Fortuny - 559 MODIF. SALA 112 SAB 12.00
21
CARDIOACTUALIDAD: LO MÁS RELEVANTE DE LA CARDIOLOGÍA EUROPEA Y MUNDIAL EN EL ÚLTIMO AÑO CARDIOPATÍA ISQUEMICA Dra. Magda Heras ICT, Hospital Clínic, Barcelona Congreso Nacional Enfermedades CV Barcelona, Octubre 2009
-
Upload
sociedad-espanola-de-cardiologia -
Category
Documents
-
view
216 -
download
1
description
Dra. Magda Heras Congreso Nacional Enfermedades CV Barcelona, Octubre 2009 CARDIOACTUALIDAD: LO MÁS RELEVANTE DE LA CARDIOLOGÍA EUROPEA Y MUNDIAL EN EL ÚLTIMO AÑO ICT, Hospital Clínic, Barcelona • GSK (beca no condicionada) • Menarini (Consultoría) • AstraZeneca (Coordinación estudio) Conflictos de interés: • SÍNDROME CORONARIO AGUDO • PREVENCIÓN SECUNDARIA
Transcript of Fortuny - 559 MODIF. SALA 112 SAB 12.00

CARDIOACTUALIDAD: LO MÁS RELEVANTEDE LA CARDIOLOGÍA EUROPEA Y MUNDIAL
EN EL ÚLTIMO AÑO
CARDIOPATÍA ISQUEMICA
Dra. Magda HerasICT, Hospital Clínic, Barcelona
Congreso Nacional Enfermedades CVBarcelona, Octubre 2009

Conflictos de interés:
• GSK (beca no condicionada)• Menarini (Consultoría)• AstraZeneca (Coordinación estudio)
• SÍNDROME CORONARIO AGUDO
• PREVENCIÓN SECUNDARIA
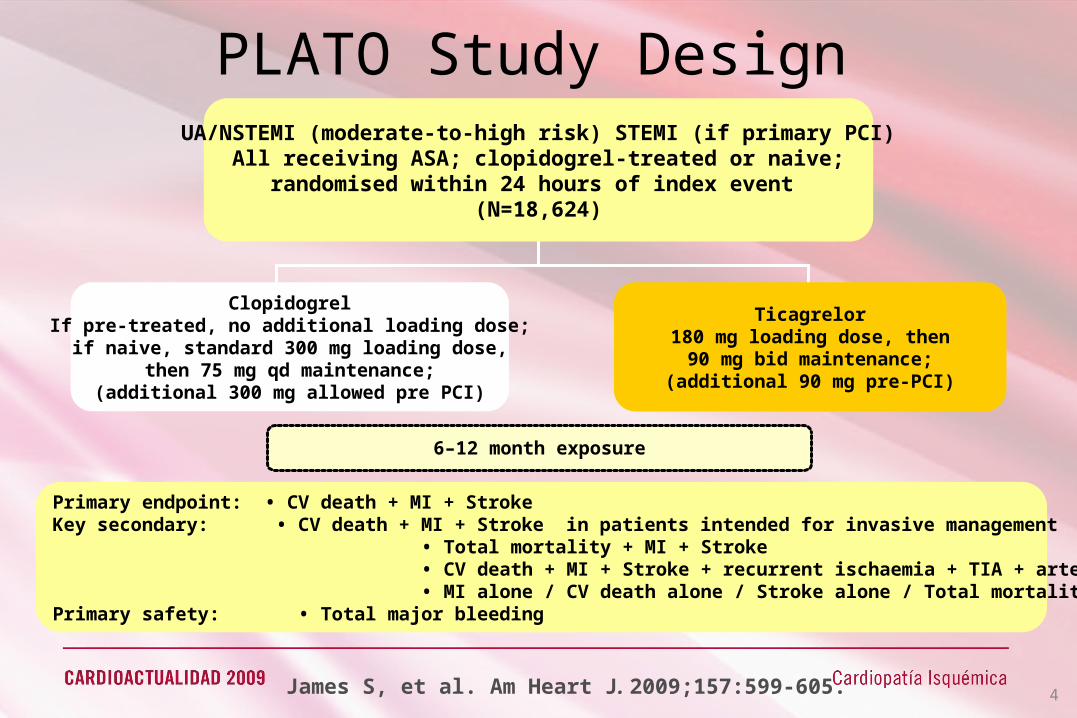
PLATO Study Design
Primary endpoint: • CV death + MI + Stroke Key secondary: • CV death + MI + Stroke in patients intended for invasive management • Total mortality + MI + Stroke • CV death + MI + Stroke + recurrent ischaemia + TIA + arterial thrombotic events • MI alone / CV death alone / Stroke alone / Total mortalityPrimary safety: • Total major bleeding
6–12 month exposure
ClopidogrelIf pre-treated, no additional loading dose;if naive, standard 300 mg loading dose,
then 75 mg qd maintenance;(additional 300 mg allowed pre PCI)
Ticagrelor180 mg loading dose, then
90 mg bid maintenance;(additional 90 mg pre-PCI)
UA/NSTEMI (moderate-to-high risk) STEMI (if primary PCI)All receiving ASA; clopidogrel-treated or naive;
randomised within 24 hours of index event (N=18,624)
James S, et al. Am Heart J. 2009;157:599-605. 4

