
Rol de la antiangiogénesis en cáncer de pulmón · •Descarta intervención y desestiman...
63
Rol de la antiangiogénesis en cáncer de pulmón Dr. Javier de Castro
Transcript of Rol de la antiangiogénesis en cáncer de pulmón · •Descarta intervención y desestiman...

Rol de la antiangiogénesis en cáncer de pulmón
Dr. Javier de Castro

• Mujer de 53 años
• Fumadora 15 cig/día x 30 años
• Cefalea opresiva, nauseas y vómitos de 7 días de evolución
• Lesiones ocupantes de espacio con realce periférico y centro quístico/necrótico supra e infratentoriales. Signos de hidrocefalia supratentorial con edema transependimario. Signos de herniación transtentorial ascendente y posiblemente amigdalar. Incipiente herniación falcial.
Caso Clínico

Nódulo en LSD de 18 mm, con afectacion ganglionar parahiliar dcha, ventana aortopulmonar (46 mm) e infracarinal (33 mm)y supraclavicualr ipsilateral.
EBUS: PAAF de adenopatías en región 4R y 7 con metástasis de adenocaricnoma
TAC
Adenocarcinoma de pulmón TTF1neg EGFR wt, AlK no traslocado

• Descarta intervención y desestiman craneotomia descompresiva
• Se desestima RT por riesgo de herniación
Neurocirugia
Oncología Radioterápica
Oncología Médica ?

1. Doblete de platino
2. Platino-pemetrexed
3. Doblete de platino + bevacizumab
4. Platino-pemetrexed+bevacizumab
En el caso presentado, ¿cuál sería su primera
opción de tratamiento?

Secretion of Angiogenic Factors New Capillary Sprouting
Sprout Fusion and Lumen Formation

Tumor Hypoxia and Angiogenesis • Hypoxia: low local oxygen concentration
• Tumor hypoxia is the primary stimulus for VEGF production1,2
• Excessive VEGF initiates the tumor angiogenic process2
1. Reviewed in Chung et al. Nat Rev Cancer 2010;10(7):505-14. 2. Reviewed in Papetti and Herman. Am J Physiol Cell Physiol 2002;282(5):C947-70.

The VEGF Family of Ligands and Receptors in Tumor Angiogenesis and Lymphangiogenesis
1. Reviewed in Adams and Alitalo. Nat Rev Mol Cell Biol 2007;8(6):464-78. 2. Reviewed in Hicklin and Ellis. J Clin Oncol 2005;23(5):1011-27.
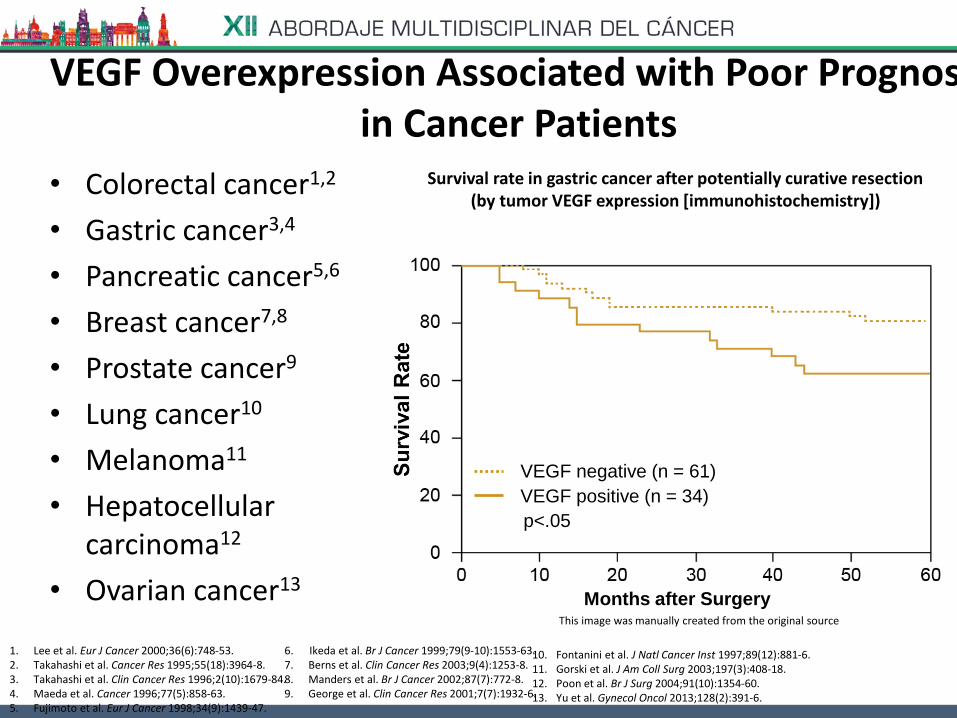
VEGF Overexpression Associated with Poor Prognosis in Cancer Patients
• Colorectal cancer1,2
• Gastric cancer3,4
• Pancreatic cancer5,6
• Breast cancer7,8
• Prostate cancer9
• Lung cancer10
• Melanoma11
• Hepatocellular carcinoma12
• Ovarian cancer13
1. Lee et al. Eur J Cancer 2000;36(6):748-53. 2. Takahashi et al. Cancer Res 1995;55(18):3964-8. 3. Takahashi et al. Clin Cancer Res 1996;2(10):1679-84. 4. Maeda et al. Cancer 1996;77(5):858-63. 5. Fujimoto et al. Eur J Cancer 1998;34(9):1439-47.
6. Ikeda et al. Br J Cancer 1999;79(9-10):1553-63. 7. Berns et al. Clin Cancer Res 2003;9(4):1253-8. 8. Manders et al. Br J Cancer 2002;87(7):772-8. 9. George et al. Clin Cancer Res 2001;7(7):1932-6.
Survival rate in gastric cancer after potentially curative resection (by tumor VEGF expression [immunohistochemistry])
10. Fontanini et al. J Natl Cancer Inst 1997;89(12):881-6. 11. Gorski et al. J Am Coll Surg 2003;197(3):408-18. 12. Poon et al. Br J Surg 2004;91(10):1354-60. 13. Yu et al. Gynecol Oncol 2013;128(2):391-6.
This image was manually created from the original source
Months after Surgery
VEGF negative (n = 61)
VEGF positive (n = 34)
p<.05

