TEJIENDO LAZOS PARA UNA MATERNIDAD … · Marcela Tapia, Patricia Poppe, Robert Ainslie Adaptación...
162
-
Upload
truongphuc -
Category
Documents
-
view
217 -
download
0
Transcript of TEJIENDO LAZOS PARA UNA MATERNIDAD … · Marcela Tapia, Patricia Poppe, Robert Ainslie Adaptación...
2
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
¡Gracias por sus aportes!
Productores educativos y AsesoresMarcela Tapia, Patricia Poppe, Robert Ainslie
Adaptación para GuatemalaClara Zuleta, Demetrio Margos,
Ingrid Valenzuela, Domingo Vásquez,Ernestina Vásquez, Patricia De León Toledo
Recurso humano a cargo de la investigaciónDemetrio Margos, Ernestina Vásquez,
Domingo VásquezCarlos Lec, Dorcas Saloj, Marcela Ajtzí,
Alejandro ChamánPatricia De León Toledo
Revisores técnicosMisterio de Salud Pública y Asistencia Social de
GuatemalaPrograma nacional de Salud Reproductiva, Unidad
Ejecutora, USAID
Nota: Es importante indicar que este en este documento se ha utilizado el género masculino en la mayoría deocasiones en que el texto puede referirse tanto a mujeres como a hombres. Se ha adoptado esta medida
exclusivamente por razones de simplificar el texto sin ninguna connotación de preferencia.
Esta publicación fue posible con el apoyo de la Agencia para el Desarrollo Internacional (AID), bajo los términosdel contrato No. C.A. HRN-A-00-98-00043-00. Las opiniones expresadas aquí son exclusivas de los autores y no
necesariamente reflejan los puntos de vista de la AID
Guatemala, enero 2004
ColaboradoresPersonal técnico y administrativo del Proyecto de
Salud Materno NeonatalDirecciones de Area de Salud: El Quiché,
Totonicapán y Sololá,Comadronas de Cantel, QuetzaltenangoComadronas de Santa Catarina Palopó
Grupos de mujeres, hombres, líderes, comadronas,proveedores
(propósito de la investigación)
Lucrecia Cúmes, José López,
FotografíasDemetrio Margos, Patricia De León Toledo
Diseño Gráfico y DiagramaciónAna Victoria Chajón y Roberto A. Pérez García
3
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
ÍNDICEÍNDICEÍNDICEÍNDICEÍNDICEINTRODUCCIÓN 5
PARTE I:LA MATERIA PRIMA 71. La riqueza de los diferentes actores de cambio 72. Visiones del mundo y visiones de la salud 93. Partiendo de la realidad: trabajando con las
iniciativas y organizaciones existentes 104. Hacia la inclusión de género 125. Del pedido de ayuda al empoderamiento 13
PARTE II:EL INSTRUMENTOENCUENTROSVIDEO-PARTICIPATIVOS 141. Los objetivos de la investigación - acción 152. El instrumento encuentros
video-participativos y su metodología de uso 15
Paso #1. Creando una buena relación 16
Paso #2. Conociendo al equipo facilitador,a los participantes y presentandoel proyecto 17
Paso #3. Creando un ambiente fraterno:El ejercicio de rompehielo 19
Paso #4. Presentando historiasde vida: Los videos 1 y 2 20
Paso #5. Priorizando los atributosde calidad que el servicio de saluddebe practicar desde la perspectivade la comunidad 23
Paso #6. Conduciendo elmapeo comunitario 24
Paso #7. Finalizando el encuentroy continuando la acción colectiva 26
3. El equipo humano facilitadorde los encuentros video participativos 27
3.1El equipo humano facilitador 273.2Las cualidades y habilidades
del equipo facilitador 283.3Consejos prácticos para
la animación de grupos 29
4. Los participantes de la comunidadinvitados a los encuentrosvideo participativos 29
4.1El proceso de invitaciónde los participantes 29
4.2Los criterios de selección de losparticipantes 30
4
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
5. La organización previa y la logística 315.1Gestión de recursos 325.2Gestión del tiempo 335.3Gestión del espacio 36
6. Información recopilada 376.1 La sistematización de la experiencia 376.2 El análisis de los encuentros 38
7. El uso del instrumento dentro de un proceso 39
PARTE III:LOS LAZOS 411. Valoración e incentivos 412. El retorno a la comunidad 423. Tejiendo lazos 44
PARTE IV:ANEXOS 46
5
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
INTRODUCCIÓN
Este manual es diseñado para acompañar allector, paso a paso, en la aplicación de uninstrumento de investigación-acción dentro de unprograma de salud materna y neonatal. Estemétodo de investigación (instrumento oherramienta) es llamado “encuentro video-participativo.” Un encuentro video-participativo esuna reunión de discusión en la que se usantestimonios, relatos e imágenes en video paramotivar al diálogo.
El ahora conocido “tejido de lazos” refleja loscomponentes y las características del proceso deinvestigación-acción en el que dicho método deinvestigación se incluye. Elegimos esta analogíaporque el “tejido de lazos” es un elemento cultural“endógeno”, es decir, que se construye desde lacomunidad misma y la representa. Los lazosrepresentan a la vez permanencia y cambio, yaque toda tradición tiene pasado (tiene historia), asu vez tiene futuro y evoluciona con el tiempo. Loslazos son, por lo tanto, no sólo productos sinotambién procesos ya que se van creando yrecreando a través del tiempo. Es más, los lazossimbolizan la comunidad, el apoyo mutuo, laformación de redes, la solidaridad.
El manual propone tejer lazos para unamaternidad saludable a través de un proceso queimplica aprendizaje, reflexión y acción. La primeraparte del manual, “La Materia Prima,” pone enrelieve el recurso esencial y más valioso para estetrabajo; el recurso humano, es decir, lacomunidad, el personal de salud y los agentesexternos que trabajan juntos creando yfortaleciendo lazos para mejorar la salud. Lasegunda parte, titulada “El Instrumento” contieneuna descripción detallada con instruccionesprecisas para el uso de los “encuentros video-participativos” como método/herramienta deinvestigación-acción. La tercera parte, “Los Lazos”puntualiza el proceso de diálogo y participacióncomunitaria que es la esencia misma del procesode investigación-acción.
Las partes II y III son las más resumidas delManual, pero esenciales en contextualizar y enhacer comprender los principios que orientan lautilización del instrumento. La parte II delmanual es la más extensa, ya que en ella seproporcionan indicaciones detalladas quepermitirán al lector apropiarse del instrumentopaso a paso, para construir lazos con la
6
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
comunidad. Para completar el manual hemosincluido en la sección de anexos algunos docu-mentos para que el lector pueda fotocopiarlos cadavez que lo necesite.
Para tener una visión más completa del procesode investigación-acción y utilizar el instrumentoen armonía con los objetivos de aprendizaje mutuoestablecidos en el marco de este trabajo, esrecomendable leer el manual como un todo.Aunque cada parte del manual aborda temasdiferentes y proporciona elementos para lareflexión que se pueden aprovechar separa-
damente, las tres partes se complementan yrepresentan, en efecto, un todo dentro del procesode investigación-acción. El compromiso delpresente manual corresponde con la meta últimaque inspiró la elaboración del instrumento, es decir,crear lazos cada vez más fuertes en apoyo a la viday a la necesidad de tomar acciones desde lacomunidad cuando ésta y sus familias se enfren-tan a casos de emergencia obstétrica. Se trata decontribuir a lograr un cambio social, a determinarcompromisos y acciones de largo plazofortaleciendo las redes sociales existentes en elámbito de la comunidad.
7
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
PARTE I:LA MATERIA PRIMA
Todo proceso de investigación-acción para elcambio social debe enfocarse en el potencialexistente en las comunidades. Sin negar la faltade insumos e infraestructura que aquejan a lascomunidades, es esencial reconocer como punto departida del trabajo con la comunidad, los recursosya existentes. En este sentido, más allá de losrecursos materiales con los que se puede contar,se debe poner en relieve el gran potencial humanoexistente en cada comunidad. A éste se unenequipos de trabajo y personas del exterior,comprometidos en apoyar a la comunidad en supropio proceso de cambio social. Los diversospárrafos en esta primera parte del manualproporcionan pistas de reflexión sobre la valiosa“materia prima” existente en las comunidades ysobre la necesidad y pertinencia de partir de loque existe, de las fortalezas y las potencialidadesde cada comunidad. A continuación se ofrecenalgunos modelos para guiar al lector en el uso yadaptación del presente Manual teniendo encuenta la necesidad de incluir a los grupos másvulnerables de la comunidad en el proceso deinvestigación-acción. Veamos:
1. La riqueza de los diferentes actores decambio
Un proyecto o una labor colectiva no empieza porgeneración espontánea. En este sentido, el papelde los “agentes de cambio” de la comunidad y delos agentes catalizadores externos es fundamentaldurante el inicio de todo proyecto. Los “agentes decambio” de la comunidad son personas que ejerceninfluencia sobre los demás y son capaces degenerar cambio dentro de la comunidad. Son ellaslas que a menudo se dan cuenta de que existe unproblema y empiezan a movilizar a la comunidadpara encontrarle una solución. A las personas quevienen de afuera a apoyar a la comunidad se lesllaman “agentes catalizadores externos.” El papelde estos últimos es facilitar el proceso de cambioen la comunidad, utilizando herramientas comola que proponemos en este manual. A veces sonellos los que le proponen a la comunidad trabajarsobre un problema específico que ha sidoidentificado, por ejemplo, a partir de inves-tigaciones. Su papel en tanto facilitadores no es el
8
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
de imponer una agenda a la comunidad sino el detrabajar con ella para que ésta:
identifique y tome conciencia delproblemadecida qué es lo que se debe hacer parasolucionarlo.
El facilitador orienta a la comunidad y entra endiálogo con ella para tomar acciones adecuadas,sin imponer su punto de vista de maneraunilateral. Los agentes de cambio de la comunidady los agentes catalizadores externos pueden juntosayudar a la comunidad a identificar un problemay a establecer metas comunes para solucionarlo.
Hay sectores de la comunidad especialmenteafectados por la problemática que se quiereabordar y que es fundamental involucrar en elproceso: en este caso, las cuestiones de saludmaterna y neonatal tocan directamente a lasmujeres en edad reproductiva y a sus comadronas.Los jefes de familia son otro grupo clave, ya quede ellos dependen a menudo las acciones que setomen en casos de emergencia. Es importantetener en cuenta, durante la investigación-acción,el papel real o potencial que cada uno de estosactores tiene dentro de la comunidad. Hay queconsiderar, especialmente, las maneras en las quese puede involucrar a los grupos que estángeneralmente ausentes en las esferas de toma dedecisión de la comunidad.
No existe un modelo único, predeterminado decómo iniciar un proceso de cambio dentro de unacomunidad con el apoyo de la investigación-acción.Las características que la experiencia adoptedependerán de las personas involucradas, de losmodos de organización existentes y de lacoyuntura. Lo importante, en todo caso, dentro deeste proceso es lograr revertir el enfoque de trabajocentrado en las deficiencias y carencias de lacomunidad. Contrariamente a ese enfoque,proponemos para este trabajo el reconocimientode las fortalezas de la comunidad y de los distintosactores involucrados. Es importante estarconscientes de que el papel de cada una de las/los…
mujeresespososcomadronaslíderesagentes de cambio de la comunidadagentes catalizadores externosautoridades
Es esencial y se debe valorar y respetar loque cada uno/a desde su posición puedeaportar al proceso de investigación-acción.
Tomar como punto de partida las fortalezasde los actores involucrados ayuda a reforzarlos lazos entre la comunidad y los agentes decambio externo.
9
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Ambos se reúnen con la convicción de quepueden avanzar juntos…
reapropiándose del pasadofocalizándose en el presente, eincorporando en sus acciones una visióndel futuro.
2. Visiones del mundo y visiones de la salud
Muchas experiencias de desarrollo fallaron en elpasado por no tener en cuenta el punto de vistade los interesados y por tratar de imponer patronesde comportamiento ajenos a la cultura local. Elenfoque centrado en las fortalezas vieneacompañado del reconocimiento de las diferenciasculturales entre los agentes catalizadores externosy la comunidad. El reconocimiento de estasdiferencias implica, al mismo tiempo, la necesidadde entender cómo concibe “el Otro”; el que esdiferente a mí, sus propios problemas y surealidad. Sin necesidad de aceptar ciegamente lastradiciones que pueden ser dañinas para la salud,es importante conocer qué significa la salud parala comunidad, cuáles son sus prioridades, valoresy tradiciones. El intercambio abierto con lacomunidad sobre sus costumbres y creencias nospuede llevar a descubrir tanto prácticastradicionales que se tendrían que modificar, comocostumbres que se deberían reforzar e integrar ala práctica de la medicina occidental.
En el contexto de esta investigación-acción esparticularmente importante conocer el punto devista de la comunidad sobre los servicios, o lo quellamamos los “atributos de calidad” de los servicios.Los “atributos de calidad” son las característicasde los servicios que van a hacer que los usuarios yusuarias aprecien o no el servicio. Por ejemplo,una persona puede quejarse de que la hacenesperar mucho antes de atenderla en el centro desalud. En este caso, el atributo de calidad es “laatención rápida.” Otra persona puede decir queella va al puesto de salud porque sabe que elpersonal que atiende allí la va a tratar con cariño.En este caso la persona habla del atributo decalidad “buen trato.” En el primer caso, al serviciole falta este atributo mientras que en el segundo,el servicio cuenta con el atributo o característicaque es importante para ese usuario/usuaria. Elhecho de que un servicio cuente con un atributo ono, puede llevar a ese usuario/usuaria a elegir unservicio u otro o simplemente, no acudir a losservicios. Es por eso que es importante conocerlos atributos de calidad desde el punto de vista dela comunidad.
Este proceso de investigación-acción propone unaperspectiva desde adentro, es decir, que parta delpunto de vista de la comunidad. El escuchar elpunto de vista de la comunidad, ayudará aentender mejor los modos de ser y de hacer de lacomunidad. Esto significa que vamos a escuchar
10
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
lo que la gente nos dice y a aprender de ella y conella. No vamos a ser capacitadotes, sinofacilitadores que van a las comunidades paraconocer el punto de vista de sus miembros sobrela salud y sobre los servicios. Esta perspectivadesde adentro ayudará por ejemplo, en el caso quenos ocupa, a comprender mejor qué es lo que lagente aprecia de los servicios y qué es lo que sepodría mejorar para que la gente se sientasatisfecha con ellos. La perspectiva desde adentroayudará también a comprender mejor cómo losmiembros de la comunidad hacen frente a lassituaciones de emergencia obstétrica y qué los llevaa actuar de una u otra forma. Esto permitirá eldesarrollo de actividades adaptadas al contexto,que tengan en cuenta el punto de vista y larealidad (psico-social, socio-económica y cultural)de los involucrados.
Lo más importante en las conversaciones con losmiembros de la comunidad es distinguir bien loque “yo” pienso de lo que “ellos” piensan. Hay quehacer un esfuerzo para dejar de lado toda las ideasque tengamos sobre la comunidad para escucharlacon nuevos oídos y poder comprender lo que ellanos dice.
En un encuentro intercultural, la apertura haciala visión del mundo de la comunidad vieneacompañada, necesariamente, de la toma deconciencia de los propios prejuicios, valores ynormas culturales.
3. Partiendo de la realidad: trabajando conlas iniciativas y organizaciones existentes
El enfoque utilizado en este manual implica partirde la realidad existente en lugar de tratar deimponer una agenda o programa que no lepertenece a la comunidad. En la medida de loposible, se debe tratar de integrar la investigación-acción dentro de las iniciativas y en las áreas detrabajo de las organizaciones existentes en lacomunidad.
Las experiencias de la comunidad al nivelde:
Desarrollo de proyectosOrganizaciones comunitarias
Gestión colectiva (por ej.,recolección de fondos)
son parte del bagaje de la comunidad que sedebe tener en cuenta durante lainvestigación-acción.
Por ejemplo, el proyecto de construcción de unacasa materna o una maternidad comunitariapuede ser el motor que anime el proceso deinvestigación-acción con la comunidad. De lamisma manera, se debe estar consciente en todomomento que el proceso iniciado en la comunidad
11
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
debe ser devuelto a ella, ya que le pertenece, yque las vías privilegiadas para hacerlo son amenudo los comités o grupos de salud ya existentesen la comunidad. En muchas ocasiones en lo querespecta a la salud materna y neonatal, se puedepensar en ampliar y/o reforzar las actividades derecolección de fondos que ya se hacen de manerapuntual en la comunidad. Por ejemplo, haycomunidades en las que se hacen colectas de fondospara casos de fallecimiento o de emergencia. Enlugar de proponer algo nuevo, se puede mejorarla organización, planificación y gestión de dichasactividades como parte de un “Plan de EmergenciaComunitario”, nombre que bien podría cambiarsegún lo que decida la comunidad. Cuando unoparte de lo que ya existe, se adapta mejor al medio.El proceso de investigación-acción puede ayudartanto a identificar como a mejorar experiencias yaexistentes en la comunidad. Es importante pues:
Estar atentos a las oportunidades de mo-vilización y participación existentes en lacomunidadInvolucrarse en núcleos de organizacióncomunitaria ya existentesMejorar lo que ya existe en lugar de “re-inventarla rueda”Igualmente es importante tener en cuenta elcalendario de actividades agrícolas y las agen-das propias de cada comunidad para podercolaborar más eficazmente con ella. Porejemplo, de nada sirve tratar de organizar
reuniones con hombres en un período decosecha cuando todos estarán fuera de lacomunidad. Tampoco sería útil organizarreuniones para conversar sobre la saludmaterna y del recién nacido cuando lacomunidad está en una semana de celebracióno tiene algún problema urgente que resolver(por ejemplo, una inundación).