TICAGRELOR IN ACS. THE PLATO STUDY
All Patients*All Patients*Ticagrelor Ticagrelor (n=9,333)(n=9,333)
Clopidogrel Clopidogrel (n=9,291)(n=9,291)
HR for ticagrelor HR for ticagrelor (95% CI)(95% CI) PP value value✝✝
Primary Objective, n (%/yr)
CV death + MI + stroke 864 (9.8) 1,014 (11.7) 0.84 (0.77-0.92) 0.0003Secondary Objectives, n Secondary Objectives, n (%/yr)(%/yr)
Total death + MI + stroke 901 (10.2) 1,065 (12.3) 0.84 (0.77-0.92) 0.0001
CV death + MI + stroke + severe + recurrent ischemia
+ TIA + arterial thrombus1,290 (14.6) 1,456 (16.7) 0.88 (0.81-0.95) 0.0006
MI 504 (5.8) 593 (6.9) 0.84 (0.75-0.95) 0.0045CV death 353 (4.0) 442 (5.1) 0.79 (0.69-0.91) 0.0013
Stroke 125 (1.5) 106 (1.3) 1.17 (0.91-1.52) 0.2249
Total Death 399 (4.5) 506 (5.9) 0.78 (0.69-0.89) 0.0003
Hierarchical Testing of Major Efficacy EndpointsHierarchical Testing of Major Efficacy Endpoints
Wallentin L, et al. New Engl J Med. 2009;361.

No. at risk
ClopidogrelTicagrelor
9,2919,333
8,5218,628
8,3628,460
8,124
Days after randomisation
6,7436,743
5,0965,161
4,0474,147
0 60 120 180 240 300 360
121110
9876543210
13
Cum
ulat
ive
inci
denc
e (%
)9.8
11.7
8,219
Clopidogrel
Ticagrelor
K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval
Wallentin L, et al. New Engl J Med. 2009;361.6
TICAGRELOR IN ACS. THE PLATO STUDY
Death, MI or Stroke
p=0.0003HR 0.84 (95% CI 0.77–0.92)
RRR = 16%, ARR = 1.87%, NNT = 54
Mehta S, et al ESC 2009, Hot Line