VEGF expression associated with significantly lower
survival in lung adenocarcinoma* patients
Pati
en
ts a
live (
%)
Time (months)
0 12 24 36 48 60 72 84
VEGF-A-negative tumours‡ (n=39)
VEGF-A-positive tumours‡ (n=46)
Nakashima, et al. Med Sci Monit 2004
*Early stage disease ‡Intratumoral VEGF-A expression measured by IHC
100
80
60
40
20
0
p=0.0002

Inducing
angiogenesis
Cancer
Sustaining proliferative
signaling
Evading growth
suppressors
Activating invasion
and metastasis
Enabling replicative
mortality
Resisting cell
death
Hanahan & Weinberg. Cell 2011

Mechanisms of targeting angiogenesis
Wheatley-Price and Shepherd, J Thorac Oncol 2008;3:1173

Strategies for Blocking the VEGF Receptor Pathways
Antibody to VEGFR-2 • Blocks ligand binding
• Blocks receptor activation and signaling
Ramucirumab
Tyrosine kinase inhibitor to VEGFR-2 • Blocks receptor kinase
activity and signaling Sorafenib Sunitinib Pazopanib Vandetanib Axitinib
Inhibition of VEGF ligand • Blocks VEGF binding
• Inhibits signaling due to VEGF(s)
Bevacizumab Aflibercept Ziv-aflibercept Neovastat
Reviewed in Tugues et al. Mol Aspects Med 2011;32(2):88-111.
Cediranib Brivanib alaninate Motesanib Linifanib Tivozanib

1. Por cuestiones de seguridad
2. Por considerar que no aporta un beneficio significativo
3. Por su elevado coste
4. Por ausencia de un biomarcador que seleccione al paciente adecuado
¿Por qué no ha considerado la opción de un tratamiento antiangiogénico?

*The analysis corrected for the patients in AVAiL (7%) who received
antineoplastic therapy before documented disease progression
Significant and consistent PFS benefit in
two phase III trials 1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
Time (months)
0 6 12 18 24 30
PF
S e
sti
ma
te Bev 15mg/kg + CP
CP
E45991
HR=0.66; p<0.001
Bevacizumab 15mg/kg
AVAiL2
Time (months)
0 6 12 18 24 30
Placebo + CG
Bev 7.5mg/kg + CG
Bev 15mg/kg + CG
HR=0.75; p=0.003
Bevacizumab 7.5mg/kg
HR=0.82; p=0.03
Bevacizumab 15mg/kg
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
1. Sandler, et al. NEJM 2006; 2. Reck, et al. JCO 2009
3. Sandler, et al. ECCO 2007
HR=0.68; p<0.0001 HR=0.74; p=0.0021 Pre-planned analysis* applying the
censoring rules from E4599 to AVAIL3