No hay que olvidar que otro actor principal en elproceso de investigación-acción es el personal desalud. Lo mismo que abogamos por la comunidadse aplica también a los prestadores de serviciosinvolucrados en este trabajo. Por ejemplo, no seríarealista pensar que los enfermeros o lostrabajadores sociales podrían dejar de lado suslabores en los servicios de salud para dedicarsepor completo a facilitar “encuentros video-participativos”. Los que estén interesados enhacerlo tendrán que: 1) planificar su trabajo detal manera que dichos encuentros complementensus labores; 2) analizar hasta qué punto puedenasumir las funciones del equipo facilitador de losencuentros y lograr que los participantes sesientan libres de contarles las cosas tal como sony no como “deberían ser.” Sabemos, al mismotiempo, que se pueden reforzar las funciones delpersonal de salud a partir de actividades previstasdentro de la investigación-acción. Por ejemplo, el“mapeo comunitario” previsto dentro y más alláde los encuentros video-participativos, es unaherramienta para ubicar los recursos disponibles
12
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
en casos de emergencia en la comunidad, lo cualviene a reforzar una de las funciones de losfacilitadores comunitarios en las salassituacionales. Como sabemos que los facilitadorescomunitarios deben hacer mapas de lascomunidades, la herramienta del mapeo dentrode la investigación-acción debe servir paraayudarlos en esa tarea. Se trata de identificar enel terreno la mejor manera de involucrar alpersonal de salud en las actividades deinvestigación-acción desde donde están.
El uso de los encuentros video-participativos comoherramienta de investigación-acción debeadecuarse a la realidad de la comunidad y de losservicios de salud, partiendo de lo que existe parareforzarlo. El proceso mismo de reflexión y deacción llevará a la formulación conjunta depropuestas para efectuar cambios en beneficio detodos.
4. Hacia la inclusión de género
Partir de la realidad no significa aceptar el statusquo (las cosas como son) y las relaciones de poderdesiguales que pueden existir en la comunidad.Se trata de incluir y no de excluir y, dentro de losgrupos vulnerables, las mujeres son a menudoexcluidas de la toma de decisiones, incluso sobreasuntos que les interesan directamente, como esla muerte materna.
A pesar del papel preponderante que las mujeresjuegan en la comunidad en general y en la saluden particular, a menudo ellas están ausentes enlos comités de salud, los comités pro-maternidadu otros núcleos de organización de lascomunidades. Sin embargo, cuando se les da laoportunidad de participar, son capaces de articularsus ideas y de hacer propuestas de las que podríanbeneficiarse tanto los comités como la comunidaden general.1 Se hace necesario, propiciar laparticipación de las mujeres a todo nivel y endistintos momentos de la investigación-acción,incluyendo su participación activa en los comitésde salud y pro-maternidad. Esto se puede lograr através de distintas acciones como:
Incentivar la participación en los encuentrosvideo-participativos de mujeres de la comunidadque no acostumbran participarDiscutir con la comunidad de qué manera sepodría incluir a liderezas, comadronas y mujeresde la comunidad en general en comités en losque se toman decisiones importantes de salud.
Los agentes catalizadores externos dentro de lainvestigación-acción pueden jugar un papelimportante en este sentido, ya que aportan unpunto de vista diferente (es decir: las mujeres
1 Esto lo pudimos confirmar durante encuentros video-participativos que se realizaron en la Zona Reina.
13
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
pueden y deben participar) y son capaces deinfluenciar la opinión de los miembros y líderesde la comunidad.
5. Del pedido de ayuda al empoderamiento
Puede suceder que al llegar a una comunidad susmiembros y representantes pidan ayuda al equipoexterno para solucionar los problemas que losaquejan. La comunidad puede incluso expresar:
Su sentimiento de impotencia ante lassituaciones que tiene que enfrentar.Su sentimiento de incapacidad para poderresolver los problemas.Su creencia de que sólo la gente que viene deafuera es capaz de cambiar la situación.
A menudo los miembros de la comunidad pierdende vista lo que están haciendo día a día paramejorar su situación y la de sus hijos. Tienen unaimagen de sí mismos centrada más en sus propiascarencias que en sus fortalezas. Y esto mismosucede, a menudo, con algunas personas de fuerade la comunidad, que ven ante todo las carenciasy no las fortalezas de la misma. Lo que se quiereen esta investigación-acción es justamente revertiresa situación y sacar a relucir las fortalezas y elvalor de las iniciativas de la comunidad.
No hay que negar las necesidades concretas deayuda de la comunidad, al contrario, debemos
estar atentos a ellas. Lo que se debe evitar es caeren el “paternalismo” o “asistencialismo” queconsiste en hacer las cosas por la comunidad enlugar de hacerlas con ella. Hay que recordar queel proceso de aprendizaje mutuo que se inició debeayudar a desarrollar en los individuos y en lacomunidad:
La confianza en sí mismos.El sentimiento de ser capaz de hacer las cosas.Las habilidades necesarias para llevar a cabolos proyectos.
Se trata, por ejemplo, de orientar a la comunidadsobre cuáles son los pasos a seguir para formalizarun acuerdo y no hacer las gestiones por ella. Hayque sacar a relucir logros pasados y presentesdándole ánimo a la gente para seguir adelante.En otras palabras, se debe tratar de enfatizar encada momento la capacidad transformadora de lacomunidad misma. Es así como un pedido deayuda puede convertirse en una oportunidad deempoderamiento. A partir del diálogo con lacomunidad se puede propiciar un proceso decambio social, en el cual la comunidad toma lasriendas y se siente capaz de buscar soluciones asus problemas—garantía del sostenimiento de lasacciones a largo plazo. El uso del instrumento, talcomo lo describimos en la siguiente parte delmanual, se inserta dentro de ese contexto decambio social y de empoderamiento.
14
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Una vez que tenemos claro el potencial existenteen la comunidad y el valor de la “materia prima”,es necesario encontrar el instrumento y el procesometodológico adecuado para trabajar con losgrupos comunitarios. Basándose en la metaúltima del proyecto que es, promover unamaternidad saludable a través de:
Valorar y reforzar la participación de lacomunidad en los distintos aspectos; elcuidado de la salud materna y neonatal y enla mejoría continua de losservicios parasalvar vidas.
Se analiza la riqueza del video como generadorde ideas y discusión, de reflexión y de “vivencia”interna de los problemas de salud. Al igual, la
participación activa de la comunidad analizandosus problemas y empoderándose para identificarsoluciones y movilizarse colectivamente da pasoa la propuesta de crear espacios de diálogo,concertación y acción colectiva a nivel comunitario.Se proponen entonces, los “encuentros videoparticipativos” como instrumento y proceso paraalcanzar la meta mencionada. A continuación seexplican detalladamente los objetivos de lainvestigación-acción, las características delinstrumento del encuentro video participativo, lametodología y proceso para su uso, el rol facilitadora cumplir por parte del equipo humano, la activaparticipación de la comunidad en los “encuentros”,y las labores de logística que asegurarán que los“encuentros” fluyan con la confianza, la capacidadanalítica y el deseo de acción de parte de lacomunidad para alcanzar un compromiso porsalvar vidas.
PARTE II:EL INSTRUMENTOEncuentros Video-Participativos
15
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
1. Los objetivos de la investigación - acción
La investigación-acción tiene como tema central,indagar conjuntamente con la comunidad lascausas de la muerte materna y neonatal, así comola disposición del servicio de salud para asistir anteun caso de emergencia obstétrica. Como objetivostenemos:
Conocer el punto de vista de la comunidad sobrelos servicios de salud, más específicamente enlo que se refiere a la salud materna y neonatal.2
Facilitar la participación activa de la comunidadpara analizarse así mismos ante un caso deemergencia obstétrica, observando decisionesy toma de acción.
Acompañar en su proceso de apropiación de unprograma dirigido a la elaboración de Planesde Emergencia Comunitarios3 para salvar vidasde madres e hijos/as.
En términos generales, el instrumento y procesode los “encuentros video-participativo” sirvenentonces para acercarnos a la comunidad, “tejerlazos” con ella y aprender conjuntamente:
Lo que piensa y siente la comunidad conrespecto a los servicios y las causas de muertematerna y neonatal.
Las barreras y los facilitadores reales ypotenciales para el uso de los servicios.
Las creencias, actitudes y prácticas que influyenlas decisiones sobre salud en la comunidad.
Las aspiraciones de la comunidad en lo querespecta: (a) la organización para el manejo decasos de emergencia; y (b) el trato y tratamientoen los establecimientos de salud.
Los recursos existentes en la comunidad queconstituyen o pueden constituir oportunidadesde organización para la formulación de losPlanes de Emergencia Comunitarios.
2. El instrumento encuentros video-participativos y su metodología de uso
El instrumento desarrollado para llevar adelanteel proceso de investigación-acción ha sidodenominado “encuentro video-participativo” comofue mencionado anteriormente. Uno de sus ejes
2 Para tratar otros temas usando el mismo método, setendría que adecuar tanto el contenido de los videoscomo la guía de preguntas.
3 La elaboración de los Planes de EmergenciaComunitarios supone, entre otros, la creación oconsolidación de redes comunitarias para tratar casosde emergencia.
16
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
centrales es la utilización de la imagen como mediopara registrar testimonios e historias de vida conrelación a un tema de salud elegido. Al presentarestas historias en video, sobre todo cuando éstasson trabajadas y producidas conjuntamente conla comunidad, los participantes en las reunionesó “encuentros”, se identifican con los personajes,las situaciones encontradas y lo vivido en supropia comunidad. Así, se genera una discusiónmuy rica que motiva a que los participantescuenten sus propias historias, ofrezcan puntos devista diferentes y/o complementarios, reflexionensobre lo visto y escuchado, y en muchos de loscasos, negocien propuestas para la toma de acción.De ahí la utilización de lo que llamamos“encuentros video-participativos” con lascomunidades, en contraste al uso de técnicas derecolección de datos sobre la comunidad. Se tratapues de un instrumento de aprendizaje mutuo ymás que una técnica, constituye una herramientapara propiciar y sostener el cambio social dentrode la comunidad.
En tanto la organización de los “encuentros”transcurre en el seno de la comunidad, se ofrece acontinuación una guía metodologíca de trabajo ydiscusión que nos ayuda a avanzar por el procesodel “encuentro video-participativo”. El “encuentro”está organizado alrededor de siete pasos claves,llamados:
1. Creando una buena relación
2. Conociendo al proyecto, el equipo facilitador ylos participantes
3. Creando un ambiente fraterno: el ejercicio derompehielo
4. Presentación historias cortas de vida: losvideos 1 y 2
5. Priorización de los atributos de calidad desdela perspectiva de la comunidad
6. Conduciendo el mapeo comunitario7. Finalizando el encuentro y continuando la
acción colectiva
Paso #1. Creando una buena relación
El primer contacto del equipo facilitador con losparticipantes es crucial en el manejo de lasreuniones de trabajo y de los “encuentros videoparticipativos”. El equipo facilitador,4 aunqueno esté en su propia comunidad, se convierteen anfitrión y, como tal, es el que da labienvenida a los participantes desde elmomento en que ellos llegan al lugar fijado parael encuentro. Para que pueda cumplir bien coneste papel de anfitrión, el equipo facilitadordebe:
Ubicarse en la sala donde se lleve a caboel encuentro con anticipación para podersaludar a los participantes en la medidaque van llegando.
4 Explicamos la composición de este equipo en la secciónsiguiente.
17
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Conversar informalmente con los parti-cipantes y darles una darles una bien-venida respetuosa y amistosa.Invitarlos a dar sus datos (socio-demo-gráficos) a la persona encargada, quienpuede explicarles que se les pide estainformación sólo para tener una ideasobre sus edades, el número de hijos quetienen y si ya utilizaron los servicios desalud.
Hay que aprovechar el momento del refrigeriocomo un espacio para seguir desarrollando unabuena relación con la comunidad. En esemomento, ya sea a la mitad o al final delencuentro el equipo facilitador sirve losrefrigerios e interactúa con los participantes. Deigual manera que cuando se recibe a un amigoen casa, se atiende a los participantes de lamejor manera posible, asegurándose de que anadie le falte algo, conversando con ellos.
Un obstáculo a la interacción del equipofacilitador con los participantes puede ser elhecho de que no todos hablan el mismo idioma.En ese caso, los miembros del equipo facilitadorque hablan el idioma de los participantes,sirven de puente entre estos últimos y el restodel equipo. Además es importante recordar quemás allá de la comunicación verbal, el lenguajeno verbal, la actitud, el estar atento a que anadie le falte algo, son signos que los par-
ticipantes perciben y que contribuyen a lacreación de una buena relación con ellos.
Paso #2. Conociendo al equipo facilitador, a losparticipantes y presentando el proyecto
La presentación del proyecto, del equipofacilitador y de los participantes reunidos esesencial. La manera en que se haga estapresentación motivará a que los “asistentes” seconviertan en “participantes reales” y a sentirselibres de exponer sus puntos de vista.
Durante la presentación del proyecto y delequipo facilitador, el facilitador debe:
Explicar el objetivo del encuentro yagradecer la participación de los presentes:Se menciona que el tema que interesaparticularmente es el de la salud de lasmamás y de los recién nacidos. Losparticipantes pueden estar acostum-brados a participar en sesiones de capa-citación o en grupos de discusión en losque un equipo externo va a impartir uobtener información de la comunidad.Durante la presentación del proyecto, elfacilitador puede aclarar que no se trata,en este caso, de una sesión de capacitacióny que lo que quiere el grupo facilitador esaprender con la comunidad y conocermejor sus puntos de vista sobre la salud.
18
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Tampoco busca recoger información e irse.Lo que quisiera es ver cómo puede apoyara la comunidad. En este sentido, esimportante también tener cuidado de nocrear expectativas falsas en la comunidad:hay que aclarar, si es necesario, el tipo deapoyo que se les puede brindar y loslímites dentro de los cuales se actúa. Porejemplo, debe quedar claro que esteequipo no tiene fondos que ofrecer a lacomunidad. Lo único que se puede ofreceres apoyarlos con ideas de cómoorganizarse para poder salvar las vidasde personas que se les presenta unaemergencia de un momento a otro en lacomunidad.
Explicar a los participantes el carácterconfidencial y anónimo de susintervenciones: Es muy importanteasegurar a los participantes de que nadieserá citado con nombre y apellido y quelas opiniones que viertan durante lasdiscusiones no serán repetidas o utilizadascontra su voluntad.
Explicar la necesidad de grabar la reuniónpara tener una “memoria” del encuentro:El equipo facilitador debe ocuparse de lagrabación de cada encuentro. Cadagrabación es transcrita para facilitar,posteriormente el análisis de la infor-
mación recogida. Los participantes sepueden preguntar por qué los estángrabando y sentirse intimidados por elaparato colocado en medio de la sala. Seaconseja pedir a los participantes suconsentimiento para la grabación,asegurándoles una vez más el anonimatoy la confidencialidad. En algunascircunstancias, el no pedir permiso parala grabación puede crear desconfianza enlos participantes. En esos casos, es mejorlimitarse a explicar lo más claramenteposible la necesidad de tener undocumento que ayude a recordar lodiscutido: es también una manera derespetar lo que la gente ha dicho, ya queno nos fiamos sólo de nuestra memoria.Si además de la grabación en audio, segraba la reunión en video, se les puedeofrecer a los participantes ver la grabaciónen un segundo momento. A la gente legusta, generalmente, ver su imagen en lapantalla y es una manera de compartircon ellos lo que compartimos durante losencuentros.
Explicar el procedimiento que se seguirádurante el encuentro: El facilitador lesexplica a los participantes que van a verjuntos un par de películas cortaspreparadas para la reunión y queconversarán informalmente de lo que
19
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
cada uno piensa. Les explica que despuésse harán también un par de presen-taciones en grupo.5
Pedir que lo interrumpan en cualquiermomento si hay algo que no está claro: Loque se quiere es que todos participen ypara eso tenemos que entendernos bien.Se aprovecha para preguntar a losparticipantes si tienen alguna pregunta osi quieren alguna aclaración antes deseguir.
Presentar a los demás miembros del equipoy pedir a los participantes que se unan a lapresentación: Ya sea que el facilitadorpresenta a los otros miembros del equipo,o mejor aún, los otros miembros del equipose presentan frente a los participantesbrevemente. Cada uno da su nombre ymenciona cuál será su participacióndurante la reunión. Si son proveedoresde salud (PS), no deben mencionar suscargos en el sector, ya que eso podría, porun lado, intimidar a los participantes, ypor otro, crear un contexto más de sesiónde capacitación que de intercambio
informal. De igual manera, los asistentesa la reunión también deberá presentarseagregando algunas palabras si así loquisieran. El equipo facilitador puedetambién participar en el ejerciciorompehielo, como uno más del grupo, parafacilitar la confianza y establecer unacomunicación de igual a igual.
Explicar que se va a empezar la reunióncon un pequeño ejercicio para conocersemejor: Punto en el cual se pasa al ejerciciorompehielo.
Paso #3. Creando un ambiente fraterno: Elejercicio de rompehielo
Hay varias técnicas de animación cuyo objetivocentral es crear un ambiente fraterno yparticipativo. Una técnica rompehielo es aquellaque sirve para que los participantes y el equipofacilitador se conozcan y empezar así a crearun ambiente amistoso y relajado para laconversación. Teniendo en cuenta las carac-terísticas de los participantes y el contexto, sedebe elegir para los encuentros una técnica:6
5 Notar que utilizamos las palabras “película cortita ó video”en lugar de “videoclip” y “representación” en lugar de“dramatización.” Es necesario simplificar el lenguaje yevitar palabras nuevas o complicadas con las que losparticipantes no están familiarizados.