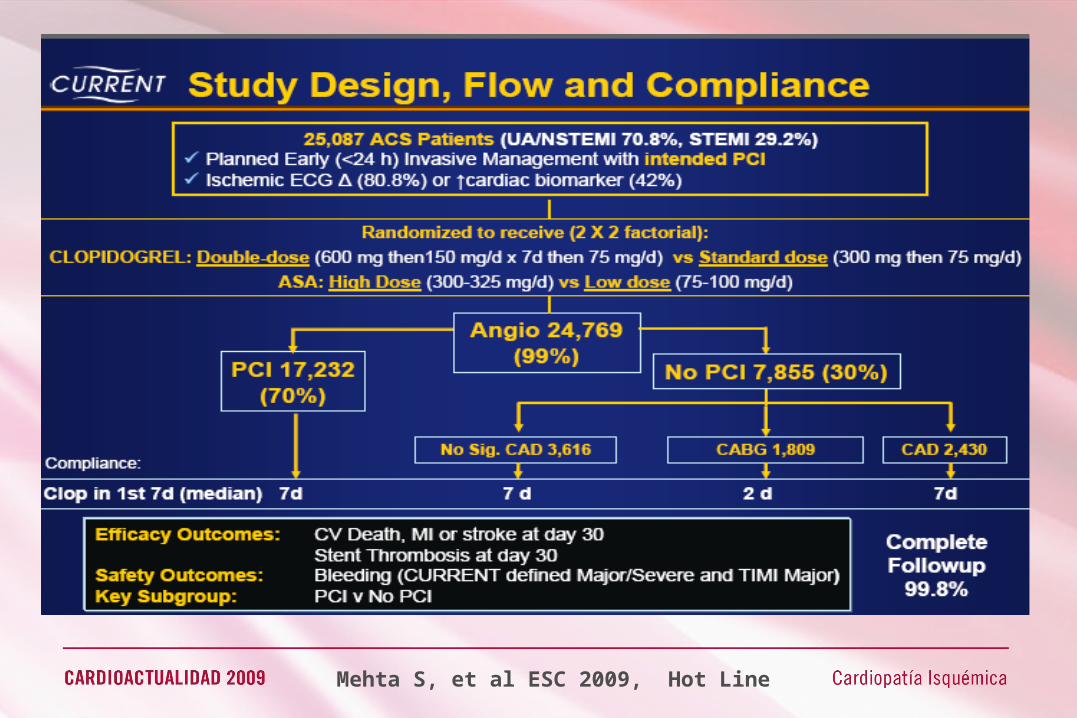
CLOPIDOGREL IN ACS. THE CURRENT STUDY
Mehta S, et al ESC 2009, Hot Line

PRASUGREL IN STEMI. THE TRITON – TIMI 38 STUDY
Montalescot G et al. Lancet 2009; 373: 723–31

PRASUGREL IN STEMI. THE TRITON – TIMI 38 STUDY
Montalescot G et al. Lancet 2009; 373: 723–31
Death, MI, stroke Death, MI, urgent TVR
Stent thrombosis TIMI major bleeding, non-CABG related

0
2
4
6
8
10
12
14
Death,MI,RIUR,BO Death, MI Major bleeding
Early eptifibatide Early placebo
% p
ts
96 h 30 d 120 h
P=0.02
P=0.08
GP IIb/IIIa antagonists in NSTEMIThe EARLY-ACS study
Giugliano et al. NEJM 2009; 360: 2176-90Giugliano et al. NEJM 2009; 360: 2176-90
• Routine early eptifibatide vs provisional use after angiography (decision by MD)• High risk: troponins, ST changes, >60 y. Randomization < 24h. Angio 8-12h• UFH 35%, LMWH 53%, both 7%, other 6%. Clopidogrel before angio 75%• 59% PCI, 13% CABG, 28% medical therapy. 37% provisional arm eptifibatide