E4599: 14-month OS in patients with
adenocarcinoma histology
Sandler, et al. J Thorac Oncol 2010
1.0
0.8
0.6
0.4
0.2
0
Time (months)
0 6 12 18 24 30 36 42
10.3 14.2
Histology n
Median OS
(months) HR
Non-squamous 878 12.3 0.79
Adenocarcinoma 602 14.2 0.69
HR=0.69 (0.58–0.83)
Pac + Carbo + Bev → Bev
Pac + Carbo
E4599 adenocarcinoma population
OS
est
imat
e
Bev = bevacizumab; Carbo = carboplatin; Pac = paclitaxel

Respuesta tras 4 ciclos de tratamiento

Respuesta tras 4 ciclos de tratamiento
RP sistémica y cerebral. Se completan 6 ciclos y se inicia mantenimiento con bevacizumab

POINTBREAK:
OS (primary endpoint) – ITT population
12.6 13.4
OS
est
imat
e
Time (months)
0 3 6 9 12 15 18 21 24 27 30 33 3639
Patel, et al. J Clin Oncol 2013
1.0
0.8
0.6
0.4
0.2
0
Pem + Carbo
+ Bev
Pem + Bev
(n=472)
Pac + Carbo
+ Bev
Bev
(n=467)
HR
(95% CI)
1.00
(0.86–1.16)
p value 0.949
Median OS
(months) 12.6 13.4

AVAPERL: OS from randomisation*
Bev+pem NR (34 events)
Bev 15.7 months (42 events)
HR=0.75 (0.47–1.20); p=0.23
128 127 120 103 56 20 3 0
125 123 110 96 45 17 2 0
Patients at risk
Bev+pem
Bev
Time (months)
OS
es
tim
ate
0 3 6 9 12 15 18 21
1.0
0.8
0.6
0.4
0.2
0
Cont. maintenance bev+pem (n=128)
Cont. maintenance bev (n=125)
*Randomised patients, Intent-to-treat population
Median follow-up time: 11 months (8 months, excluding induction)
30% of events at the time of analysis for overall survival Barlesi, et al. JCO 2013

Tras un año y medio de tratamiento presenta progresión pulmonar y renal

1. Docetaxel o Pemetrexed
2. Nivolumab
3. Ensayo clínico
4. Docetaxel + antiangiogénico
Ante la progresión de la enfermedad, ¿cuál sería la
opción de tratamiento de segunda línea?

CÁNCER DE PULMÓN DE CÉLULAS NO PEQUEÑAS (CPCNP)
ESTADIO IV
NO ESCAMOSO
TTO 2ª L
ESCAMOSO
TTO 2ª L
PEMETREXED DOCETAXEL DOCETAXEL ERLOTINIB
DOCETAXEL+ NINTEDANIB DOCETAXEL + RAMUCIRUMAB
NIVOLUMAB NIVOLUMAB