6 Una referencia útil para la selección de técnica participativay de rompe hielo es el libro editado por el Centro de Estudiosy Publicaciones Alforja titulado “Técnicas Participativaspara la Educación Popular” (Tomos I y II, San José, CostaRica: Centro de Estudios y Publicaciones Alforja, 1988).
20
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Que sea activa.Que permita relajar a los/lasasistentes.Que involucre la participación de losparticipantes.Que tenga presente el humor.
Paso #4. Presentando historias de vida: Losvideos 1 y 2
Los videos presentan a los participanteshistorias de vida muy cortas, “historias de lavida real” que reflejan lo que sucede en lacomunidad. Describamos a continuación losobjetivos, contenidos, de los videos y la guía depreguntas utilizada para generar diálogo ydebate, en el propósito de aprender e indagarjunto con la comunidad cómo se actúa frente aun caso de emergencia de una madre gestantey qué se piensa sobre la calidad de los serviciosofrecidos en los establecimientos de salud anteuna emergencia materna.
Video #1: Relato de una madre en emergencia situadaen la comunidad
Objetivos:
Explorar qué hace generalmente lacomunidad en casos de emergencias duranteo inmediatamente después del parto.Conocer cuáles son las costumbres y lastradiciones en lo que respecta el cuidado
materno y del recién nacido.Indagar qué es lo que puede estarimpidiendo el traslado de la mujer al serviciode salud correspondiente.Indagar qué es lo que puede facilitar eltraslado de la mujer al servicio de saludcorrespondiente.
Resumen del Contenido:
Mujer enferma en casa, la persona que está conella le explica a otra los síntomas que tiene lamujer, pero ninguna de ellas sabe que se tratade señales de peligro. La comadrona llega y ledice que en ese caso ella ya no puede hacer algopor la paciente. Al mismo tiempo llega unprofesional (o proveedor) de la salud que insisteen que lleven a la mujer al servicio de saludmás cercano. El marido no está y la suegra noquiere que se lleven a la mujer al servicio desalud. Empieza una discusión acalorada entrelos que están alrededor de la mujer sobre quédeben hacer. Ésta se ve cada vez más débil, vadesfalleciendo. Se corta la filmación.
Proyección del Video 1:
El facilitador explica a los participantes que seles presentará una película7 para después
7 Se usa la palabra “película o video” en lugar de “videoclip”que es una palabra con la cual los participantesprobablemente no están familiarizados.
21
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
discutir lo que vieron. Durante el video, elequipo facilitador verifica si los participantessiguen con atención el mismo. En zonas ruralesalejadas, puede ser que la gente no estáacostumbrada a ver televisión y que en unprimer momento no presten suficiente atenciónal contenido sino más bien a la forma. Esrecomendable, pasar el video una segunda vezpara asegurarse de que todos han lo vieron yentendieron de principio a fin. Se debe tambiénpreguntar a los participantes si quieren ver lapelícula una segunda vez.
Dialogo y Debate8:
Luego de ver el video se procede a trabajar engrupo con la siguiente guía de preguntas:
1. ¿Qué les recuerda lo que acaban de ver? ¿hanvivido algo igual? ¿han escuchado de un casocomo éste en su comunidad?
2. ¿Qué es lo que sucede en la película? ¿quéproblema tiene la mujer que se siente mal?¿quiénes discuten? ¿por qué estándiscutiendo?
3. En casos como éste, ¿qué hace la gente de la
comunidad? ¿qué se hace con la mujer?4. (Si es necesario, retomar el hilo de la historia
para que los participantes se acuerden).Según ustedes, ¿qué pasaría después? ¿enqué momento y cómo se da cuenta la familiade que la mujer está grave? ¿quiénes decidenlo que se va hacer? ¿qué hacen? (aceptar quese va a morir, llamar a un curandero, llevarlaa un servicio de salud: de religiosos,institucional, prestadoras). ¿Qué pasa con laenferma al final (muere, sobrevive)?
5. ¿Qué problemas tienen que pasar para tratarde salvar la vida de esta señora? ¿quénecesitan para resolver esos problemas?¿quién los ayuda? ¿quién no los ayuda? (adistintos niveles: familia, comunidad, redesfuera de la comunidad) ¿qué tan difícilresulta resolver estos problemas?
6. Si estuvieran ustedes en esa situación, ¿quéharían?
7. ¿Qué sucede cuando una mujer muere en lacomunidad? ¿Con quién se quedan los niños?¿Quién se ocupa de ellos? ¿Qué pasa con elesposo?
Video #2: Relato de una madre gestante que llega deemergencia al servicio de salud
Objetivos:
Explorar qué es lo que le gusta y disgusta(atributos de calidad) a la comunidad sobrelos servicios y cómo les gustaría que fueran.
8 La guía de preguntas para el momento de diálogo ydebate después del ver el video, se encuentra en elAnexo #1.
22
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Indagar qué es lo que impide el uso de losservicios.Indagar qué puede facilitar el uso de losservicios.
Contenido:
Llegan al servicio de salud y un proveedor deservicios los recibe diciendo ¿por qué hanesperado tanto? y se muestra molesto con lafamilia y con la comadrona. Llega el médico deturno (joven) que no habla el idioma y explica,con buena voluntad, lo que la paciente tiene.El intérprete tiene dificultad para traducirporque el médico utiliza términos técnicos queno existen en el idioma del lugar. El médicobusca el instrumental que necesita paraintervenir y todos alrededor se empiezan amovilizar, y la filmación se corta.
Proyección del video II:
El facilitador explica a los participantes que sepresentará una segunda película para despuésdiscutir lo que vieron.
Diálogo y Debate9:
1. ¿Qué es lo que vieron en la película? ¿Quéestá pasando?
2. ¿Les ha pasado a ustedes o a alguien queconozcan algo parecido? ¿qué fue lo queles sucedió?
3. ¿Qué es lo que más les llama la atenciónde esta segunda película? ¿qué otras cosasven? ¿es así en los servicios que ustedesconocen?
4. (Si es necesario, retomar el hilo de lahistoria para que los participantes seacuerden). ¿Se acuerdan que lesmostramos sólo una parte de la película?¿Qué creen ustedes que pasó al inicio (enla parte de la película que no les hemosmostrado: cuando la familia llega alservicio de salud)?
(Si el tema no fue abordado en el videoanterior) ¿cómo hizo la familia parallegar al servicio de salud?¿Cómo recibieron a la familia en elservicio de salud? ¿Cómo piensanustedes que el personal de salud tratóa la familia, a la señora, a lacomadrona? ¿Les dejaron hacerpreguntas? ¿Cómo les contestaron?¿Qué le dijo el personal de salud a lacomadrona?
5. Y en el pedazo de película que vimos,¿Cómo piensan ustedes que se siente laseñora y la familia en el lugar donde laestán atendiendo? ¿Qué les parece el lugardonde atienden a la señora? ¿Cómo venese lugar? ¿Qué es lo que hay y qué es lo
9 La guía de preguntas para el momento de diálogo y debatedespués de ver el video 2, se encuentra en el Anexo #1.
23
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
que falta en el servicio de salud? ¿Qué eslo que les gusta y qué es lo que no lesgusta?
6. Si estuvieran ustedes en esa situación,¿qué harían?
7. Al final de la película (que tampoco hemosvisto porque la cortamos antes) ¿qué creenustedes que pasa con la señora? (¿laseñora sobrevive o muere?)
8. ¿Cuál sería un final feliz para estasegunda película? Para llegar a ese finalfeliz, ¿qué se necesitaría?
9. ¿Cómo les gustaría que los trataran en losservicios de salud?
Paso #5. Priorizando los atributos de calidad queel servicio de salud debe practicar desde laperspectiva de la comunidad
Durante el momento de diálogo y debategenerado a partir del video 2, se indaga sobrelos atributos de calidad y de satisfacción acercadel servicio de salud desde la perspectiva delos participantes. El objetivo del presenteejercicio es justamente priorizar en orden deimportancia, los atributos o características queun buen servicio de salud debe practicar y/omostrar. Por ejemplo, los participantes puedenhaber mencionado en el paso anterior que noles gusta que los traten mal o que les griten,cuando llegan con la mujer enferma al hospital,
pero que aprecian que el médico que atiende ala mujer la cure: qué es más importante paralos participantes, ¿el trato que se da a laspersonas que llegan con la mujer al hospital ola competencia técnica del médico que laatienda?
Procedimiento:
1. Se pide a los participantes que se dividanen dos o tres grupos (dependiendo delnúmero de personas). Cada grupo va arepresentar cómo le gustaría queterminara la historia que acaban de ver(video 2) desde el momento en que llegala señora a un establecimiento de saludhasta que se le salva la vida.10
2. Cada grupo presenta su dramatización. Elfacilitador le pide a los participantes quecomenten la dramatización del otro grupoy la de su propio grupo a partir depreguntas tales como:
10 Cabe mencionar que en una primera versión delinstrumento, se pedía a los participantes querepresentaran el “final feliz” de la historia que acababande ver. Nos dimos cuenta de que estos términos no tienensignificado para las personas en algunas comunidades,por lo que optamos por solicitar que representaran cómodebería concluir la historia.
24
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
¿Cómo se sintieron en el servicio desalud?¿Qué encontraron en el servicio que lesgustó?¿Cómo los trataron allí?¿Cómo se logró salvar a la mujerenferma?
3. El facilitador o el observador dibuja en elpapelógrafo imágenes de lo que la genteva diciendo. Esto lo puede hacer unmiembro del equipo facilitador que tengaaptitudes para el dibujo.11
4. Una vez que se agotaron los comentariosy que se tienen todas las imágenes en elpapelógrafo, el animador hace laspreguntas que lo ayudarán a poner loselementos mencionados en orden deprioridad:
Si tuvieran que poner en orden deimportancia todo lo que han men-cionado, ¿qué vendría primero? ¿ydespués...?El facilitador explora divergencias yconvergencias de puntos de vista y elpor qué del orden de prioridad queeligen los participantesReordena, simultáneamente, los ele-mentos siguiendo el orden de prioridadseñalado por los participantes (nume-rar los elementos en la lista delpapelógrafo).
5. Se consulta la lista final de prioridad paraasegurarse que el orden reflejado es lo queel grupo piensa.
Paso #6. Conduciendo el mapeo comunitario
El objetivo del ejercicio de mapeo comunitarioes el ubicar a personas claves y recursos en lacomunidad que pueden ayudar a las familiasen caso de una emergencia, entre ellas,miembros del poder local institucional, poderlocal tradicional, la red tradicional de salud, lared social local (por ejemplo, los vecinos,familiares). Una de las características del mapeoes que se dibuja con la participación activa delos miembros de la comunidad, la ubicación delos recursos y redes existentes para movilizarseante un caso de emergencia materna y neonatal.
11 Otra posibilidad es utilizar un flanelógrafo con imágenespreparadas de antemano. Si se decide fabricar uno, loque se puede hacer es extraer de las primeras reunioneslos elementos del discurso de los participantes que salenmás a menudo. A partir de esos elementos, se fabricaríaun flanelógrafo que podría quedar como herramienta deanimación para ésta y otras fases del trabajo con lascomunidades. También se puede optar por hacer esteejercicio con figuras, elegidas con anticipación, que sepuedan pegar sobre un papelógrafo durante la animación.
25
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Procedimiento:
1. Se pide a los participantes que se dividan endos o tres grupos (dependiendo del númerode personas). Cada grupo va a representarcómo le gustaría que terminara la primerahistoria que vimos juntos (video I) desde elmomento en que la señora se enferma hastaque se decide qué hacer. Se les explica queesta dramatización o representación tieneque mostrar cómo se puede organizar lacomunidad para tener éxito en solucionar uncaso de gravedad (emergencia): ¿Qué decidenhacer?, ¿En qué momento toman la decisión?,¿Cómo logran sacar a la mujer de su casapara salvarla?, ¿Qué los ayuda?, ¿Quiéneslos ayudan?
2. Cada grupo presenta su dramatización. Elfacilitador le pide a los participantes quecomenten la dramatización del otro grupo yla de su propio grupo. Luego el facilitadorindaga:
¿Quiénes pueden ayudar para lograr quela madre o el hijo se salven?Por ejemplo, para llevar a la mujer a unservicio de salud donde la puedan salvar¿quién puede ayudar a tomar la decisióna tiempo?¿quién puede ayudar con el transporte?¿quién puede avisar de la urgencia a losotros miembros de la comunidad y a losservicios de salud?
El facilitador dibuja en el papelógrafo figurasque representen a estos actores.12
¿Dónde están estas personas en sucomunidad? ¿cerca de la casa? ¿lejos dela casa? ¿cómo se puede hacer paraubicarlos? ¿se puede hablar con ellos?
El facilitador, con las opiniones de losparticipantes, dibuja el mapa con los recursoscon que cuenta la comunidad en el cual sepueda ubicar las personas claves que puedenayudar a las familias en caso de emergencia.Si es posible, le puede pedir a uno de losparticipantes que pase al frente paraayudarlo a hacer este pequeño mapa.Mostrando el mapa a los participantes, elfacilitador verifica que su representacióncorresponde a lo que ellos dicen y lanza lasiguiente pregunta final al grupo:
¿Qué puede hacer la comunidad paraayudar en casos de emergencia?¿Nos podremos movilizar todos juntospara salvar vidas?¿Quiénes son las personas clave en lacomunidad para los casos de emergencia?
12 Se puede pensar también en la fabricación de unflanelógrafo como en el caso anterior.
26
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
¿Cuáles son los recursos existentes en lacomunidad?
El facilitador dibuja en un papelógrafofiguras que representen a estas personasu actores identificados, así como recursosdisponibles en casos de emergencia dentrodel espacio geográfico de la comunidad..13
Una vez terminado el mapa, el animadorhace la siguiente pregunta al grupo, conla que concluirá el diálogo sobre el temacentral que nos ocupa:
¿Qué puede hacer la comunidadpara ayudar en casos de emergencia?¿Nos podremos movilizar todosjuntos para salvar vidas?
Paso #7. Finalizando el encuentro y continuandola acción colectiva
Dando seguimiento a la última pregunta hechaa los participantes, el facilitador explica que elobjetivo es justamente trabajar con lacomunidad para mejorar los servicios de salud,para ayudarlos a prevenir problemas de salud,y apoyarlos a hacer frente a casos de emergencia
para lograr así, salvar vidas. Hace al mismotiempo hincapié en que se trata de un procesoa largo plazo y que éste es sólo el inicio.Agradece al grupo por su participación y losinvita a hacer sus últimos comentarios, si tuvie-sen algo que añadir.
Luego se explica cuál será el seguimiento, esdecir, se trabajará en una “devolución” de ladiscusión conjunta de la investigación-acción ala comunidad. Se plantea que con todos loshallazgos provenientes de este proceso, se puededar continuidad a la acción colectiva conalgunas iniciativas ya forjadas en muchas otrascomunidades a través de sus autoridadeslocales y su asamblea comunitaria como es eldesarrollo de un Plan de Emergencia Comu-nitario14 y el Plan de Emergencia Familiar15
en apoyo a la vida de la madre y del niño/a.
13 Como en el ejercicio anterior de priorización, se puedepensar también en la fabricación de un flanelógrafo o enla utilización de figuras elegidas de antemano.
14 Es la expresión de la comunidad organizadasolucionando juntos un problema de salud, unaemergencia que pone en peligro la vida de una madre,niño o niña. El Plan de Emergencia Comunitario es elinstrumento que materializa el empoderamiento de lacomunidad para salvar vidas.
15 El Plan de Emergencia Familiar es el que trabaja la mujerembarazada con su esposo, en el seno de la familia paratomar decisiones anticipadas sobre qué hacer ante unaemergencia obstétrica: ¿a dónde ir?, ¿Cuánto dinero tengoahorrado?, ¿Cómo ir? ¿Quién me acompaña? ¿Quiéncuida mi casa y a mis otros hijos/as? y buscar al comitéde salud en mi comunidad para que me ayude.
27
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
3. El equipo humano facilitador de losencuentros video participativos
En esta sección especificaremos la conformación yfunciones del equipo humano encargado de llevaradelante el proceso de los “encuentros videoparticipativos”. Así mismo detallaremos algunasde las características y cualidades que el equipofacilitador debe mostrar y finalmente, aborda-remos el tema de la animación de gruposofreciendo consejos útiles para llevar adelante losencuentros video participativos. Los/as invitamosa revisar el Anexo #2, que incluye una ampliaciónde los consejos prácticos para la animación de losencuentros video-participativos presentados enésta sección.
3.1 El equipo humano facilitador
El equipo facilitador de los encuentros video-participativos está conformado por:
(a) un facilitador (o animador) quien es la personaque guía la discusión en grupo
(b) un observador participante que es la personaque toma notas durante el encuentro y apoyaal animador (o facilitador) indicándole, porejemplo:
Que hay alguien en la sala que parecetener algo que decir;
Que habría que tratar de integrar a ladiscusión a un participante que se estádurmiendo o que no participa;Que sería bueno volver a un tema, queuno de los participantes tocó en unmomento dado, para completarlo.
El observador participante está tambiénatento a la grabación de audio para verificarque se graba la reunión adecuadamente ycambiar los cassettes a tiempo.
(c) un camarógrafo (si es necesario). En algunoscasos, se necesita a alguien que se ocupe de lafilmación del encuentro en video. El compartirlas imágenes grabadas con los participantespuede constituir parte del proceso deaprendizaje con ellos y de movilización haciala elaboración de planes de emergencia.
