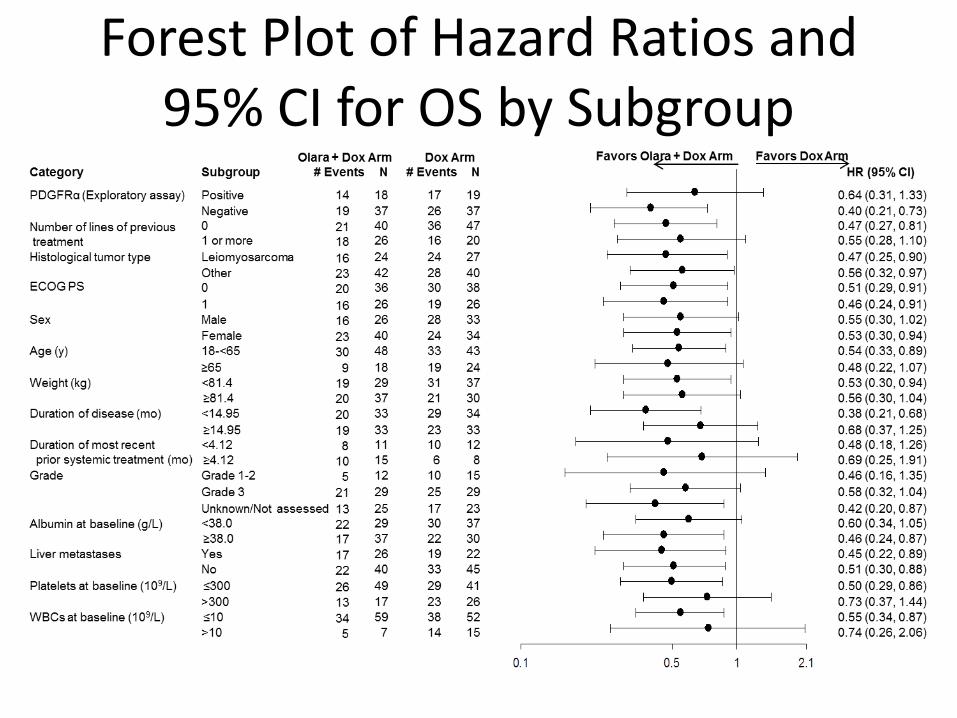
Forest Plot of Hazard Ratios and 95% CI for OS by Subgroup
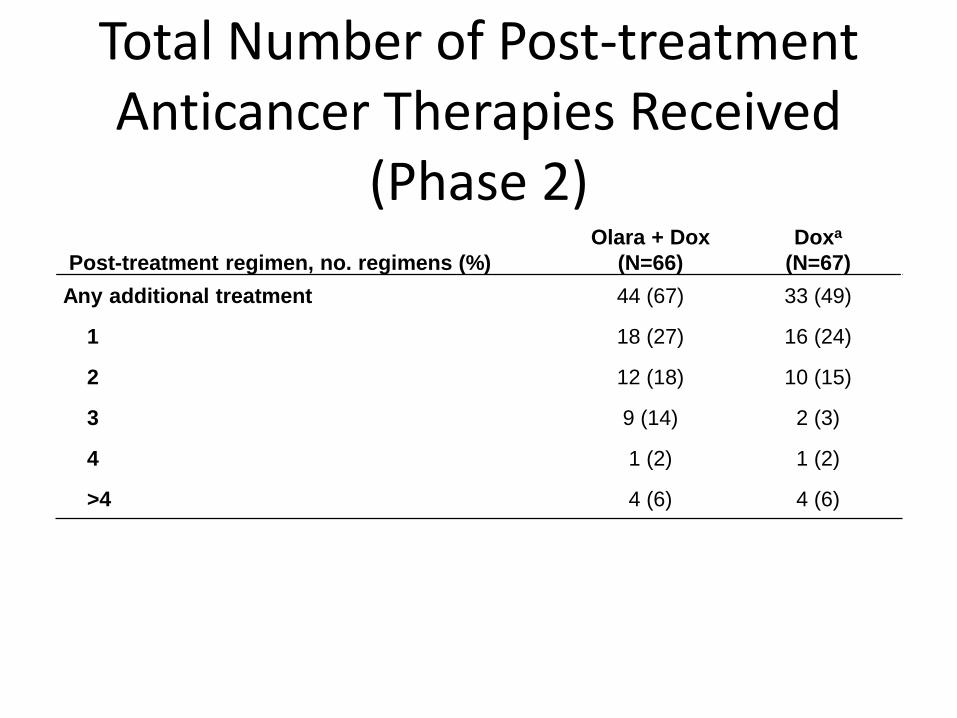
Post-treatment regimen, no. regimens (%)
Olara + Dox
(N=66)
Doxa
(N=67)
Any additional treatment 44 (67) 33 (49)
1 18 (27) 16 (24)
2 12 (18) 10 (15)
3 9 (14) 2 (3)
4 1 (2) 1 (2)
>4 4 (6) 4 (6)
Total Number of Post-treatment Anticancer Therapies Received
(Phase 2)
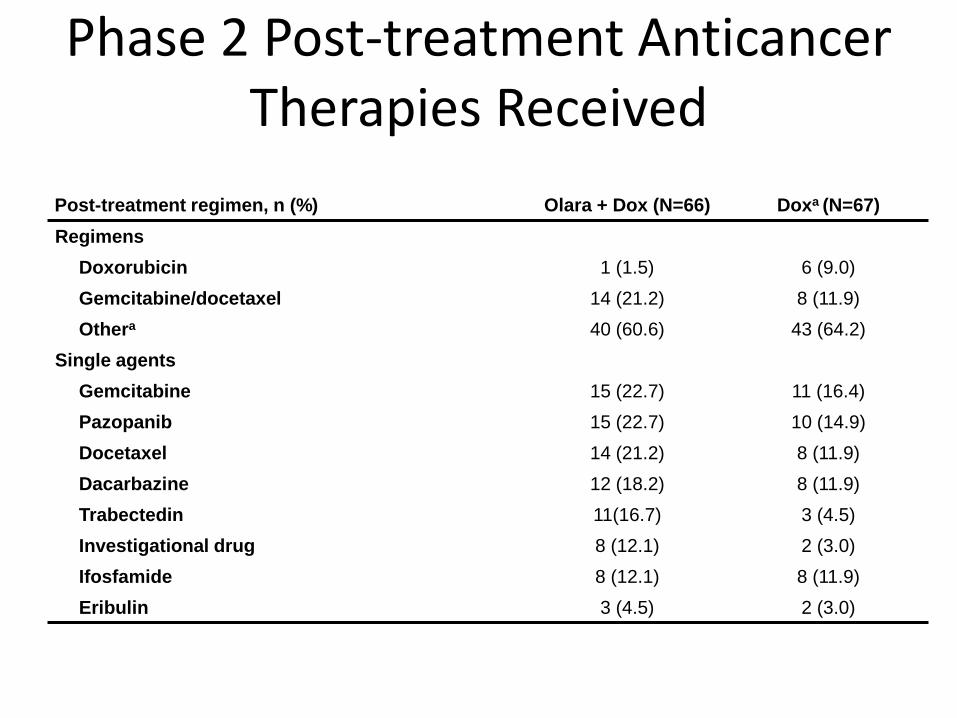
Post-treatment regimen, n (%) Olara + Dox (N=66) Doxa (N=67)
Regimens
Doxorubicin 1 (1.5) 6 (9.0)
Gemcitabine/docetaxel 14 (21.2) 8 (11.9)
Othera 40 (60.6) 43 (64.2)
Single agents
Gemcitabine 15 (22.7) 11 (16.4)