Ramucirumab (IMC-1121B)
• Ramucirumab is a fully human IgG1 monoclonal antibody that binds with high affinity to human VEGFR-2 (Kd ~ 50 pM)1
• Ramucirumab is specific for the human VEGFR-2 receptor2
• Ramucirumab potently blocks binding of VEGF-A to VEGFR-2 (IC50 = 0.8 nM)1
• Ramucirumab blocks binding of VEGF-C and VEGF-D to VEGFR-23
1. Lu et al. J Biol Chem 2003;278(44):43496-507.
2. Data on file, ImClone Systems, a wholly-owned subsidiary of Eli Lilly and Company.
3. Data on file, ImClone Systems, a wholly-owned subsidiary of Eli Lilly and Company.
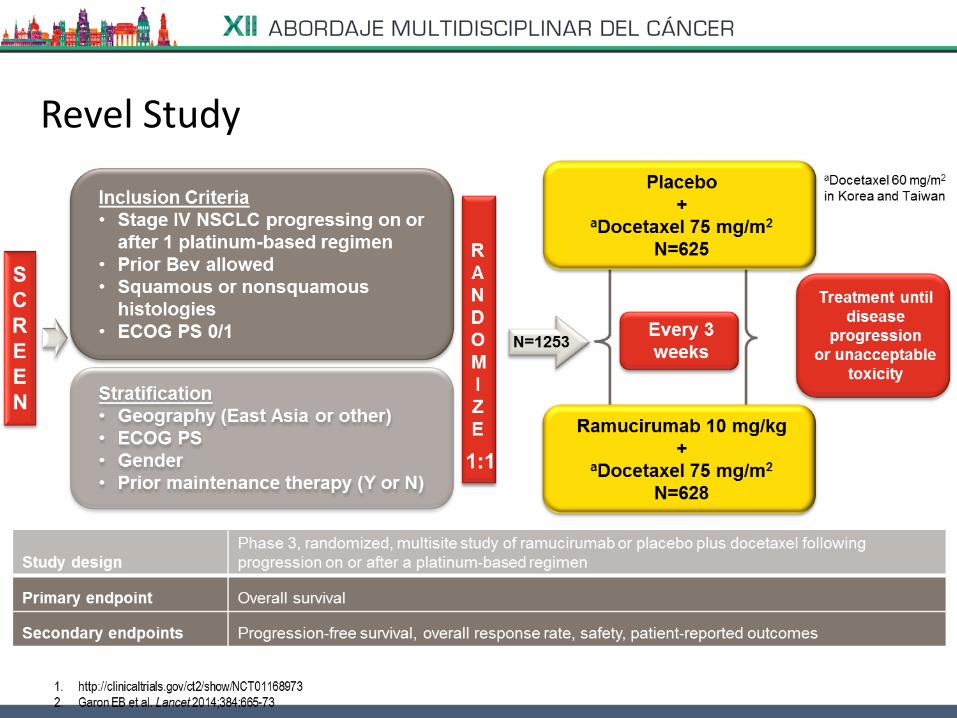
Revel Study

OVERALL SURVIVAL (ITT)

OVERALL SURVIVAL (SUBGROUP ANALYSIS)
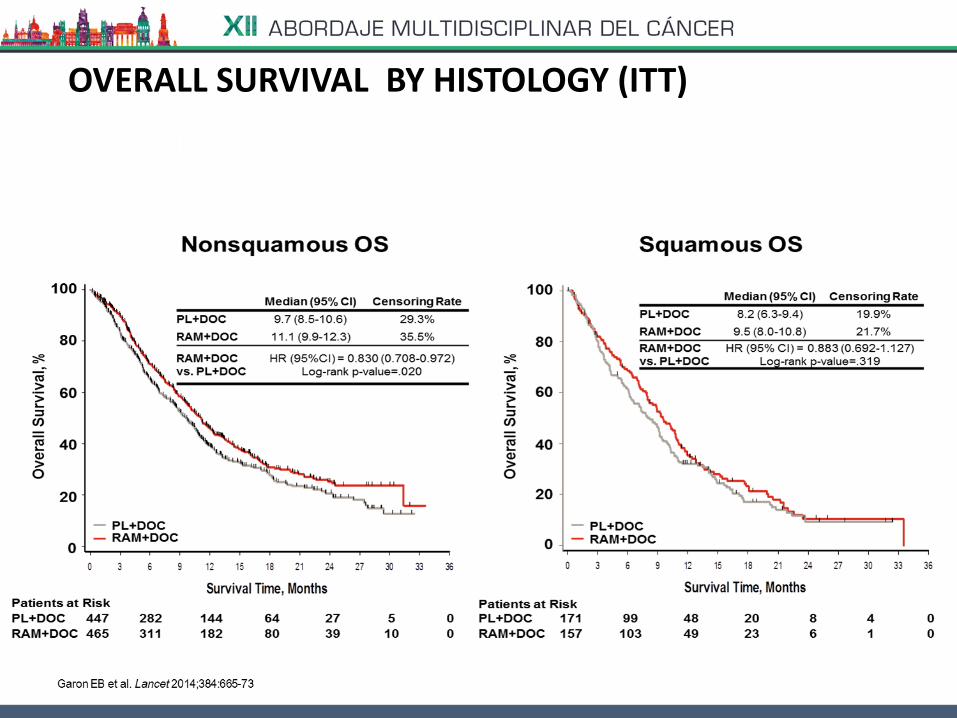
OVERALL SURVIVAL BY HISTOLOGY (ITT)

OVERAL SURVIVAL (HISTOLOGICAL SUBTYPES)

PROGRESSION-FREE SURVIVAL

RESPONSE RATES (RECIST 1.1)