En esta primera etapa, puede ser conveniente queel equipo facilitador de los encuentros no estéconformado por personal de salud institucional quetrabaje en la misma localidad o comunidad. Estotiene un doble propósito: (i) evitar el sesgo de“capacitadores” que el personal de salud ya tienedebido a sus funciones y que llevaría a que losparticipantes confundieran el encuentro con unasesión de capacitación; (ii) asegurarse de que lagente se sienta totalmente libre de expresar susopiniones. Una posibilidad es que el personal de
28
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
salud que trabaja en una localidad, encuentre acomunidades de otra región y no de la suya. Laotra posibilidad es que el equipo facilitador estéconformado por personas del exterior, nonecesariamente personal de salud, que tenganbuenas habilidades de animación y co-animación.En el caso en el que un profesional o proveedor desalud actúe como animador o como observadorparticipante en la comunidad en la que trabaja,es importante asegurarse de que su propiapresencia no afecte los resultados del proceso.
3.2 Las cualidades y habilidades del equipofacilitador
El equipo facilitador tendrá que realizar untrabajo minucioso, que requiere rigor y capacidadde organización, pero que es a la vez divertido.Para llevar a cabo este trabajo es importanteactualizar algunas cualidades, tales como:
Saber escucharActuar con modestiaTener aperturaTener sentido del humor
Los principios de base que guían este trabajoson:
El respeto (incluyendo el respeto a lasdiferencias)La equidadLa veracidad
Las reglas de oro a seguir son:La puntualidadEl cumplimiento (de promesas,ofrecimientos, etc.)
Hay que recordar siempre, que toma añosdesarrollar lazos de confianza con la comunidad,pero sólo segundos destruirlos. La comunidadpercibe si la relación que el equipo establececon ellos es o no auténtica y lo confirma, porejemplo, cuando se da cuenta de que el equipo:
No crea falsas expectativas en lacomunidadRespeta la confidencialidad de losparticipantes
El equipo facilitador debe ser:
Participativo y a la vez estructurado¿Qué significa esto?, significa que laparticipación no sucede de maneraespontánea sino que es el producto deun esfuerzo consciente y ordenado porcrear las condiciones necesarias paraque la gente participe.Para lograr la participación hay que:
Ser estructurado y organizadoRespetar los tiemposdisponibles para los encuentrosSer lo suficientemente flexiblecomo para adaptarse a lascircunstancias y al medio
29
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Ser creativo para encontrar lamejor manera de adecuarse almedio sin perder de vista losobjetivos fijadosSer disciplinado paradocumentar sistemáticamentelos hallazgos de los encuentros ypoder así retornarlos a lacomunidad y transmitirlos atomadores de decisión demanera confiable.
Finalmente, es importante que el equipofacilitador:
sepa desarrollar empatía con lacomunidad al mismo tiempo queestablece una distancia objetiva que lepermita documentar las cosas tal comoson.
En la medida que el equipo esté consciente desu propia subjetividad, de sus valores ycreencias, podrá lograr la objetividad necesariapara llevar a cabo el trabajo aquí propuesto.
3.3 Consejos prácticos para la animación de grupos
El facilitador actúa durante los encuentros a lavez como un “periodista” que:
está “en el centro de la acción”está buscando la opinión de “expertos”
que son los miembros de la comunidadquiere conocer la verdad
Como un “antropólogo”:que aprende con la comunidadlisto siempre a descubrir nuevas cosas
Y es, al mismo tiempo, un “artesano”:que trabaja con minuciosidad yque es paciente y perseverante
4. Los participantes de la comunidadinvitados a los encuentros videoparticipativos
Los participantes de los encuentros video-participativos son seleccionados a partir de criteriosprecisos y dentro de un proceso de selección queincluya a toda la comunidad.
4.1 El proceso de invitación de los participantes
Los agentes externos, en este caso el equipofacilitador, pasa a menudo por las autoridadeslocales formales para realizar las convocatorias enlas comunidades. Es importante que estaspersonas clave, que van a hacer la convocatoria,tengan una copia de la lista de criterios para laselección de participantes de cada encuentro. Peromás allá de estos criterios, es esencial dejar enclaro que se quiere invitar a los encuentros a
30
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
miembros de los grupos más vulnerables dentrode la comunidad.
Toda comunidad o sociedad es un universocomplejo, en el que existen distintos estratossociales. Teniendo en cuenta las limitaciones queel medio puede imponer, es importante tratar depromover la participación de aquellos que puedenestar siendo dejados de lado debido a que:
Se considera que no están interesadoso no son capaces de participar.Constituyen grupos marginales (porejemplo, son los más pobres) dentro dela comunidad.No forman parte del grupo de electoresde las autoridades vigentes.
La práctica nos ha enseñado que una convocatoriarestringida y sesgada puede causar resentimientoy desconfianza en la comunidad. Al mismo tiempo,la presencia de agentes externos, que aportan unpunto de vista desde fuera de la comunidad, puedea veces contribuir a la inclusión de grupostradicionalmente rezagados y abrir espacios dediálogo en los que estos grupos, particularmentevulnerables, puedan participar.
4.2 Los criterios de selección de los participantes
En el caso que nos ocupa, identificamos por lomenos cuatro grupos de personas que nos interesa
encontrar en grupos separados, ya que cada unode ellos puede aportar una perspectiva diferentesobre la salud materna y neonatal y el manejo decasos de emergencia en la comunidad. Se trata de:las mujeres, las comadronas, los líderes y loshombres. Es importante que cada grupo seahomogéneo para facilitar los intercambios entre losparticipantes. Por ejemplo, si invitamos a unacomadrona que es líder tradicional en sucomunidad a participar dentro a un encuentro conmadres de familia, encontraremos que su discursoes diferente al de estas últimas, hablaráprobablemente más que las otras mujeres, einfluirá tal vez sobre sus opiniones. De ahí laimportancia de encontrar a estos gruposseparadamente.
Los criterios para la selección de los participantesson, en cada caso:
GRUPO DE MUJERES
Que estén embarazadas o hayan sidomadres (pueden haber perdido hijos).Puede que se quieran incluir tambiénmujeres en pareja y en edad reproductiva,que todavía no han tenido un embarazo.Es importante incluir futuras madresjóvenes y mujeres con alta paridad.Usuarias y no usuarias de los servicios.Que hablen el idioma del lugar.
31
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
GRUPO DE COMADRONAS
Con distintos niveles de experiencia comocomadronas.Con y sin capacitación (de parte de losservicios formales).Que hablen el idioma del lugar.
GRUPO DE LÍDERES
Líderes institucionales (alcalde auxiliar,presidente de comité de iglesia, pastorevangélico, comité de escuela, etc.) ylíderes tradicionales (comadrona,sacerdote maya, curandero).Hombres y mujeres (equilibrio de género),pero tomando en cuenta la composiciónreal de la comunidad.Diversidad en cuanto a tipo de líderes(religiosos, políticos, etc.).Que hablen el idioma local.Invitar a comadronas con muchainfluencia a participar en los encuentrosde líderes (ya que podrían dirigir ladiscusión en los grupos de comadronascon menos influencia).
GRUPOS DE HOMBRES
Esposos o convivientes. Pueden o no serlas parejas de las participantes en el grupode mujeres.
Usuarios y no usuarios de los servicios.Que hablen el idioma del lugar.
Sobre los criterios de selección:La edad noes considerada un criterio de selección enningún caso. Especialmente en el grupo demujeres, el más alto índice de mortalidad seda al inicio de la vida reproductiva y, por lotanto, es importante incluir también afuturas madres jóvenes. Por otro lado, esimportante también invitar a participar amujeres de alta paridad, que constituyentambién un grupo de riesgo.
5. La organización previa y la logística
La realización de encuentros en comunidadesremotas del país requiere un esfuerzo deorganización y de coordinación considerable. Lapuerta de entrada a la comunidad, como loacabamos de mencionar, son las autoridadeslocales formales. Una visita previa a la comunidadelegida para el trabajo permitirá a los miembrosdel equipo facilitador hacer un primer contacto conellos y verificar el interés y la factibilidad derealizar los encuentros en la localidad en cuestión.Una vez confirmada la posibilidad de llevarlos acabo en una comunidad dada, se debe proceder aplanificar cuidadosamente la visita, previendo los
32
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
recursos humanos y materiales necesarios paralos encuentros.
5.1 Gestión de recursos
Es recomendable utilizar cuadros de verificacióncon la finalidad de prever los recursos humanos ymateriales necesarios para cada encuentro. Lapreparación con anticipación de otros documentos,como la ficha de datos socio-demográficos paracada encuentro o las guías de diálogo y debatetraducidas al idioma local, contribuirá igualmenteal buen desarrollo de las actividades.
Cuadro de recursos humanosPreparar un cuadro en el que se puedanindicar los nombres de los miembros del equipofacilitador para cada localidad. Dicho cuadroservirá para verificar si se cuenta con el equipohumano necesario en las fechas previstas ypara cada encuentro. Proporcionamos unejemplo de Cuadro de recursos humanos enel Anexo #3
Cuadro de recursos materialesPreparar un cuadro con la lista de materialese insumos que se necesitan para el encuentroy usarlo como lista de verificación antes desalir al campo. Proporcionamos un ejemplode Lista de verificación de materiales einsumos en el Anexo #4.
La ficha de datos socio-demográficosNo olvidar preparar, para cada reunión, unaficha en la que se vaciarán los datos socio-demográficos (más pertinentes) de losparticipantes. Proporcionamos ejemplos deFichas de datos socio-demográficos en losAnexos #5(A) y #5(B).
La traducción del instrumentoEl instrumento debe ser traducido pre-feriblemente con anticipación para usodurante los encuentros que se lleven a caboen otro idioma que no sea el castellano. Estatraducción debe respetar la formulación y elorden de las preguntas del instrumentooriginal.
Es importante no fiarse para la traducción nide la memoria del facilitador ni de sucapacidad de hacer traducciones simultáneas.No hay que olvidar que el trabajo de traduccióne interpretación simultánea requiere unaformación y experiencia específicas con la cualla mayoría de los animadores no cuentan.
Las transcripciones de los encuentrosDesde antes de salir al campo, el equipo debeempezar a preparar el trabajo de transcrip-ción. Hay que ubicar y contactar a las personasque se ocuparán de las transcripciones con
33
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
tiempo, para estar seguros de realizarlas a labrevedad posible. Estas personas debenhablar los idiomas en los que se lleve a cabolos encuentros, tener una buena velocidad deescritura y, si es posible, experiencia en estetipo de trabajo.
Se les debe entregar una hoja escrita coninstrucciones precisas acerca de cómo hacer latranscripción. (Esto aparece en el Anexo 7).
Algunas instrucciones para lastranscripciones
Indicar quién habla en cada caso.Traducir lo que la persona dice talcomo lo dice.No hacer resúmenes, ni sintetizar loque la persona dice.Cuando resulte difícil o imposibletraducir palabras al castellano(porque no existen en nuestrovocabulario), escribirlas en la lengualocal y explicar entre paréntesis loque significan.Cuando la traducción literal de lapalabra ilustra maneras de pensar ode ver el mundo, ceñirse a latraducción “literal” y explicar entre
paréntesis lo que la palabra significaen el contexto (por ejemplo, si lapersona usa el término “suciedad”para referirse a la menstruación,escribir “suciedad” y explicar entreparéntesis lo que significa).
El formato que la persona utilice para vaciarla información, dependerá del uso que sequiera hacer de la transcripción. Así, si seha grabado la reunión en video y se quieredespués editar lo filmado, se le proporcionaráun formato en el que se puedan plasmartanto las imágenes como el texto. Si se piensautilizar la transcripción para un análisis deldiscurso (verbal) de los participantes, bastarácon transcribir las intervenciones orales delos participantes.16
5.2 Gestión del tiempo
La gestión del tiempo es importante a distintosniveles: antes, durante y después de los encuen-tros.
16 En algunos casos, en los que se opta por analizar lainformación con la asistencia de programascomputarizados, se deben dar instrucciones precisas paraque el formato de las transcripciones resulte compatiblecon el programa.
34
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Antes:
Planificar los encuentros conanticipación y, en la medida de loposible, hacer un recordatorio oconfirmación, uno o dos días antes dela fecha fijada en coordinación con elpersonal de salud o autoridadeslocales.
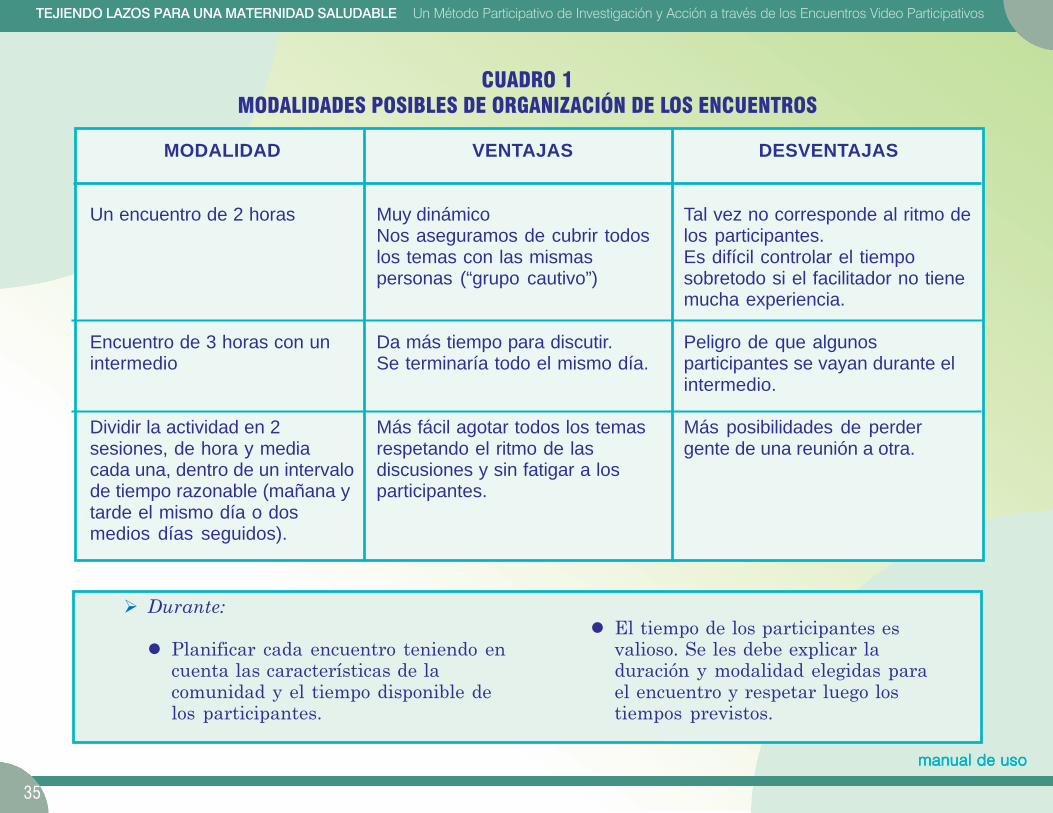
En consulta con personas clave queconozcan bien la comunidad,incluyendo el personal de salud quetrabaja en la zona, se elige lamodalidad de organización queconviene en cada caso. El cuadro 1resume tres modalidades deorganización entre las que el equipofacilitador podrá elegir. Es importanteque una vez elegida la modalidadmás apropiada, se prevean losrecursos y el tiempo específicosrequeridos en cada caso.
Llegar a la localidad con suficienteanticipación como para que el equipopueda reunirse y afinar los últimosdetalles de cada encuentro.
Planificar con anticipación el trabajode transcripción de los encuentros,teniendo en cuenta que se necesitanaproximadamente 8 horas paratranscribir una hora de grabación deaudio.
Anticipar las actividades deseguimiento y los “productos” apresentar como resultado del procesoy preparar un cronograma globaldetallado de trabajo, teniendo encuenta estos aspectos.
35
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
VENTAJAS
Muy dinámicoNos aseguramos de cubrir todoslos temas con las mismaspersonas (“grupo cautivo”)
Da más tiempo para discutir.Se terminaría todo el mismo día.
Más fácil agotar todos los temasrespetando el ritmo de lasdiscusiones y sin fatigar a losparticipantes.
MODALIDAD
Un encuentro de 2 horas
Encuentro de 3 horas con unintermedio
Dividir la actividad en 2sesiones, de hora y mediacada una, dentro de un intervalode tiempo razonable (mañana ytarde el mismo día o dosmedios días seguidos).
DESVENTAJAS
Tal vez no corresponde al ritmo delos participantes.Es difícil controlar el tiemposobretodo si el facilitador no tienemucha experiencia.
Peligro de que algunosparticipantes se vayan durante elintermedio.
Más posibilidades de perdergente de una reunión a otra.
CUADRO 1MODALIDADES POSIBLES DE ORGANIZACIÓN DE LOS ENCUENTROS
Durante:
Planificar cada encuentro teniendo encuenta las características de lacomunidad y el tiempo disponible delos participantes.
El tiempo de los participantes esvalioso. Se les debe explicar laduración y modalidad elegidas parael encuentro y respetar luego lostiempos previstos.
36
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Después:
Planificar con anticipación las tareasde compilación y análisis de lainformación para poder, dentro de untiempo razonable, devolver lainformación a los interesados: lacomunidad misma y los tomadores dedecisiones.
5.3 Gestión del espacio
Hay que tomar en cuenta también, durante laorganización de los encuentros, aspectosrelacionados al espacio físico en el que setrabajará, como por ejemplo los referidos a:
Electricidad. Verificar si hay electricidaden la comunidad. Si no hubieseelectricidad ubicar un generador eléctricoen la localidad para ser prestado. Si nofuera posible, contactar a un grupo depersonas voluntarias dispuesta a hacer ladramatización o sociodrama en cada unode los encuentros.Local del encuentro. La ubicación dedónde se llevarán a cabo los encuentroses crítica para asegurar disponibilidad.Las características del local a tener encuenta:
Referirse al cronograma de trabajo yrespetar las fechas límitesestipuladas. Si esto no fuera posible,y se requiriera hacer algunamodificación al cronograma inicial,comunicar los cambios a las personasinvolucradas (es decir, a aquellos queesperan resultados del equipo).