OTAMIXABAN IN NSTEMI. THE SEPIA-ACS 1 STUDY
Sabatine M. ESC 2009 [ figura REC 2009;62:1149-60]
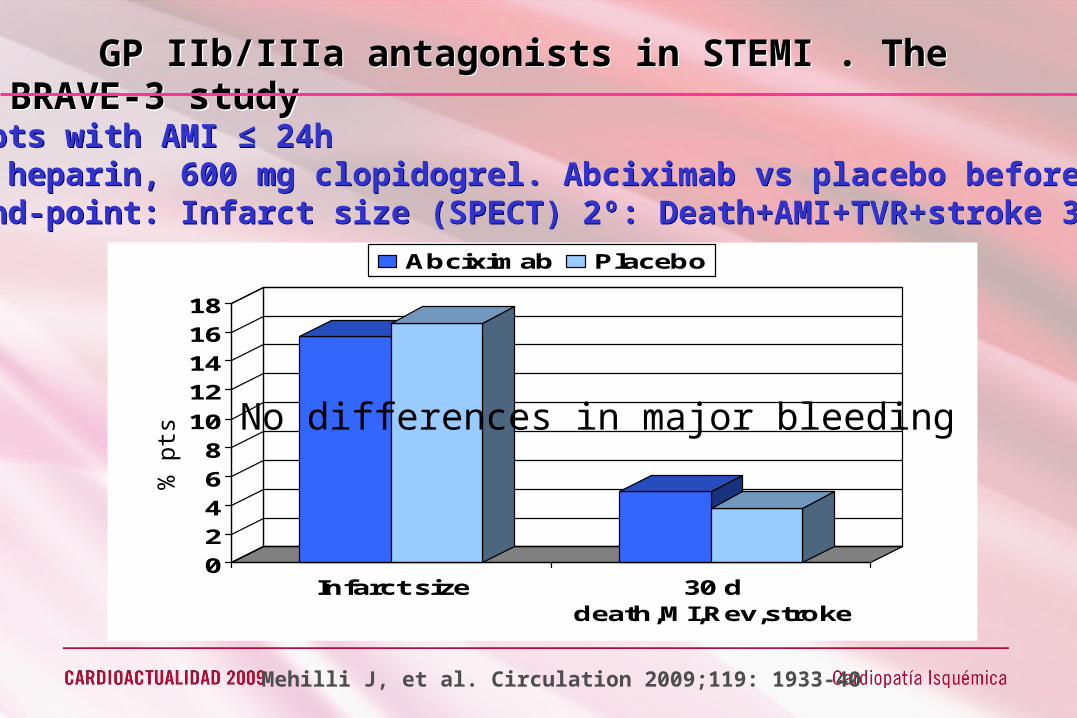
GP IIb/IIIa antagonists in STEMI . The BRAVE-3 study
800 pts with AMI ≤ 24hASA, heparin, 600 mg clopidogrel. Abciximab vs placebo before pPCI1º end-point: Infarct size (SPECT) 2º: Death+AMI+TVR+stroke 30 d.
02468
1012141618
Infarct size 30 ddeath,MI,Rev,stroke
Abciximab Placebo
% p
ts No differences in major bleeding
Mehilli J, et al. Circulation 2009;119: 1933-40

ROUTINE PCI AFTER FIBRINOLYSIS IN STEMI The TRANSFER study
1059 pts with high risk AMI ≤ 12h, in non-PCI centresASA, TNK, heparin, clopidogrel (recom). Randomized early routine PCI ≤ 6h (99%) vs standard treatment (1/3 required urgent PCI)1º end-point: Death+AMI+ Rec isch+ CHF, shock 30 d.
Cantor WJ, et al. NEJM 2009;360: 2705-18
02468
1012141618
Prim end-point Rec isch CHF
Standard Tt Early PCI
P=0.004
P=0.003P=0.04
RR 0.64 0.09 0.54
% p
ts

PRIMARY PCI VS FIBRINOLYSIS IN STEMI IN THE ELDERLY. The TRIANA study
266 pts with AMI > 75 yrs, admitted to active pPCI (23 centres) Randomized to pPCI vs TNK ASA, heparin, clopidogrel (recom). 1º end-point: Death+AMI+ stroke 30 d.
Bueno H, et al ESC 2009, Hot Line
0
5
10
15
20
25
30
Death,AMI,CVA Death AMI CVA
pPCI Fibrinolysis
OR 1.31 (0.67-2.56) P = 0.43
OR 1.60 (0.60-4.25) P = 0.35
OR 4.03 (0.44-36.5)P = 0.18
OR 1.46 (0.81-2.61) P = 0.21