RESPONSE RATES (HISTOLOGY SUBTYPES)

HEMATOLOGICAL ADVERSE EVENTS

ADVERSE EVENTS (ANTIANGIOGENIC THERAPY)

ADVERSE EVENTS (HISTOLOGY SUBTYPES)

QUALITY OF LIFE (LCSS, ASBI)

Nintedanib, a triple angiokinase inhibitor • Oral triple angiokinase inhibitor targeting:1,2
and RET and Flt-3
• No drug–drug interaction liability via CYP4503
• Manageable safety profile in combination with:
– Docetaxel3
– Pemetrexed4
– Paclitaxel/carboplatin5
– Gemcitabine/cisplatin6
1. Hilberg F, et al. Cancer Res 2008;68:4774–8; 2. Boehringer Ingelheim Data on file; 3. Stopfer P, et al. Xenobiotica. 2011;41:297–311; 4. Bousquet G, et al. Br
J Cancer 2011;105:1640–5; 5. Ellis PM, et al. Clin Cancer Res 2010;16:2881–9; 6. Doebele RC, et al. Ann Oncol 2012;23:2094–102.
IC50
(nmol/L)
VEGFR 1 / 2 / 3
34/ 21/ 13
PDGFR α / β
59/ 65
FGFR 1 / 2 / 3
69/ 37/ 108

VEGFs
FGFs
PDGFs
Endothelial cells VEGFRs, FGFRs
Pericytes PDGFRs
Smooth muscle cells FGFRs, PDGFRs
By targeting the 3 major angiogenesis signaling pathways Nintedanib prevents further tumor growth and related tumor escape mechanisms
Mode of action
Ligands Cell type/receptors Stimulation
a Angiokinase refers to tyrosine receptor kinases involved in promoting angiogenesis. Hilberg F et al. Cancer Res 2008; 68: (12). June 15, 2008] VEGF: vascular endothelial growth factor FGF: fibroblast growth factor PDGF: platelet -derived growth factor 38
Nin
ted
anib
Nintedanib, a triple angiokinase inhibitor

Nintedanib Combined with Docetaxel or Pemetrexed Enhances Antitumour Efficacy
• Combination of suboptimal doses of nintedanib and docetaxel or pemetrexed results in improved
antitumour efficacy compared with single-agent treatments and is well tolerated
39
NCI-H460 xenograft Calu-6 xenograft
0
200
400
600
800
1000
1200
1400
1600
1800
13 15 17 19 21 23 25 27 29 31 33 35
Days
Tum
ou
r vo
lum
e [
mm
³]
Nintedanib, 25mg/kg, qd, p.os
Docetaxel, 7.5mg/kg q7d, i.v
Nintedanib + Docetaxel
T/C
60%
69%
24%
Control
0,0
100,0
200,0
300,0
400,0
500,0
600,0
700,0
800,0
900,0
1000,0
0 5 10 15 20 25 30
Days
Tum
ou
r vo
lum
e [m
m³]
Control 125mg/kg, q7d,
64%
41%
24%
Pemetrexed i.p
Nintedanib + pemetrexed
Nintedanib, 50 mg/kg, qd
T/C
Hilberg F, Brandstetter I. 2007, J of Thoracic Oncol: August 2007

LUME-Lung 1: study design
BIBF 1120 200 mg BID p.o., Day 2–21 + Docetaxel 75 mg/m2 IV, Day 1,
21-day cycles (n=655)
Placebo BID p.o., Day 2–21 + Docetaxel 75 mg/m2 IV, Day 1,
21-day cycles (n=659)
n=1314
RANDOMIZE
Stratification: ECOG PS (0 vs. 1)
Prior bevacizumab (yes vs. no)
Histology (squamous vs. non-squamous)
Brain metastases (yes vs. no)
Stage IIIB/IV or recurrent
NSCLC patients after first-line chemotherapy (all histologies)
1:1
PD
PD
Number of docetaxel cycles not restricted Monotherapy allowed after ≥4 cycles of combination therapy
Regions: Europe/Asia/South Africa Accrual: 23 Dec 2008 to 09 Feb 2011
Reck M, et al. Lancet Oncol 2014; 15: 143
40