Que sea lo suficiente espacioso comopara albergar al grupo y, si es posible,no tan grande que provoque eco o ladispersión de los participantes.Que no esté cerca de un puesto deventa o de un ambiente en el que hayamucha bulla. Esto distrae durante lasdiscusiones y dificulta la grabación.La disposición física de las sillas obancas para los participantes estambién importante: Formar un semi-círculo o círculo que incluya al equipofacilitador.La cercanía de los participantes entresí dará una atmósfera más íntima quefavorecerá la conversación y facilitaráal mismo tiempo la grabación.
Posición del equipo facilitador respecto alos participantes. Evitar que la disposición
37
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
del equipo facilitador al frente de laaudiencia, como si se tratara de un cursomagistral. Esta disposición da la impresiónque los unos (que están al frente) “saben”(vienen a enseñar) y los otros (los queescuchan) “no saben” (y vienen a recibir).Por el contrario, lo que se quiere promoveren este caso es el intercambio igualitarioentre el equipo facilitador y losparticipantes.Prever hospedaje para equipo facilitador.Si es necesario que el equipo se quedevarios días en la comunidad, se debeprever un lugar donde puedan dormir.Como veremos más adelante, la visita oestadía en la comunidad constituye en síuna oportunidad de estrechar lazos con lacomunidad y de encontrar informalmentea personas que no participaron en losencuentros.
6. Información recopilada
No basta recoger la información e intercambiar conla comunidad. Si se quiere utilizar la informaciónpara alimentar un proceso de cambio en lacomunidad, es preciso procesarla y analizarla paradevolverla a la comunidad, para que ésta puedaasí compartirla con tomadores de decisiones. Sehace necesario pues, por un lado, ir sistematizando
la experiencia, y por el otro, llevar a cabo un aná-lisis de lo conversado en busca de propuestas útilesque salgan de los participantes mismos y en lasque ellos se vean reflejados.
6.1 La sistematización de la experiencia
La sistematización constituye en sí un temametodológico aparte, que no pretendemos cubriren este manual. Sugerimos aquí simplemente unpar de herramientas de base que pueden servirpara la sistematización de la experiencia por elequipo facilitador y la comunidad. Se trata dedesarrollar herramientas para el registro de losmomentos, hechos, acciones más sobresalientes yconstruir así una memoria viva del proceso con lacomunidad.
Documento de reflexión y autorreflexión sedebe llenar luego de cada encuentro, enel cual se mencionen los puntossobresalientes (barreras, facilitadores,hallazgos, sorpresas) en cuanto a:
PreparaciónConvocatoriaOrganización / logísticaFacilitación e instrumentoContenido de las discusionesEl proceso con la comunidad
38
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Diario de ruta en el cual se puedan docu-mentar las entrevistas formales einformales y las observaciones del equipofacilitador durante sus estadías o visitasa la comunidad:
FechaDescripciónElementos sobresalientesSeguimiento previstoGlosario de la terminología de lacomunidad
Cuadros para la compilación yorganización de datos con respecto a:
Los recursos identificados en lascomunidades, tales como los mediosde comunicación tradicionales ytécnicos comúnmente utilizados,principales canales y fuentes deinformación y comunicación formale informal, personas y grupos clave,redes existentes, etc. Estos datosservirán para el desarrollo deestrategias de participación social yde IEC (información, educación ycomunicación), así como a laformación o consolidación de redesde apoyo a la vida.
Reuniones de sistematización periódicasplanificadas de antemano para:
El intercambio y socialización conla comunidad y con el personal desalud que trabaja a distintosniveles.Estas reuniones no sonespontáneas ni casuales. Ellasdeben ser organizadas conanticipación siguiendo una agendaprecisa y un diseño metodológicoparticipativo coherente con eltrabajo de investigación-acción.
6.2 El análisis de los encuentros
El análisis de datos es un tema complejo que vamás allá de los límites de este manual. Cabemencionar aquí simplemente que el análisis condetalle de los encuentros permitirá una mejorcomprensión de las dinámicas psico-sociales ysocio-culturales que influencian las maneras dehacer y de ser en una comunidad. Estacomprensión permitirá a su vez el desarrollo deestrategias adecuadas al contexto así como laidentificación y previsión de problemas potencialesque se puedan encontrar en las comunidades enlo que respecta a la salud materna y del reciénnacido. Más allá de su utilidad desde el punto devista de agentes externos deseosos de mejorar su
39
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
trabajo con la comunidad, el análisis de datos eneste contexto parte del punto de vista de lacomunidad y busca retornar los resultados demanera de reforzar el proceso de empoderamientocomunitario.
Para llevar a cabo este tipo de análisis se debentener en cuenta ciertas etapas que requierenplanificación y organización, tales como:
La preparación de las transcripciones.El ordenamiento de datos en matrices.El análisis de la información.La socialización de los resultados.
Es recomendable contar con el apoyo deespecialistas en análisis cualitativo para realizarconjuntamente este trabajo. La contribución de losinvolucrados—tanto del equipo facilitador como delos participantes de la comunidad—durante la fasede análisis es esencial. El proceso de retorno a lacomunidad se convierte a menudo en unaoportunidad de validar y afinar los resultados delanálisis.
7. El uso del instrumento dentro de unproceso
El instrumento de investigación-acción queproponemos es una herramienta de aprendizajeque se sitúa dentro de un contexto que va más
allá de los encuentros video-participativos. Esesencial no perder de vista que, más allá de la“recolección de información,” se inicia un procesocon la comunidad, de cuyo éxito dependerán lassiguientes fases del trabajo con ella. Durante lasvisitas a las comunidades hay una serie de tareasparalelas a realizar, que se complementan yrefuerzan entre sí:
Conducir los encuentros video-parti-cipativos con los diversos gruposCrear y desarrollar los contactos conorganizaciones de base, comités,organizaciones no gubernamentales, etc.activos en la comunidad.Elaborar estrategia de cómo estos gruposformados para los encuentros y laspersonas y grupos clave contactados en lacomunidad, pueden mantenerse involu-crados a lo largo del proyecto para seguirel trabajo.Proseguir, fuera de los encuentros, con el“mapeo comunitario” visitando lo queexiste.Aprovechar también para conversar conel resto de los miembros de la comunidady no sólo con aquéllos que han participadoen los encuentros.
Estas conversaciones girarán en torno,en un primer momento, a temas más
40
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
bien generales que nos darán una ideade la realidad y la trayectoria de lacomunidad, como por ejemplo: cómo seformó la comunidad, cómo es la vida enla comunidad, si hay muchos niños,cuáles son las fiestas, cómo las celebran,dónde está la escuela, dónde está laparroquia, quiénes son las autoridades(tradicionales y formales), dónde sereúne la gente, si la gente de losalrededores se conoce bien, cuáles sonlos principales problemas en la comu-nidad, si se ayudan entre ellos, etc.
Poco a poco, y en un segundo momento,podrán entrar al tema de: ¿qué hacencuando alguien se enferma?, ¿hastadónde tienen que ir para hacerse ver osi alguien viene a sus casas?; ¿si sabende alguna señora que haya tenidoproblemas con su embarazo o en el
momento de dar a luz?; ¿qué es lo quela gente hace en esos casos: dónde van?,¿a quién consultan?; ¿si acuden a losservicios?: ¿cuándo van?, ¿dónde?, ¿quéles parecen?, ¿qué tipo de cuidadoprefieren?; ¿si conocen gente u orga-nizaciones (redes formales e informales)que son importantes en la comunidady que deberíamos contactar?; etc.17
Fortalecer los lazos con la comunidad apartir, por ejemplo, de la participación(bajo invitación) a reuniones comuni-tarias.
Es fundamental en esta etapa establecer y / oconsolidar el trabajo en redes y desarrollar lazosde confianza y colaboración con los miembros dela comunidad. El éxito de la iniciativa podrámedirse en función de la continuidad y elfortalecimiento de estos lazos a lo largo del tiempo.
17 Toda esta información debe ser documentada usandolas herramientas para la sistematización de la experienciapropuestas más arriba.
41
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
No basta con tener una excelente materia prima yun instrumento adecuado para tejer los lazos. Esnecesario asegurarse de la calidad y de lacontinuidad de los lazos que se vayan tejiendo conla comunidad. Para hacerlo, lo más importante espropiciar el diálogo y la participación. El diálogo yla participación son, en efecto, los principalesingredientes a lo largo del proceso de creación delazos dentro de esta investigación-acción. Ellosatraviesan el trabajo de principio a fin. En estaparte ofreceremos pautas para dos aspectos de laparticipación que pueden presentar interrogantesprácticas durante el trabajo: la cuestión de losincentivos y el retorno de la información recogidaa la comunidad. Terminaremos con una reflexiónsobre el diálogo y la participación como procesos ycomo resultados que se quieren potencializar enla comunidad a través de la metodología de trabajoque proponemos.
1. Valoración e incentivos
A menudo, los miembros de la comunidad estáninteresados en participar. Están dispuestos no sólo
a participar en discusiones en grupo donde puedenexpresar sus opiniones sino, además, a realizarvoluntariamente algunas tareas específicas. Porejemplo, hay miembros de la comunidad que seprestan gustosos a hacer las dramatizaciones, locual nos permite reemplazar las imágenes de losvideos con imágenes “en vivo” cuando no hayenergía eléctrica en la comunidad. Otros sirvende intérpretes cuando hay personas de fuera queno entienden el idioma local en que se lleva a caboel encuentro.
La retribución a las personas que colaboran yparticipan a distintos niveles se presta al debate.Hay quienes consideran que es importante quelos miembros de la comunidad se involucrenvoluntariamente, sin esperar una compensaciónmaterial e inmediata a cambio. Hay tambiénquienes consideran que es importante retribuir alas personas, ya que es una forma de reconocersus esfuerzos y el tiempo que dedican a unaactividad. Entre las dos posturas, ¿cuál nosconviene adoptar? Una posición intermedia seríala que:
PARTE III:LOS LAZOS
42
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Reconoce e incentiva la participación de lacomunidad yEvita, al mismo tiempo, dar la impresión deque se está “remunerando” a los que parti-cipan
Una manera de hacerlo es encontrar con lacomunidad un “símbolo” que a la vez:
Tome la forma de un objeto que se puedadistribuir como incentivo durante lasactividades, ySirva para reforzar el trabajo en saludmaterna y neonatal, sin dar la impresión quees una “remuneración” o compensaciónmaterial
El “listón blanco” es un ejemplo de “símbolo” quees a la vez un objeto que puede distribuirse a losparticipantes. Los listones se utilizan a nivelmundial para simbolizar distintas causas.18 Ellistón blanco representa, entre otros, la luchacontra la violencia hacia las mujeres; el rojorepresenta el apoyo al trabajo de educación sobreel sida; el amarillo representa el apoyo al trabajode defensa de los derechos humanos. Se podríapensar en introducir en las comunidades un listón,
u otro elemento elegido con la comunidad, comomedio de reconocimiento y como símbolo de loslazos para la mejora de la salud materna y delrecién nacido. Lo ideal sería que este objetosimbólico fuera pensado y fabricado con lacomunidad, adaptándolo a la cultura local. En estecaso, ese objeto representaría o sería un “símbolo”del trabajo a favor de la salud materna y del reciénnacido. A partir de este objeto podría desarrollarsetodo un sistema de incentivos con la finalidad dereforzar la participación de los miembros de lacomunidad a distintos niveles.
2. El retorno a la comunidad
El retorno de la información recogida durante losencuentros video-participativos es un aspectoesencial del proceso de investigación-acción ya quea través de él se va reforzando el proceso de diálogocon la comunidad y se va propiciando que lacomunidad misma tome un papel cada vez másactivo en la búsqueda de soluciones a losproblemas que la aquejan. Este retorno deinformación debería convertirse no en una“presentación de resultados” sino en un espaciode intercambio con la comunidad.
Al mismo tiempo que se devuelve a la comunidadlo que sus miembros opinan sobre el manejo delos casos de emergencia o la utilización de losservicios, se verifica con ellos si la información
18 En el sito www.sltrib.com se da información sobre loslistones de distintos colores y las causas que representana nivel mundial o en distintos países del mundo.
43
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
parece exacta y si hay otras opiniones que noaparecen y que deberían añadirse. Si no se haempezado todavía a trabajar con la comunidad enel desarrollo de planes locales de apoyo a la vida,esta reunión de intercambio puede ser unmomento adecuado para iniciar este trabajo. Estosplanes adoptarán un nombre diferente según loque decida la comunidad.
Dado que se trata de un espacio de intercambio,esta reunión con la comunidad debe organizarsede tal manera que facilite la presencia de los queparticiparon en los encuentros, así como de los queno tuvieron la oportunidad de participar en ellos.Esta reunión tomará probablemente la forma deuna asamblea comunal durante la cual semotivará a los asistentes a participar activamente.El personal de salud que trabaja de cerca con lacomunidad debe también ser invitado a la reunióny, si es posible, co-animar la reunión. Podría pueshaber uno o dos facilitadores durante la reuniónque se compartirían las tareas durante la discusiónen grupo. El o los facilitadores de la reunióndeberán utilizar técnicas participativas, así comodibujos, figuras e imágenes para lograr unintercambio dinámico con los participantes.
Los temas de la reunión podrían ser priorizadosteniendo en cuenta los intereses salientes de lacomunidad. Para facilitar la participación durantela reunión, los facilitadores pueden seguir los
consejos para la animación que se ofrecen en elAnexo #2 y asegurarse de verificar:
Si lo que dicen es claro y comprensiblepara los participantes¿Qué opinan los participantes sobre loque dicen?
Si hay algo que añadirSi hay algo que corregir
¿Qué les parece a los participantes laspropuestas hechas (de trabajo conjunto,por ejemplo)?¿Qué sugerencias tienen losparticipantes?
Es importante planificar cuidadosamente estareunión tanto a nivel de contenido como en lo quese refiere a la previsión de los recursos humanosy materiales necesarios para llevarla a cabo. Paraordenar lo que se discuta sobre el Seguimiento ala Reunión con la Comunidad es recomendableutilizar un cuadro que los facilitadores debenllenar con la ayuda de los participantes. Se debeprever para ello ya sea un pizarrón, marcadores ypapel de rotafolio, para que los facilitadorespuedan tomar nota de lo que se discute en grupo.En este proceso de diálogo con la comunidad, losfacilitadores no imponen un programa, sino quenegocian la mejor manera de incluir en la agendalocal la prevención de muertes maternas y derecién nacidos como una de las prioridades en la
44
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
comunidad. Esta es una oportunidad de estrecharlos lazos entre la comunidad y el personal de saludy de establecer las bases para un trabajo querequiere un compromiso a largo plazo de las dospartes.
3. Tejiendo lazos
Como señalamos al principio del manual, los lazosno son sólo producto sino también proceso. Loslazos se forman en diálogo con los miembros de lacomunidad, dentro de un proceso de participaciónque incluye a los grupos más vulnerables. Se debebuscar la participación de la comunidad a distintosniveles y en diferentes momentos dentro y fuerade las reuniones de discusión y de intercambio.Pero esta participación no se logra de maneraautomática. Lograrla requiere tiempo, esfuerzo yperseverancia. Por un lado, mucha gente no hatenido antes la oportunidad de participar y le tomatiempo darse cuenta de que puede hacerlo yaprender a hacerlo. Por otro lado, para establecerun diálogo abierto hay que desarrollar lazos deconfianza y sostenerlos a través del tiempo, cosaque no se hace de un día a otro. A veces, se tieneque empezar a desarrollar lazos de confianza encontextos en los que por motivos históricos ya haydesconfianza y resistencia hacia las propuestas quevienen de afuera o que representan instanciasgubernamentales.
La participación es:Un proceso largo y lentoUna meta a seguir, pero también unaserie de problemas para resolver
La participación:No se da de manera automáticaRequiere un “trabajo de hormiga”
A menudo la necesidad de respetar el ritmo deeste proceso a largo plazo se enfrenta con laurgencia de presentar resultados dentro decronogramas de trabajo precisos. ¿Cómo conciliarentonces los procesos y los productos? Nopretenderemos dar una respuesta absoluta a estainterrogante en el espacio limitado que nos quedadentro de este manual, ya que cada caso esdiferente y requeriría un tratamiento específico.Sin embargo, en términos generales, dentro delproceso de investigación-acción siempre hayresultados que se pueden y deben ir compartiendocon los interesados, en la medida que salen y estodentro de límites razonables de tiempo. Así, si sellevan a cabo los encuentros en una comunidad yse retornan los resultados después de un año, yano hay continuidad y el proceso se rompe. De igualmanera, hay información que puede ser útil paralos decisores y que se le debe transmitir en lamedida que se encuentra.
45
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Es necesario trabajar con fechas límite yofrecer productos útiles a los actoresinvolucrados (comunidades y tomadoresde decisiones) en la medida que vayaavanzando la iniciativa.
Pero al mismo tiempo que se ofrecenproductos útiles, tanto a la comunidadcomo a los decidores, es importante teneren cuenta que el proceso instaurado tomatiempo y requiere un “trabajo de hormiga.”El éxito de este tipo de iniciativa, se midemás en relación a la calidad de laparticipación y los beneficios a largo plazo,que en función del número de personas ocomunidades cubiertas y el impacto de lasactividades a corto plazo.
Es necesario sensibilizar a los involu-crados y a los tomadores de decisiones, enespecial a aquéllos que están máshabituados a trabajar en función deproductos concretos, sobre la naturalezay las implicaciones de un trabajoparticipativo dentro de procesos de cambioa largo plazo.
Los lazos son tanto productos comoprocesos. Es importante pues, lograr unequilibrio entre productos a corto plazo yprocesos a largo plazo.