Pazopanib 15 (22.7) 10 (14.9)
Docetaxel 14 (21.2) 8 (11.9)
Dacarbazine 12 (18.2) 8 (11.9)
Trabectedin 11(16.7) 3 (4.5)
Investigational drug 8 (12.1) 2 (3.0)
Ifosfamide 8 (12.1) 8 (11.9)
Eribulin 3 (4.5) 2 (3.0)
Phase 2 Post-treatment Anticancer Therapies Received

♦ Initial analysis of PDGFRα expression showed 88% of tumors in patients treated with olaratumab + doxorubicin and 88% of tumors in patients treated with doxorubicin were PDGFRα positive; however, this assay was subsequently found to have poor specificity for PDGFRα by also detecting PDGFRβ, precluding meaningful data analysis
♦ Reanalysis of study tumor samples with an assay that had better specificity for PDGFRα showed that 33% of tumors in patients treated with olaratumab + doxorubicin and 34% of tumors in patients treated with doxorubicin were positive for PDGFRα, consistent with a 2015 study1
♦ The interaction effect between PDGFRα expression (positive or negative) and treatment was not significant for either OS (p=.3209) or PFS (p=.5924)
Analysis of PDGFR Expression
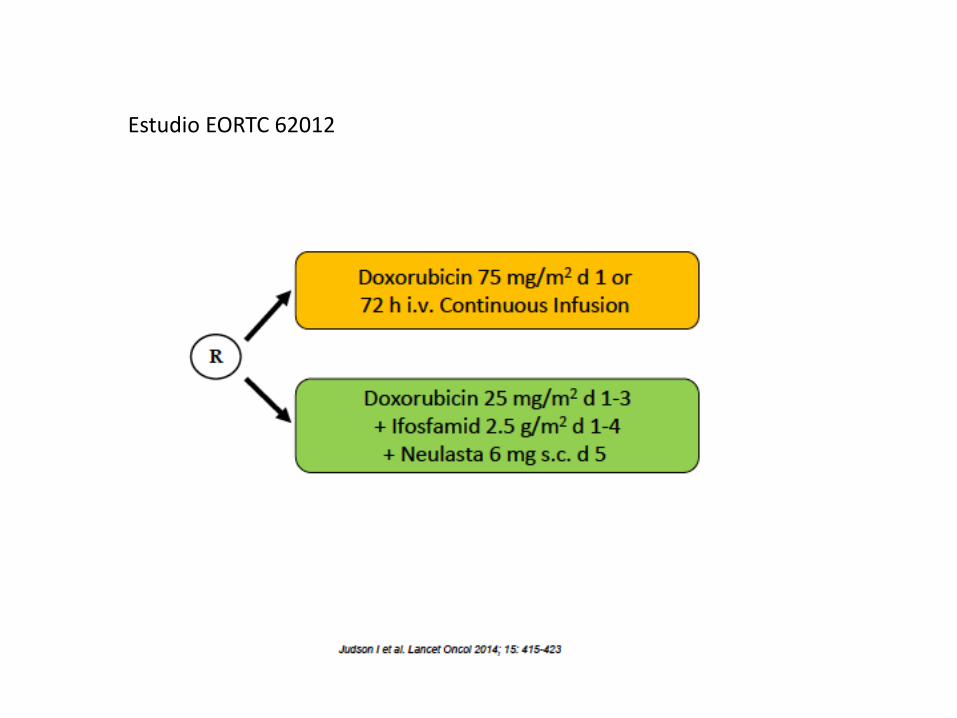
Estudio EORTC 62012
– Sunitinib:
Estudios retrospectivos: PR+EE (3/4 pac)
– Cediranib: fase II.RP 14/28 pac)
– Pazopanib:
– Estudio retropectivo (n=30). Resp+ EE= 25/29pac. PFS 13.6m
Stacchiotti S et al. Oncologist 2018:62-70.