LUME-Lung 1: primary endpoint met – significantly longer PFS with the addition of nintedanib to docetaxel
Independent central review in all patients Reck M, et al. Lancet Oncol 2014;15:143–155.
100
80
60
40
20 Pro
bab
ilit
y o
f P
FS
(%
)
0 2 4 6 8 10 12 14 16 18 Time (months)
0
No. at risk
Nintedanib 565 295155 57 19 4 3 1 0
Placebo 569 250116 43 21 2 1 0 0
Nintedanib + docetaxel
Placebo + docetaxel
Median PFS (months) 3.4 2.7
HR = 0.79 (95% CI: 0.68–0.92); p=0.0019

OS: Key secondary endpoint
100
80
60
40
20
0
0 4 8 12 16 20 24 28 32 36
655 607 516 444 374 316 271 234 200 171 147 130 106 88 67 51 34 27 14
659 600 511 411 344 290 250 207 162 144 120 100 91 74 58 51 28 25 13
Pro
bab
ilit
y o
f su
rviv
al
(%)
Number at risk
Nintedanib
Placebo
Time (months)
Nintedanib + docetaxel
Placebo + docetaxel
Median, mo 10.1 9.1
HR (95% CI) 0.94 (0.83–1.05)
p value 0.2720
• All patients
OS = overall survival; mo = months; HR = hazard ratio; CI = confidence interval.
Reck M, et al. Lancet Oncol. 2014;15:143-55.

OS: Key secondary endpoint met • Patients with adenocarcinoma histology
Nintedanib + docetaxel
Placebo + docetaxel
Median, mo 12.6 10.3
HR (95% CI) 0.83 (0.70–0.99)
p value 0.0359
100
80
60
40
20
0
322 302 263 230 203 180 163 149 131 113 96 87 72 59 46 36 25 22 10
336 312 269 219 184 159 139 119 101 88 73 62 55 46 33 29 15 13 7
Pro
bab
ilit
y o
f su
rviv
al
(%)
52.7%
44.7% 25.7%
19.1%
Time (months)
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
OS = overall survival; mo = months; HR = hazard ratio; CI = confidence interval.
Reck M, et al. Lancet Oncol. 2014;15:143-55.
Number at risk
Nintedanib
Placebo

Best tumor response Independent Central Review in Major Histologies
Best response, n (%)
Adenocarcinoma Squamous Cell Carcinoma
Nintedanib + docetaxel (n=322)
Placebo + docetaxel (n=336)
Nintedanib + docetaxel (n=276)
Placebo + docetaxel (n=279)
Complete response (CR) 0 0 0 1 (0.4)
Partial response (PR) 15 (4.7) 12 (3.6) 13 (4.7) 6 (2.2)
Stable disease (SD) 179 (55.6) 136 (40.5) 123 (44.6) 92 (33.0)
Disease control rate* (CR + PR + SD)
194 (60.2) 148 (44.0) 136 (49.3) 99 (35.5)
Progressive disease 87 (27.0) 147 (43.8) 90 (32.6) 134 (48.0)
*Statistically significant improvement in disease control rate with nintedanib + docetaxel
(Odds ratio 1.93; p<0.0001 for adenocarcinoma and Odds ratio 1.78, p<0.0009 for squamous cell carcinoma)

LUME-Lung 1: hierarchical analysis used to reduce error rate and maintain power for the important OS endpoint
*Hanna N, et al. ASCO 2013. Abstract #8034; Hanna N, et al. ESMO 2013. Abstract #3418;
Kaiser R, et al. ESMO 2013. Abstract #3479.
Reck M, et al. Lancet Oncol 2014;15:143–155.
Prim
ary
en
dp
oin
t K
ey s
eco
nd
ary
en
dp
oin
t
Independently
assessed PFS
All histologies
OS Adenocarcinoma
Time since start of first-line therapy <9 months
OS All adenocarcinoma
OS All histologies
Significant
finding for
PFS at time
of OS
Significant
finding
Significant
finding
Previously analysed trial, LUME-Lung 2,
showed enhanced benefit in early progressing
adenocarcinoma tumours, so stepwise testing
was used to preserve power and reduce error*

LUME-Lung 1 Overall Survival Hazard ratio interaction: Final Analysis Feb 2013
• Time since start of first line was the only prognostic and predictive variable for the treatment effect of nintedanib in combination with docetaxel in patients with adenocarcinoma histology in LUME-Lung 11
• Time since start of first line is not a predictive variable in the squamous population
1. Kaiser R, et al. ESMO 2013 Abstract #3479
4.00
2.00
1.00
0.50
0.25
Haz
ard
rat
io
0 5 10 15 20 25
4.00
0.25
2.00
1.00
0.50
0 5 10 15 20 25
Squamous histology
Hazard ratio Lower 95% CI Upper 95% CI
Hazard ratio Lower 95% CI Upper 95% CI
Time since 1st-line therapy (months) Time since 1st-line therapy (months)
Adenocarcinoma histology
Reck M, et al. WCLC 2013 Abstract #3284