No cabe duda de que el diálogo y la participación,como los lazos, tienen una utilidad y un propósitoque se traducen—y deben traducirse—enresultados concretos. Las comunidades mismasinsisten una y otra vez en ver estos resultados yen que su participación no sea “en vano.”19 Almismo tiempo, el valor del diálogo y laparticipación es que se trata de procesos querepresentan continuidad y que favorecen lasostenibilidad de las iniciativas a largo plazo. Es,en efecto, a través del diálogo y la participaciónque los miembros de la comunidad se apropian deiniciativas y adquieren las herramientas que lespermiten asegurar su continuidad a lo largo deltiempo.
Los lazos tienen pasado, presente y futuro. Eldiálogo y la participación, al igual que los lazos,se convierten en parte de la historia de lacomunidad ayudándola a rescatar su pasado,analizar su presente y desarrollar una visiónconjunta hacia un mejor futuro. El propósito deeste manual ha sido no sólo familiarizar al lectorcon la metodología de investigación-acción a travésde los encuentros video-participativos, sinocompartir algunas pistas de reflexión para su usoen el contexto más amplio del trabajo participativocon las comunidades.
19 De acuerdo a los resultados de los encuentros realizadosen Momostenango y en la Zona Reina.
46
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
PRESENTACIÓN DEL PROYECTO Y DEL EQUIPO
El facilitadorexplica, de forma general, el objetivo delencuentro y agradece la participación de lospresentes.explica a los participantes el carácterconfidencial y anónimo de sus intervenciones.les explica la necesidad de grabar la reuniónpara tener una “memoria” del encuentro (se lespuede ofrecer, en la medida de lo posible, el verla grabación posteriormente).20 Si es posible,pedirles su consentimiento para la grabación,reasegurándolos una vez más el anonimato yla confidencialidad.
PARTE IV. ANEXOSANEXO 1
GUIA DE DISCUSIÓN
EL INSTRUMENTO DE RECOLECCIÓN DE DATOSPARA LOS ENCUENTROS VIDEO-PARTICIPATIVOS
les explica que verán juntos un par de videoscortos preparados para la reunión y queconversarán informalmente de lo que cada unopiensa.les pide que lo interrumpan en cualquiermomento si hay algo que no esté claro.presenta a los demás miembros del equipo porsu nombre y función (durante la reunión). Sesugiere no mencionar sus cargos en el sector desalud, para evitar sesgos.les explica que van a empezar con un pequeñoejercicio para conocerse mejor.
20 Es muy importante asegurar confidencialidad y anonimato de los participantes. Para reasegurarlos de manera concreta, loideal sería que los de una región encuentren a usuarios/as de OTRA región y no de la suya. O, como hemos acordado, que lagente que facilite sea gente del exterior con buenas habilidades de animación. Tener cuidado de que el personal de salud quehaga las veces de observador participante en su propia comunidad no afecte con su propia presencia los resultados.
47
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
DINÁMICA ROMPE-HIELO:A elegir teniendo en cuenta las características delos participantes.
PARTE IPresentación del video 1, seguida de discusiónEl facilitador explica el procedimiento a losparticipantes: se les presentará una parte de unapelícula de la cual se discutirá después de verla.Observación: ver si los participantes estánsiguiendo con atención el video. Pasarlo unasegunda vez para asegurarse de que todos lo hanvisto y entendido de principio a fin.
Video 1: Situación—emergenciaDramatización: mujer enferma en casa, lapersona que está con ella le explica a otra lossíntomas que tiene la mujer, pero ninguna deellas sabe que se trata de señales de riesgo.La comadrona llega y le dice que en ese casoella ya no puede hacer nada. Al mismo tiempollega un proveedor de servicios de salud queinsiste en que lleven a la mujer al servicio desalud más cercano. El esposo no está y lasuegra no quiere que se lleven a la mujer alServicio de salud. Empieza una discusiónacalorada entre los que están alrededor de lamujer sobre qué deben hacer. Ésta se ve cadavez más débil, va desfalleciendo. Se corta lafilmación.
Video 1, preguntas para la discusión:1. ¿Qué les recuerda lo que acaban de ver? ¿han
vivido algo igual? ¿han escuchado de un casocomo éste en su comunidad?
2. ¿Qué es lo que sucede en la película? ¿quéproblema tiene la mujer que está mal?¿quiénes discuten? ¿por qué están discutiendo?
3. En casos como éste, ¿qué hace la gente de lacomunidad? ¿qué se hace con la mujer?
4. (Si es necesario, retomar el hilo de la historiapara que los participantes se acuerden). Segúnustedes, ¿qué pasaría después? ¿en quémomento y cómo se da cuenta la familia de quela mujer está grave? ¿quiénes deciden lo quese va hacer? ¿qué hacen? (aceptar que se va amorir, llamar a un curandero, llevarla a unservicio de salud: de religiosos, institucional,prestadoras) ¿Qué pasa con la enferma al final(muere, sobrevive)?
5. ¿Qué problemas tienen que pasar para tratarde salvar la vida de esta señora? ¿qué necesitanpara resolver esos problemas? ¿quién losayuda? ¿quién no los ayuda? (a distintosniveles: familia, comunidad, redes fuera de lacomunidad) ¿qué tan difícil resulta resolverestos problemas?
6. Si estuvieran ustedes en esa situación, ¿quéharían?
7. ¿Qué sucede cuando una mujer muere en lacomunidad? ¿Con quién se quedan los niños?¿Quién se ocupa de ellos? ¿Qué pasa con elesposo?
48
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
PARTE IIPresentación de video 2, seguida de discusiónEl facilitador explica a los participantes que van aver una parte de otra película y que después ladiscutirán juntos como la anterior.Observación: ver si los participantes estánsiguiendo con atención el video. Pasarlo unasegunda vez para asegurarse de que todos hanprestado atención.
Video 2: supuesto caso en el que se decidió llevara la señora a un servicio de salud (red financiadacon fondos estatales)
Dramatización: llegan al Servicio de Salud yun proveedor de servicios los recibe diciendoque cómo esperaron tanto. Está molesto conla familia y con la comadrona. Llega elproveedor de salud médico de turno (joven) queno habla el idioma y explica, con buenavoluntad, lo que la paciente tiene. El intérpretetiene dificultad para traducir porque el médicoha utilizado términos técnicos que no existenen la lengua del lugar. El médico se pone abuscar el instrumental que necesita paraintervenir y todos alrededor se empiezan amovilizar, y se corta.
Clip 2, preguntas para la discusión:1. ¿Qué es lo que vieron en la película?
(expliquen qué es lo que está pasando en lapelícula: ¿Qué está pasando?
2. ¿Les ha pasado a ustedes o a alguien queconozcan algo parecido? ¿qué sucedió?
3. ¿Qué es lo que más les llama la atención deesta segunda película? ¿qué otras cosas ven?¿es así en los servicios de salud que ustedesconocen?
4. (Si es necesario, retomar el hilo de la historiapara que los participantes se acuerden). ¿Seacuerdan que les mostramos sólo una partede la película?
5. ¿Qué creen ustedes que pasó al inicio (en laparte de la película que no les hemosmostrado: cuando la familia llega al serviciode salud)?5.1 (Si el tema no fue abordado en la
proyección anterior) ¿cómo hizo lafamilia para llegar al servicio de salud?
5.2 ¿Cómo recibieron a la familia en elservicio de salud? ¿Cómo piensanustedes que el personal de salud tratóa la familia, a la señora, a la comadrona? ¿Les dejaron hacer preguntas? ¿Cómoles contestaron?
5.3 ¿Qué le dijo el personal de salud a lacomadrona?
6. Y en el pedazo de película que hemos visto,¿Cómo piensan ustedes que se siente laseñora y la familia en el lugar donde la estánatendiendo? ¿Qué les parece el lugar dondeatienden a la señora? ¿Cómo ven ese lugar?
49
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
¿Qué es lo que hay y qué es lo que falta en elservicio de salud? ¿Qué es lo que les gusta yqué es lo que no les gusta?
7. Si estuvieran ustedes. en esa situación, ¿quéharían?
8. Al final de la película (que tampoco hemosvisto porque la cortamos antes) ¿qué creenustedes que pasa con la señora? (¿la señorasobrevive o muere?)
9. ¿Cuál sería un final feliz para esta segundapelícula? Para llegar a ese final feliz, ¿qué senecesitaría?
10. ¿Cómo les gustaría a ustedes que lostrataran en los servicios de salud?
PARTE IIIDramatización seguida de priorizaciónSe pide a los participantes que se dividan en dos otres grupos (dependiendo del número de personas).Cada grupo va a representar cómo le gustaría queterminara la primera historia que acabamos dever: desde el momento en que llega la señora a unservicio de salud hasta que se le salva la vida.OJO: Empezamos con la dramatización del finalfeliz relacionado al video 2 que acabamos deproyectar.
Dramatización de mujer grave en los serviciosde salud: final feliz.Cada grupo presenta su dramatización (quees a su vez grabada, como el resto delencuentro).Dramatización 1, discusión: priorizaciónSe pide a los participantes que comenten ladramatización del otro grupo y la de su propiogrupo:Preguntas del facilitador: ¿cómo se sintieronen el servicio de salud?, ¿qué encontraron queles gustó?, ¿cómo los trataron?, ¿cómo se logrosalvar a la mujer enferma?El facilitador va dibujando imágenes en elpapelógrafo de lo que la gente va diciendo (estolo puede hacer otro miembro del equipo quetenga aptitudes para el dibujo).21 Facilitadory observador van tomando nota de loselementos mencionados por los participantespara completar las imágenes en el papelógrafo.Una vez que los dos grupos han hecho suscomentarios, el facilitador hace la siguientepregunta (priorización):1. Si tuvieran que poner en orden de
importancia todo lo que han mencionado,
21 Otra posibilidad sería utilizar un flanelógrafo con imágenes preparadas de antemano. Para esto lo que se podría hacer es veren las primeras reuniones cuáles son los elementos que salen en el discurso de los participantes. Se podría entoncescomenzar a fabricar este flanelógrafo que quedaría como herramienta de animación para reuniones posteriores durante lainvestigación y en otras fases del proyecto; ya que se trata de una investigación-acción.
50
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
¿qué vendría primero? ¿y después?Explorar por qué ese orden de prioridad.Se ordenan los elementos en el orden deprioridad señalado por los participantes(poner número 1, 2, etc. en la lista delpapelógrafo).
PARTE IVDramatización seguida de mapeo comunitarioSe pide a los participantes que se dividan en dos otres grupos (dependiendo del número de personas).Cada grupo va a representar cómo le gustaría queterminara la primera historia que vimos juntos(video 1): desde el momento en que la señora seenferma hasta que se decide qué hacer. Se lesexplica que la dramatización o representacióntiene que mostrar cómo se organiza la comunidadpara un caso grave (emergencia en la comunidad):¿qué deciden hacer?, ¿en qué momento toman ladecisión?, ¿cómo logran sacar a la mujer de su casapara salvarla?, ¿qué los ayuda?, ¿quiénes losayudan?
Dramatización de emergencia en lacomunidad: final feliz.Cada grupo presenta su dramatización (quees a su vez grabada, como el resto delencuentro).
Dramatización 2, discusión: mapeoSe pide a los participantes que comenten ladramatización del otro grupo y la de su propiogrupo.
Preguntas del facilitador:1. ¿Quiénes pueden ayudar para lograr estos
finales felices? ¿por ejemplo, para llevara la mujer a un servicio de salud donde lapuedan salvar? ¿quién puede ayudar atomar la decisión a tiempo? ¿quién puedeayudar con el transporte? ¿quién puedeavisar de la emergencia a los otrosmiembros de la comunidad y al serviciode salud?
El facilitador dibuja en el papelógrafo figurasque representen a estos actores.22
2. ¿Dónde están estas personas en sucomunidad? ¿cerca de la casa? ¿lejos de lacasa? ¿cómo se puede hacer paraubicarlos? ¿se puede hablar con ellos?
El facilitador, mediante la información que losparticipantes aportan, va dibujando un mapade la comunidad en el cual se pueda ubicarlas personas claves que pueden ayudar a lasfamilias en caso de emergencia: poder localinstitucional, poder local tradicional, redtradicional de salud, vecinos, etc. Mostrandoel mapa a los participantes, el facilitador
22 Se puede pensar también en la fabricación de un flanelógrafo como en el caso anterior.
51
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
verifica que su representación corresponde alo que ellos están diciendo y lanza la siguientepregunta final al grupo:
3. ¿Qué puede hacer la comunidad paraayudar en casos de emergencia? ¿nospodremos movilizar todos juntos parasalvar vidas?
Para terminar la reunión:Explicar que el objetivo es justamente trabajar conla comunidad para mejorar los servicios de salud,para ayudarlos a prevenir problemas de salud, yapoyarlos a enfrentar casos de emergencia paralograr así salvar vidas. Recalcar que se trata deun proceso a largo plazo y que éste es sólo el inicio.Se les agradece por su participación y se les invita
a hacer sus últimos comentarios (si tienen algoque añadir). Luego se concluye la charlaexplicando cuál será el seguimiento. En estesentido, se sugiere recalcar que éste es el iniciode un trabajo conjunto; que regresaremos alas comunidades para dar un seguimiento aeste proceso.
NOTA: El seguimiento a esta recolección dedatos podría resultar en una retroalimentaciónde los resultados de la investigación-acción ala comunidad, en forma de desarrollo de planeslocales de emergencia (el nombre que se daráa este tipo de iniciativa saldrá de los gruposmismos). No debemos olvidar involucrar (deuna manera o de otra) a las personas queaceptaron participar en la discusión en las otrasetapas del proyecto.
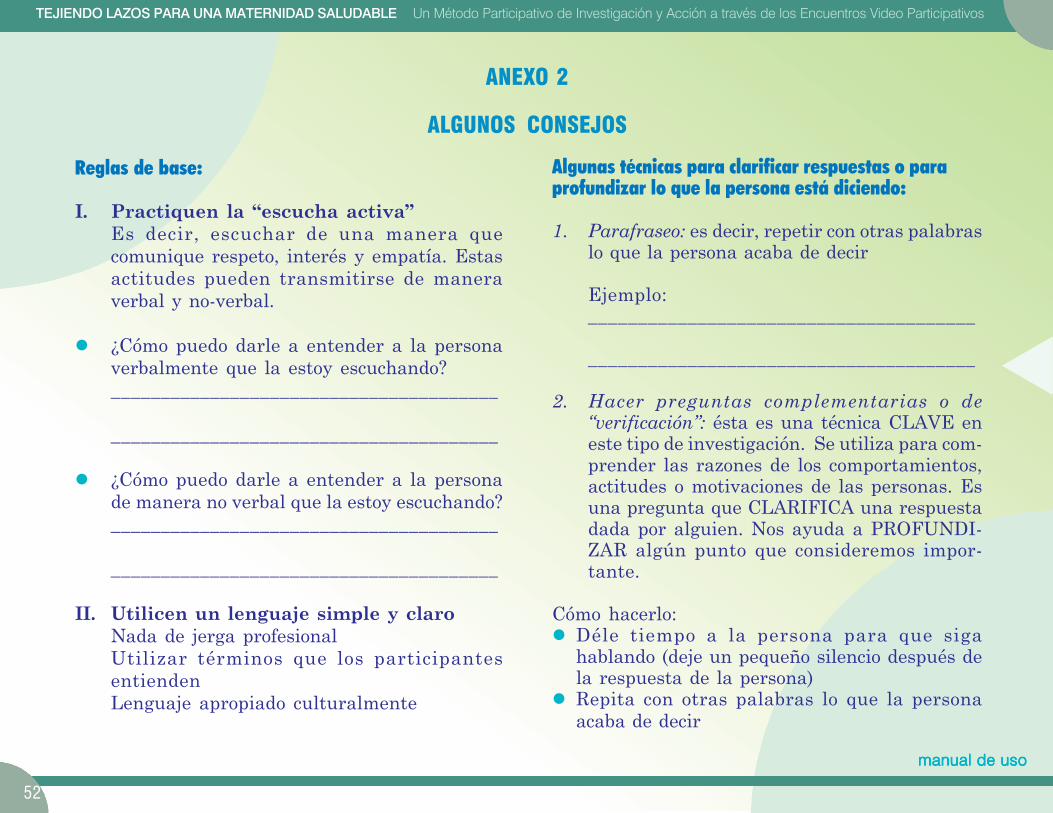
52
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
ANEXO 2
ALGUNOS CONSEJOS
Reglas de base:
I. Practiquen la “escucha activa”Es decir, escuchar de una manera quecomunique respeto, interés y empatía. Estasactitudes pueden transmitirse de maneraverbal y no-verbal.
¿Cómo puedo darle a entender a la personaverbalmente que la estoy escuchando?_______________________________________
_______________________________________
¿Cómo puedo darle a entender a la personade manera no verbal que la estoy escuchando?_______________________________________
_______________________________________
II. Utilicen un lenguaje simple y claroNada de jerga profesionalUtilizar términos que los participantesentiendenLenguaje apropiado culturalmente
Algunas técnicas para clarificar respuestas o paraprofundizar lo que la persona está diciendo:
1. Parafraseo: es decir, repetir con otras palabraslo que la persona acaba de decir
Ejemplo:_______________________________________
_______________________________________
2. Hacer preguntas complementarias o de“verificación”: ésta es una técnica CLAVE eneste tipo de investigación. Se utiliza para com-prender las razones de los comportamientos,actitudes o motivaciones de las personas. Esuna pregunta que CLARIFICA una respuestadada por alguien. Nos ayuda a PROFUNDI-ZAR algún punto que consideremos impor-tante.