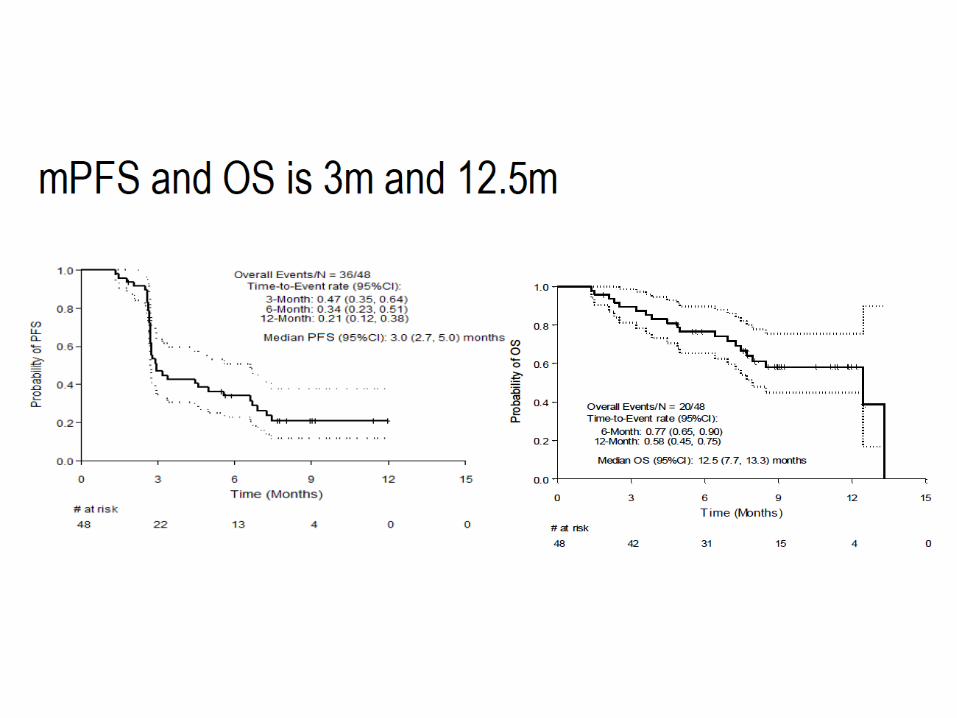
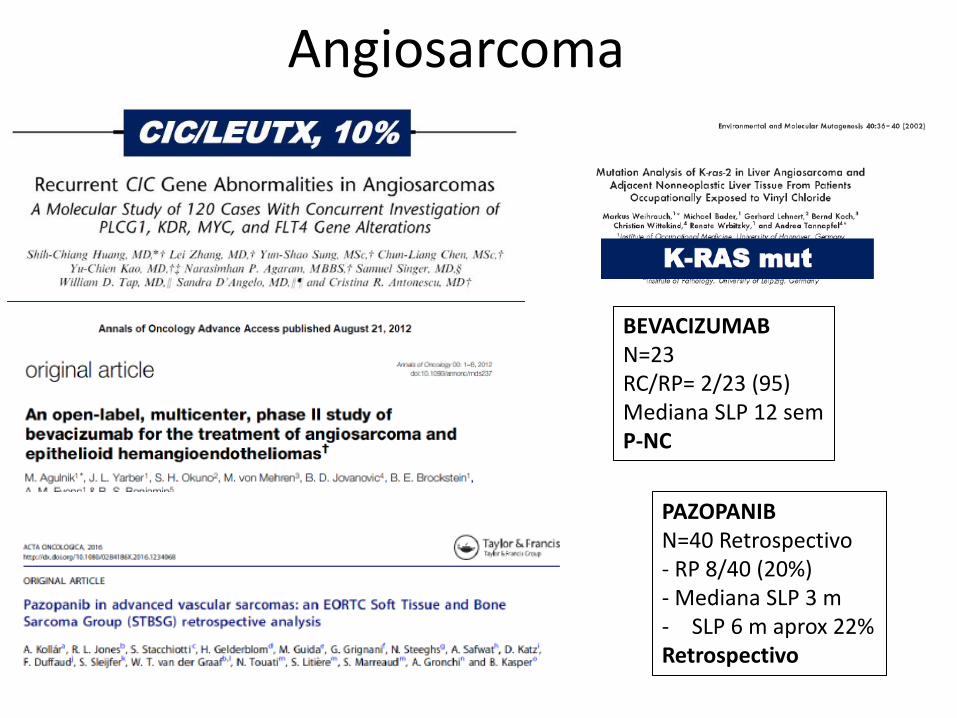
Angiosarcoma
BEVACIZUMAB N=23 RC/RP= 2/23 (95) Mediana SLP 12 sem P-NC
PAZOPANIB N=40 Retrospectivo - RP 8/40 (20%) - Mediana SLP 3 m - SLP 6 m aprox 22% Retrospectivo
¿biomarcadores?

¿biomarcadores?
Top Related