OS: Key secondary endpoint met • Adenocarcinoma + time since start of first-line therapy <9 months
Nintedanib + docetaxel
Placebo + docetaxel
Median, mo 10.9 7.9
HR (95% CI) 0.75 (0.60 to 0.92)
p value 0.0073
Feb 2013, 345 events
206 167 119 92 73 51 35 16 9 3
199 154 91 62 42 25 17 12 5 1
100
80
60
40
20
0
0 4 8 12 16 20 24 28 32 36
Pro
bab
ilit
y o
f su
rviv
al
(%)
Time (months)
44.7%
31.2%
17.0%
8.5%
Number at risk
Nintedanib
Placebo
OS = overall survival; mo = months; HR = hazard ratio; CI = confidence interval.
Reck M, et al. Lancet Oncol. 2014;15:143-55.

Early vs Late Progressors: Mechanistic Hypothesis
Rapidly progressing adenocarcinomas depend more strongly on vascularization for oxygen and nutrient supply than slowly growing tumors
High-level production of angiogenic growth factors by tumor cells
High intrinsic rate of tumor cell proliferation (oncogenome-dependent)
Rapid disease progression
High-level angiogenesis
nintedanib

Consistent Trend Towards Survival Benefit Regardless of Prior Treatment in Patients With Adenocarcinoma
CI = confidence interval; HR = hazard ratio; OS = overall survival. Krzakowski M, et al. Ann Oncol (2014);25(Suppl 4): iv158. Abstract 471P and poster; Mellemgaard A, et al. Ann Oncol
(2014);25(Suppl 4): iv157. Abstract 473P and poster; Boehringer Ingelheim data on file.
Overall Survival by Prior First-line Chemotherapy
Nintedanib
Placebo
No. at risk
Pro
bab
ility
of
surv
ival
(%
)
Prior taxane treatment 100
80
60
40
20
0
Time (months)
0 4 8 12 16 20 24 36 28 32
77 66 55 44 34 28 23 4 16
65 53 40 30 21 16 11 1 8
8
2
Prior pemetrexed treatment 100
80
60
40
20
0
Time (months)
0 4 8 12 16 20 24 36 28 32
61 48 37 30 24 17 14 0 7
62 65 49 31 25 18 13 1 12
2
5
Prior bevacizumab treatment 100
80
60
40
20
0
Time (months)
0 4 8 12 16 20 24 36 28 32
24 20 15 14 11 8 7 2 6
21 15 12 7 6 4 4 0 2
4
1
Nintedanib + docetaxel
Placebo + docetaxel
Median OS (months)
15.1 11.6
HR = 0.75 (95% CI: 0.51–1.11)
Nintedanib + docetaxel
Placebo + docetaxel
Median OS (months)
12.0 8.0
HR = 0.79 (95% CI: 0.53–1.18)
Nintedanib + docetaxel
Placebo + docetaxel
Median OS (months)
14.9 8.7
HR = 0.61 (95% CI: 0.31–1.20)