Cómo hacerlo:Déle tiempo a la persona para que sigahablando (deje un pequeño silencio después dela respuesta de la persona)Repita con otras palabras lo que la personaacaba de decir
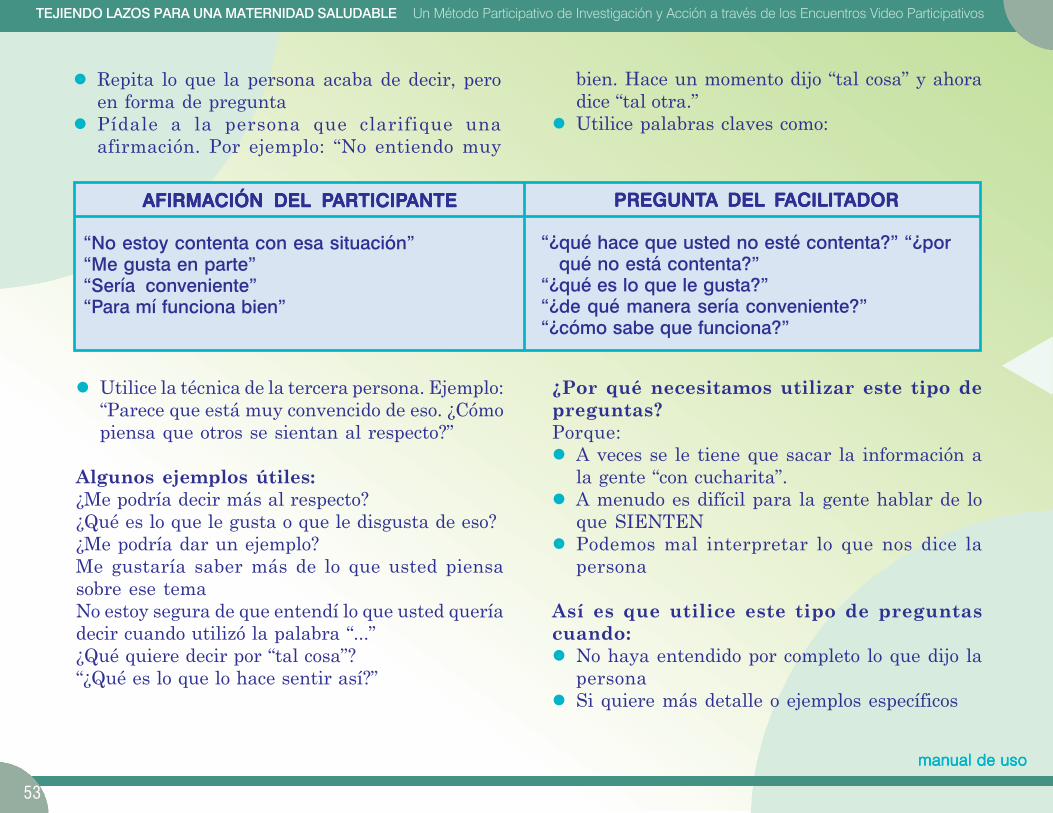
53
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Repita lo que la persona acaba de decir, peroen forma de preguntaPídale a la persona que clarifique unaafirmación. Por ejemplo: “No entiendo muy
bien. Hace un momento dijo “tal cosa” y ahoradice “tal otra.”Utilice palabras claves como:
AFIRMACIÓN DEL PAFIRMACIÓN DEL PAFIRMACIÓN DEL PAFIRMACIÓN DEL PAFIRMACIÓN DEL PARTICIPARTICIPARTICIPARTICIPARTICIPANTEANTEANTEANTEANTE
“No estoy contenta con esa situación”“Me gusta en parte”“Sería conveniente”“Para mí funciona bien”
PREGUNTPREGUNTPREGUNTPREGUNTPREGUNTA DEL FA DEL FA DEL FA DEL FA DEL FACILITACILITACILITACILITACILITADORADORADORADORADOR
“¿qué hace que usted no esté contenta?” “¿porqué no está contenta?”
“¿qué es lo que le gusta?”“¿de qué manera sería conveniente?”“¿cómo sabe que funciona?”
Utilice la técnica de la tercera persona. Ejemplo:“Parece que está muy convencido de eso. ¿Cómopiensa que otros se sientan al respecto?”
Algunos ejemplos útiles:¿Me podría decir más al respecto?¿Qué es lo que le gusta o que le disgusta de eso?¿Me podría dar un ejemplo?Me gustaría saber más de lo que usted piensasobre ese temaNo estoy segura de que entendí lo que usted queríadecir cuando utilizó la palabra “...”¿Qué quiere decir por “tal cosa”?“¿Qué es lo que lo hace sentir así?”
¿Por qué necesitamos utilizar este tipo depreguntas?Porque:
A veces se le tiene que sacar la información ala gente “con cucharita”.A menudo es difícil para la gente hablar de loque SIENTENPodemos mal interpretar lo que nos dice lapersona
Así es que utilice este tipo de preguntascuando:
No haya entendido por completo lo que dijo lapersonaSi quiere más detalle o ejemplos específicos
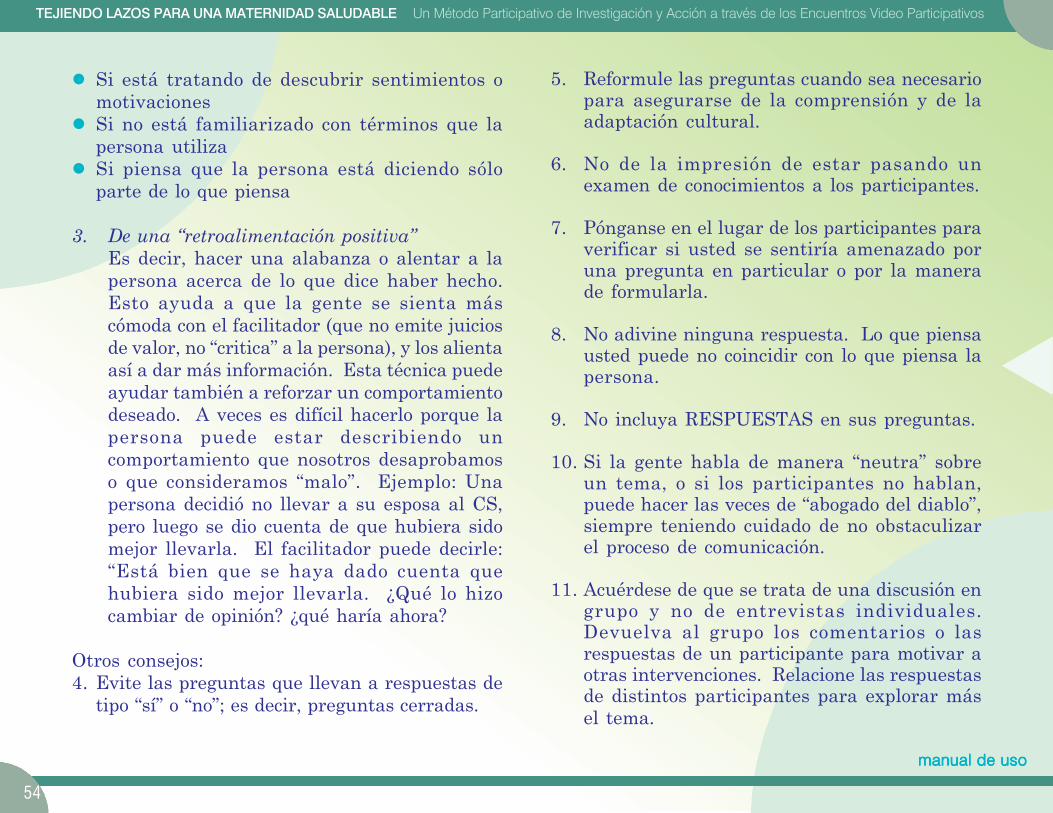
54
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Si está tratando de descubrir sentimientos omotivacionesSi no está familiarizado con términos que lapersona utilizaSi piensa que la persona está diciendo sóloparte de lo que piensa
3. De una “retroalimentación positiva”Es decir, hacer una alabanza o alentar a lapersona acerca de lo que dice haber hecho.Esto ayuda a que la gente se sienta máscómoda con el facilitador (que no emite juiciosde valor, no “critica” a la persona), y los alientaasí a dar más información. Esta técnica puedeayudar también a reforzar un comportamientodeseado. A veces es difícil hacerlo porque lapersona puede estar describiendo uncomportamiento que nosotros desaprobamoso que consideramos “malo”. Ejemplo: Unapersona decidió no llevar a su esposa al CS,pero luego se dio cuenta de que hubiera sidomejor llevarla. El facilitador puede decirle:“Está bien que se haya dado cuenta quehubiera sido mejor llevarla. ¿Qué lo hizocambiar de opinión? ¿qué haría ahora?
Otros consejos:4. Evite las preguntas que llevan a respuestas de
tipo “sí” o “no”; es decir, preguntas cerradas.
5. Reformule las preguntas cuando sea necesariopara asegurarse de la comprensión y de laadaptación cultural.
6. No de la impresión de estar pasando unexamen de conocimientos a los participantes.
7. Pónganse en el lugar de los participantes paraverificar si usted se sentiría amenazado poruna pregunta en particular o por la manerade formularla.
8. No adivine ninguna respuesta. Lo que piensausted puede no coincidir con lo que piensa lapersona.
9. No incluya RESPUESTAS en sus preguntas.
10. Si la gente habla de manera “neutra” sobreun tema, o si los participantes no hablan,puede hacer las veces de “abogado del diablo”,siempre teniendo cuidado de no obstaculizarel proceso de comunicación.
11. Acuérdese de que se trata de una discusión engrupo y no de entrevistas individuales.Devuelva al grupo los comentarios o lasrespuestas de un participante para motivar aotras intervenciones. Relacione las respuestasde distintos participantes para explorar másel tema.
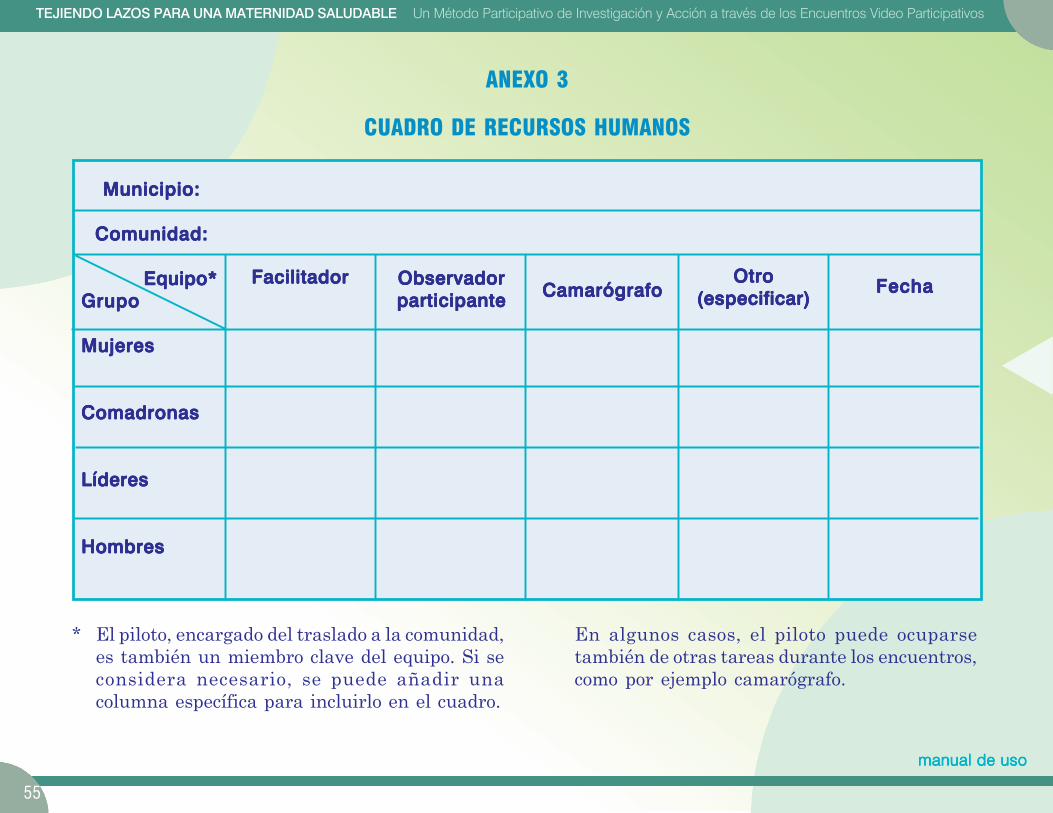
55
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
ANEXO 3
CUADRO DE RECURSOS HUMANOS
Municipio:Municipio:Municipio:Municipio:Municipio:
Comunidad:Comunidad:Comunidad:Comunidad:Comunidad:
Equipo* Equipo* Equipo* Equipo* Equipo*GrupoGrupoGrupoGrupoGrupo
MujeresMujeresMujeresMujeresMujeres
ComadronasComadronasComadronasComadronasComadronas
LíderesLíderesLíderesLíderesLíderes
HombresHombresHombresHombresHombres
FacilitadorFacilitadorFacilitadorFacilitadorFacilitador ObservadorObservadorObservadorObservadorObservadorparticipanteparticipanteparticipanteparticipanteparticipante CamarógrafoCamarógrafoCamarógrafoCamarógrafoCamarógrafo
OtroOtroOtroOtroOtro(especificar)(especificar)(especificar)(especificar)(especificar)
FechaFechaFechaFechaFecha
* El piloto, encargado del traslado a la comunidad,es también un miembro clave del equipo. Si seconsidera necesario, se puede añadir unacolumna específica para incluirlo en el cuadro.
En algunos casos, el piloto puede ocuparsetambién de otras tareas durante los encuentros,como por ejemplo camarógrafo.
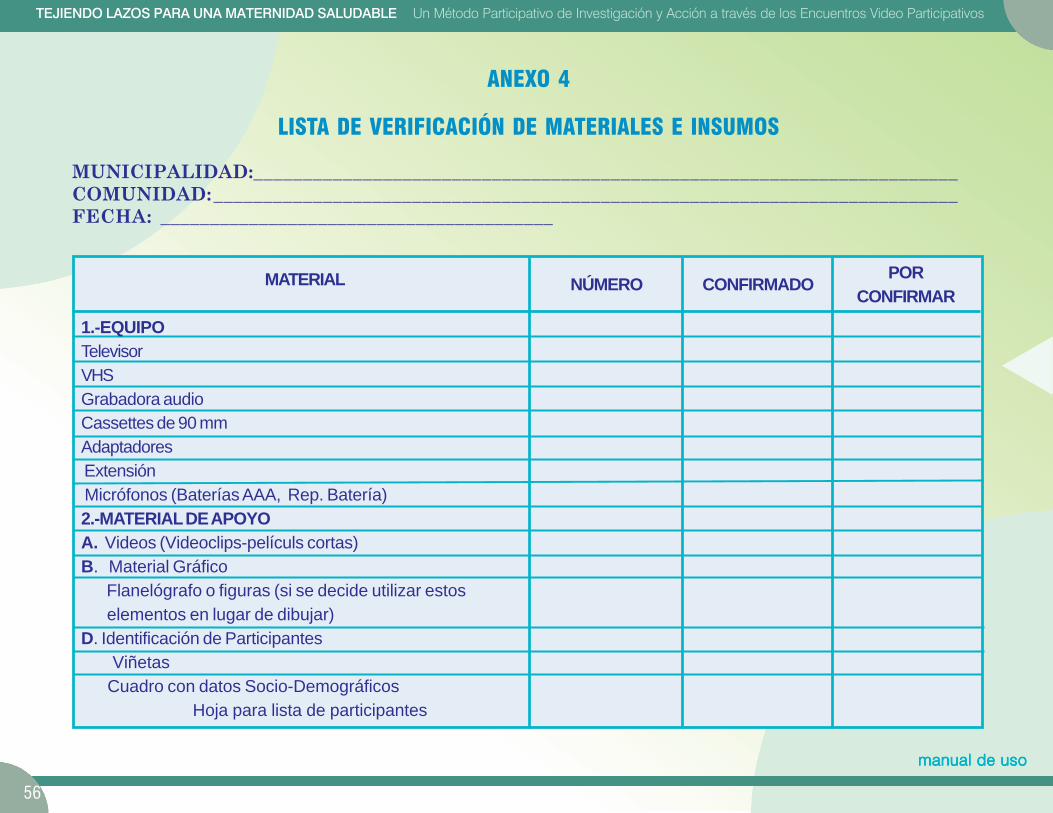
56
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
NÚMERO CONFIRMADO PORCONFIRMAR
ANEXO 4
LISTA DE VERIFICACIÓN DE MATERIALES E INSUMOS
MUNICIPALIDAD:_______________________________________________________________________COMUNIDAD:___________________________________________________________________________FECHA: ________________________________________
MATERIAL
1.-EQUIPOTelevisorVHSGrabadora audioCassettes de 90 mmAdaptadores Extensión Micrófonos (Baterías AAA, Rep. Batería)2.-MATERIAL DE APOYOA. Videos (Videoclips-películs cortas)B. Material Gráfico Flanelógrafo o figuras (si se decide utilizar estos elementos en lugar de dibujar)D. Identificación de Participantes Viñetas Cuadro con datos Socio-Demográficos Hoja para lista de participantes
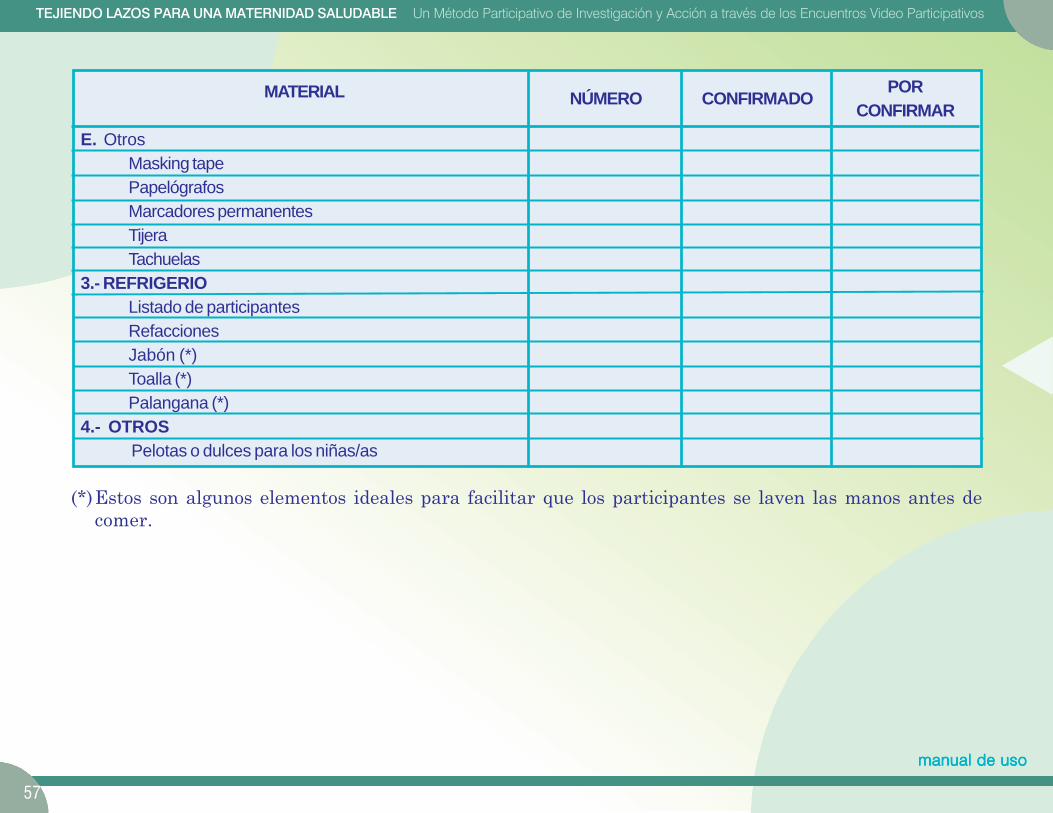
57
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
NÚMERO CONFIRMADO PORCONFIRMAR
MATERIAL
E. OtrosMasking tapePapelógrafosMarcadores permanentesTijeraTachuelas
3.- REFRIGERIOListado de participantesRefaccionesJabón (*)Toalla (*)Palangana (*)
4.- OTROSPelotas o dulces para los niñas/as
(*)Estos son algunos elementos ideales para facilitar que los participantes se laven las manos antes decomer.