• SÍNDROME CORONARIO AGUDO
• PREVENCIÓN SECUNDARIA
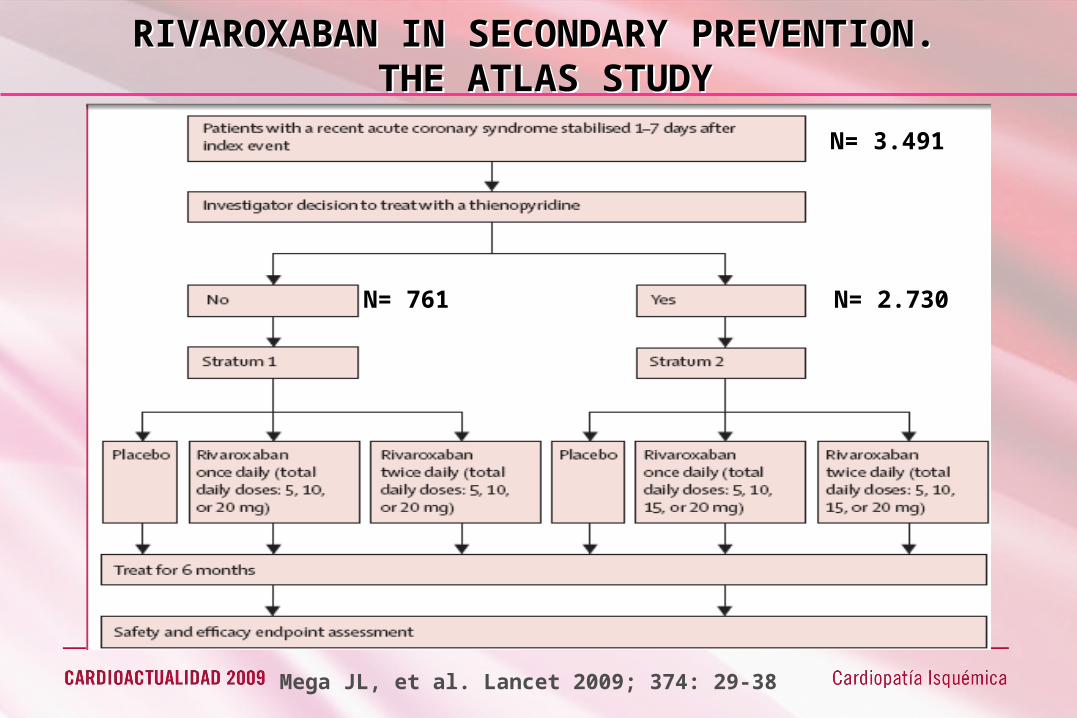
N= 3.491
N= 2.730N= 761
Mega JL, et al. Lancet 2009; 374: 29-38
RIVAROXABAN IN SECONDARY PREVENTION. THE ATLAS STUDY

RIVAROXABAN IN SECONDARY PREVENTION. THE ATLAS STUDY
Mega JL, et al. Lancet 2009; 374: 29-38
BLEEDING
2 EFFICACY
5,5
3,9
1 EFFICACY
5,6
7,0

Apixaban 2,5 HR 1,78, NSApixaban 10 HR 2,45, p=0,005
BLEEDINGISTH MAJOR, CR NON-MAJOR
Apixaban 2,5 HR 0,73, NSApixaban 10 HR 0,61, p=0,07
EFFICACYDEATH, MI, REC ISCH, STROKE
APIXABAN IN SECONDARY PREVENTION. THE APPRAISE STUDY
Appraise Investigators. Circulation 2009; 119: 2877- 85
CR: Clinically relevant

THROMBIN RECEPTOR ANTAGONIST SCH 530348THE TRA-PCI STUDY
Becker RC, et al Lancet 2009; 373: 919-28

CONCLUSIONES
SCA• Nuevos fármacos antiagregantes, prasugrel y ticagrelor • El traslado para ICP tras fibrinolíticos reduce los eventos• Estudio TRIANA: la ICPp es > fibrinolisis en pacientes >75 a;
no provoca exceso de hemorragias
PREVENCIÓN SECUNDARIA• Nuevos tratamientos antiplaquetarios (inhibidor receptor trombina) y anticoagulantes orales (inhibidores FXa)