Adverse Events Occurring in ≥5% of the Patients With Adenocarcinoma
Reck et al. Lancet Oncol. 2014;15:143-55. Suppl.
Nintedanib + docetaxel (n=320) n (%)
Placebo + docetaxel (n=333) n (%)
All grades Grade ≥3 All grades Grade ≥3
Any AE 308 (96.3) 243 (75.9) 314 (94.3) 228 (68.5)
Diarrhoea 139 (43.4) 20 (6.3) 82 (24.6) 12 (3.6)
Neutrophil count decreased 131 (40.9) 116 (36.3) 135 (40.5) 116 (34.8)
ALT increased 121 (37.8) 37 (11.6) 31 (9.3) 3 (0.9)
Fatigue 99 (30.9) 15 (4.7) 98 (29.4) 14 (4.2)
AST increased 97 (30.3) 13 (4.1) 24 (7.2) 2 (0.6)
Nausea 91 (28.4) 3 (0.9) 59 (17.7) 2 (0.6)
White blood cell count decreased 89 (27.8) 63 (19.7) 94 (28.2) 61 (18.3)
Decreased appetite 75 (23.4) 4 (1.3) 52 (15.6) 5 (1.5)
Vomiting 62 (19.4) 4 (1.3) 41 (12.3) 2 (0.6)
Alopecia 56 (17.5) 1 (0.3) 68 (20.4) 0 (0)
Dyspnoea 54 (16.9) 15 (4.7) 52 (15.6) 20 (6.0)
Neutropenia 44 (13.8) 38 (11.9) 51 (15.3) 45 (13.5)
Cough 42 (13.1) 3 (0.9) 63 (18.9) 2 (0.6)
Pyrexia 39 (12.2) 2 (0.6) 47 (14.1) 1 (0.3)
Stomatitis 36 (11.3) 4 (1.3) 26 (7.8) 1 (0.3)
Haemoglobin decreased 35 (10.9) 3 (0.9) 46 (13.8) 7 (2.1)
Constipation 22 (6.9) 0 (0) 39 (11.7) 1 (0.3)
Adverse events were classified according to Common Terminology Criteria for Adverse Events version 3.0
LUME-Lung 1
• Only 1.2% of the patients in the nintedanib arm discontinued treatment due to diarrhoea
• 1.7% of the patients treated with nintedanib discontinued due to liver-related investigations

REEVALUACION TRAS 3 CICLOS
RP PULMONAR MANTENIMIENTO DE LA RESPUESTA SNC

RP A NIVEL RENAL

PROGRESION CEREBRAL SINTOMATICA
( cefalea, vómitos, inestabilidad)
RADIOTERAPIA HOLOCRANEAL

• Deterioro del estado general
• Comienza con astenia, hiporexia
• Ingreso por deterioro
RADIOTERAPIA HOLOCRANEAL
Progresión renal importante

Tto previo con bevacizumab
RP a los 3 ciclos de nintedanib ( misma
cavitación de la masa pulmonar-mismo patrón
radiologico)
Respuesta en paciente respondedora a la primera
línea ( >9 meses)
No resistencia cruzada entre antiangiogénicos
CASO CLÍNICO

SELECCIÓN DE PACIENTES
DESARROLLO DE RESISTENCIA
INMUNOTERAPIA
CUESTIONES PENDIENTES

Factors that Regulate the
Angiogenic Process
Reviewed in Welti et al. J Clin Invest 2013;123(8):3190-200.
Role in Angiogenesis Factors
Liberation of angiogenic factors from ECM VEGF, FGF
Tip cell guidance and adherence Semaphorins, neuropilins, plexins, ephrins, Unc5b, Robo4
Collective endothelial cell migration Ang1, aPKC
Lumen formation VE-cadherin, CD34, sialomucins, VEGF
Pericyte recruitmentPDGF-B, Ang1, Notch, Ephrin-B2, N-cadherin, Notch3,
Jagged1
Macrophages and myeloid cells Tie2, Ang2, PIGF, PHD2, SDF-1
Stalk elongation VEGFR-1, Notch, Wnt, Nrarp, Alk1, BMP9, SIRT1, EGFL7

Folkman, Nature Rev 2007;6:273-286

Limitations of Anti-Angiogenic Therapies
Moserle, Jiménez-Valerio & Casanovas Cancer Discovery, 2014

Anti-Angiogenic
Therapy
Anti-Angiogenic Therapies and Metastasis
Decreased Metastasis
TWO DISTINCT RESPONSES TO
ANTI-ANGIOGENIC THERAPIES:

Tumor Adaptation to Antiangiogenics: more Invasion and Metastasis
Pàez-Ribes et al. Cancer Cell 2009
T
Ac
Control (end-stage) Anti-VEGFR2 1 week Anti-VEGFR2 4 weeks
H&
E A
nti
-T a
nti
gen
T
Ac
T
Ac
50 µm 50 µm 50 µm
150 µm 150 µm 150 µm

How to Block Alternative Proangiogenic Resistance?
Biological base of combining anti-VEGFR and Immunotherapy ?
Vanneman & Dranoff Nat.Rev.Cancer 2012
Inhibition of VEGF-VEGFR exerts some Immune Activation!

• TRATAMIENTO EFICAZ
• COMPLEMENTARIO Y NO EXCLUYENTE
• BÚSQUEDA DE PACIENTES CANDIDATOS
• COMBINACIONES
• OPCIÓN TERAPÉUTICA EN CÁNCER DE PULMÓN
antiangiogénesis en cáncer de pulmón
