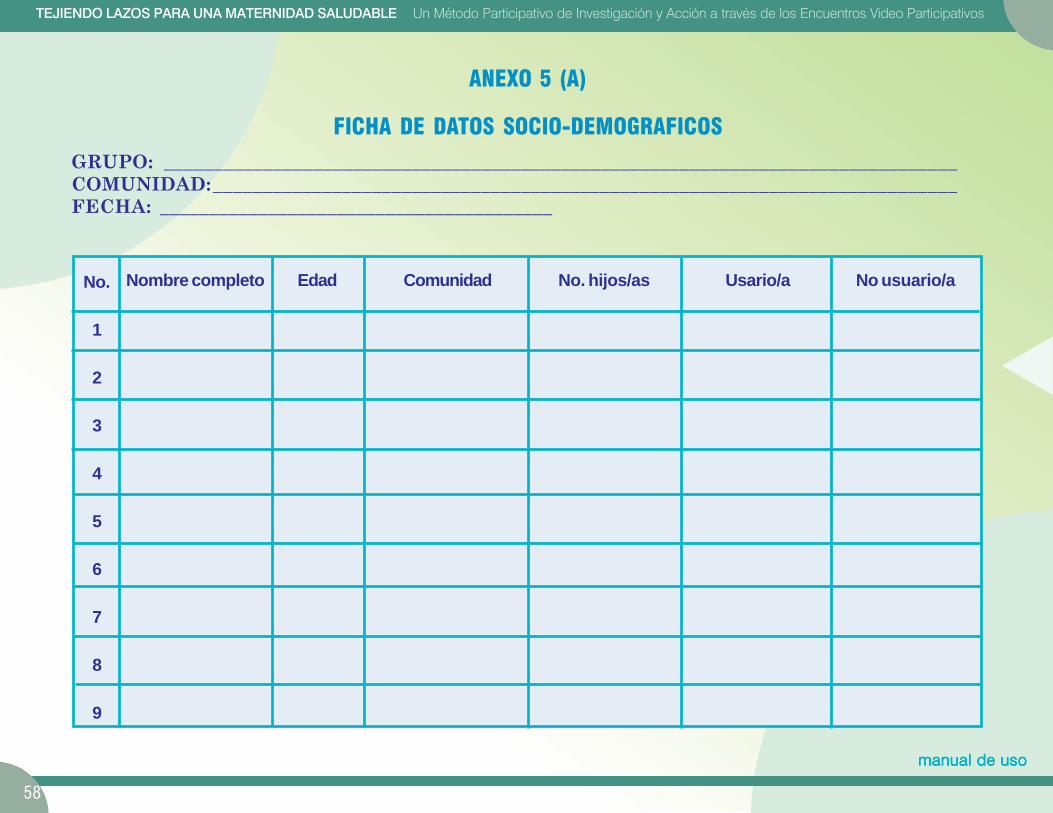
58
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
No. hijos/as Usario/a No usuario/a
ANEXO 5 (A)
FICHA DE DATOS SOCIO-DEMOGRAFICOSGRUPO: ________________________________________________________________________________COMUNIDAD:___________________________________________________________________________FECHA: ________________________________________
No.
1
2
3
4
5
6
7
8
9
Nombre completo Edad Comunidad

59
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Grupo u organización
ANEXO 5 (B)
FICHA DE DATOS SOCIO-DEMOGRAFICOS (LIDERES)GRUPO: ________________________________________________________________________________COMUNIDAD:___________________________________________________________________________FECHA: ________________________________________
No.
1
2
3
4
5
6
7
8
9
Nombre Edad Comunidad
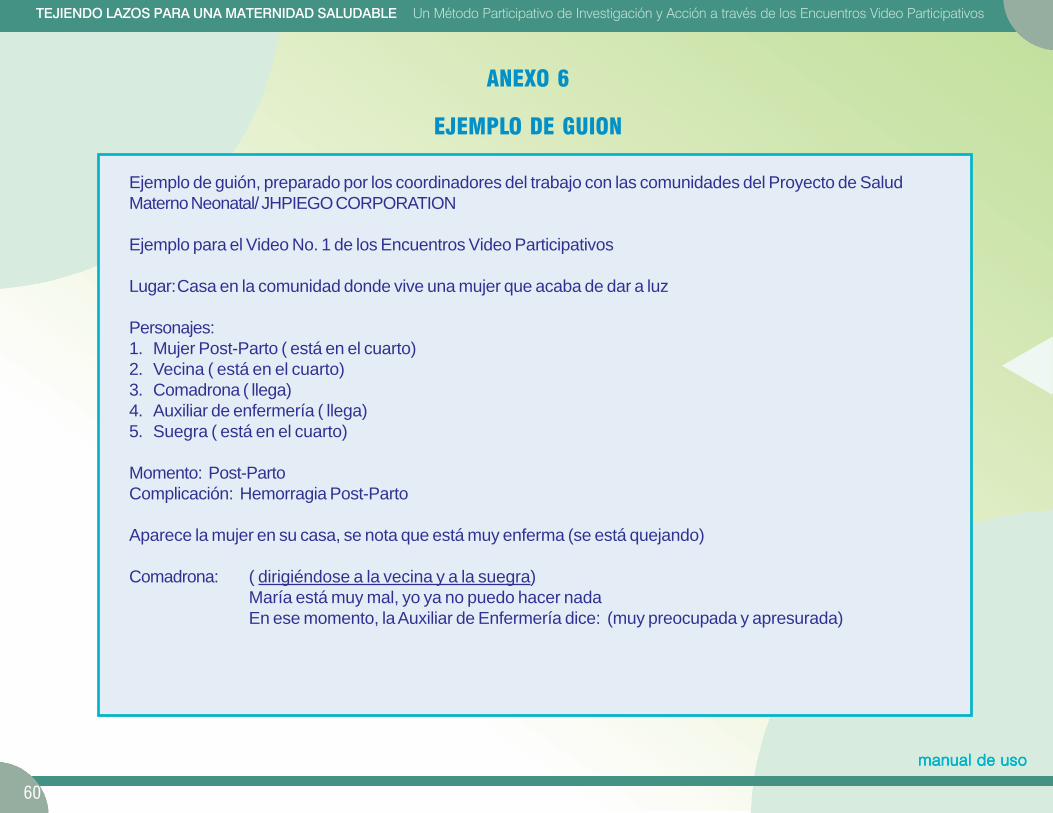
60
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
ANEXO 6
EJEMPLO DE GUION
Ejemplo de guión, preparado por los coordinadores del trabajo con las comunidades del Proyecto de SaludMaterno Neonatal/ JHPIEGO CORPORATION
Ejemplo para el Video No. 1 de los Encuentros Video Participativos
Lugar:Casa en la comunidad donde vive una mujer que acaba de dar a luz
Personajes:1. Mujer Post-Parto ( está en el cuarto)2. Vecina ( está en el cuarto)3. Comadrona ( llega)4. Auxiliar de enfermería ( llega)5. Suegra ( está en el cuarto)
Momento: Post-PartoComplicación: Hemorragia Post-Parto
Aparece la mujer en su casa, se nota que está muy enferma (se está quejando)
Comadrona: ( dirigiéndose a la vecina y a la suegra)María está muy mal, yo ya no puedo hacer nadaEn ese momento, la Auxiliar de Enfermería dice: (muy preocupada y apresurada)
61
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
Auxiliar deEnfermería: Doña Juana deje que llevemos a María al hospital, está grave, se puede morir. Necesitamos
buscar ayuda para que se cure.
Suegra: Es que Juan no está, no sé cuando regresa y yo no puedo dejar que la lleven al hospital, ellos novan a dejarnos entrar con ella y se nos va a morir ( preocupada, pero convencida que no va a dejarque se la lleven)
En ese momento, la discusión aumenta entre todos (el tono y los gestos de unos a favor de llevarla y otros que noestán de acuerdo, menos la mujer).(Pueden hablar al mismo tiempo)
SE CORTA LA FILMACION.
62
TEJIENDO LAZOS PARA UNA MATERNIDAD SALUDABLE Un Método Participativo de Investigación y Acción a través de los Encuentros Video Participativos
manual de usomanual de usomanual de usomanual de usomanual de uso
ANEXO 7
TRANSCRIPCIONES — ALGUNOS CONSEJOS
El formato que la persona utilice para vaciar lainformación, dependerá del uso que se quierahacer de la transcripción. Así, si se ha grabado lareunión en video y se quiere después editar lofilmado, se le proporcionará un formato en el sepuedan plasmar tanto las imágenes como el texto.
Si se piensa utilizar la transcripción para unanálisis del discurso (verbal) de los participantes,bastará con transcribir las intervenciones oralesde los participantes.
Algunas instrucciones para las transcripciones
Indicar quién habla en cada caso.
Traducir lo que la persona dice tal como lo dice.
No hacer resúmenes ni sintetizar lo que la persona dice.
Cuando resulte difícil o imposible traducir palabras al castellano (porque no existen en nuestrovocabulario), escribirlas en la lengua local y explicar entre paréntesis lo que significan, aunqueeso implique una explicación detallada de su significado
Cuando la traducción literal de la palabra ilustra maneras de pensar o de ver el mundo,ceñirse a la traducción “literal” y explicar entre paréntesis lo que la palabra significa en elcontexto (por ejemplo, si la persona usa el término “suciedad” para referirse a la menstruación,escribir “suciedad” y explicar entre paréntesis lo que significa).
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Method of Participatory Research and Action Using Video Discussion Meetings Practical Guide
2
Thank you for your support!
Educational Producers and Evaluators
Marcela Tapia, Patricia Poppe, Robert Ainslie
Adaptation for Guatemala
Human Resources Responsible for the Investigation
Technical Reviewers Ministry of Public Health and Social Welfare of Guatemala
National Program for Reproductive Health, Executive Board,
USAID
Collaborators
Technical and Administrative Personnel of the Maternal and
Neonatal Health Project
Regional Health Offices:
Groups of women, men, leaders, midwives, providers
(purpose of the investigation)
Photographs
Graphic Design and Diagrams
Note: It is important to indicate that in this document the masculine gender has been used on most occasions in which the text might
refer to either men or women. This measure has been adopted with the sole intention of simplifying the text, without any suggestion of
preference.
This publication was made possible with the support of the Agency for International Development (AID), under Contract No. C.A.
HRN-A-0098-00043-00. The opinions expressed are those of the authors and do not necessarily reflect the point of view of AID.
Guatemala, January 2004
3
TABLE OF CONTENTS
INTRODUCTION
I. Human Resources or Raw Material for the
Participatory Research A. Potential Partners
B. Visions of the World and of Health
C. Basis in Reality
D. The Gender Lens
E. The Process of Changing from Soliciting Help to
Taking Power
II. Participatory Video Discussion Meeting A. Necessary Characteristics
B. Objectives of This Tool
C. Components of the Methodology
1. Discussion Guide
2. Introduction and Development
3. Prioritization of the Subject Matter
4. Community Mapping
D. Production of the Videos
E. Human Resources
F. Advance Planning and Logistics
G. Resource Management (the things you need)
H. Time Management
I. Space Management
J. Systematizing (documenting) the Experiment
III. Creating Bonds of Trust
IV. Appendices
1. Discussion Guide: The data collection
instrument for participatory video discussion
meetings
2. A few tips
3. Table of human resources
4. Checklist of materials and supplies
5. (A) Socio-demographic information sheet
5. (B) Socio-demographic information sheet
(leaders)
6. Sample script
7. Some tips on transcribing
8. Possible formats for organizing the discussion
meetings
4
INTRODUCTION The purpose of this guide is to lead you step by step
through the application of a “methodology” of
participatory research in a health project.
The subjects of the videos presented in this guide are
related to maternal and neonatal health, since that is
the focus of the Maternal and Neonatal Health Project
of the JHPIEGO Corporation. However, the end
result is to provide a tool that can support us in
resolving any health problem, and which can be
adapted to the needs of the community and of
organizations desiring to carry out participatory
research (or participatory investigation).
We will call this “method (instrument or tool)”
participatory video discussion meeting, consisting
of a meeting in which video taped images (short film)
from a real situation are used to stimulate dialogue
and discussion among the participants.
This guide consists of three parts and a section of
appendices at the end.
The first part examines the essential and most
important resource for this work, that is, the human
element or raw material of the participatory
research.
The second part, entitled The Tool or Participatory
Video Discussion Meetings, contains instructions for
carrying out these discussion meetings, presents the
objectives of the “videoclips” (videos or short films)
and basic principles of production. It provides general
information on the organization of these discussion
meetings and how to document the experience.
The third, entitled Creating Bonds of Trust, refers to
the process of dialogue and participation that goes
beyond the methodology and supports its use.
WELCOME!
5
I. Human resources or raw material for the participatory research
Every process of participatory research should
validate the human potential existing in the
communities. Five factors are described below which
we suggest be taken into consideration when
planning to work within a community.
A. Potential Partners In every community, we will find two kinds of agents:
Change agents
People who have influence over others and who
are capable of generating change in the
community, such as some community leaders and
deputy mayors.
External collaborating agents People from outside the community who
“facilitate” the change, such as people from
projects, NGOs, the Ministry of Health, etc.
Other players Women of reproductive age, midwives, heads of
families, and groups that are usually absent from
community decision-making. Other key players in
the participatory research process are health
service staff members. Ideally they should
participate in the process.
It is important at the beginning to secure the
authorization of health authorities, municipal
authorities, etc., to conduct the investigation.
There is no single model for initiating the process of
change within a community supported by
participatory research. The important thing is to
change the focus of the endeavor from being centered
on “what we don’t have” to one centered on the
“strengths” of the community and of the players
involved, that is, an effort centered on “what we do
have.”
6
B. Visions of the World and of Health
Many development projects and programs have
learned that it is necessary to take into account the
point of view of those who have an interest in a
specific problem or theme, and that it is not
appropriate to try to impose patterns of behavior that
are foreign to the local culture.
To reach the objectives of an investigation, project or
program, we recommend that you:
Recognize and respect the cultural differences
between the external collaborating agents and the
community
Understand how “the other” sees his own problems
and reality
Know what health means to the community, for
example, its values, priorities and traditions
Know what the community thinks of the health
services, that is, the “attributes of quality.”
C. Basis in Reality
The participatory research needs to be integrated with
existing organizational initiatives, and take into
account the priorities the community establishes to
resolve its problems. For example, the project of
building a community maternity center could be the
engine that drives the participatory research process
with the community.
D. The Gender Lens
Remember that within the vulnerable groups, women
must be included in making decisions about matters
that directly affect them.
E. The Process of Changing from Soliciting Help to Taking Power
It is important not to fall into the paternalism or
“aidism” that consists of doing things for the
community instead of doing them with the
community. Empowerment is the process by which
people develop skills, make decisions, increase their
self-confidence, and take ownership of the situation.
7
II. Participatory Video Discussion Meeting
A. Necessary Characteristics
Must respond to precise objectives;
Must be in harmony with the goal of the
participatory research;
Must reinforce community participation in caring
for the health of the mother and the newborn;
Must be culturally appropriate (adapted as much as
possible to the customs and needs of the
community).
B. Objectives of This Tool To learn the community’s perception of its health
services;
To facilitate active community participation in the
evaluation of those services; and
To walk the community through the process of
implementing and executing Community
Emergency Plans.
This participatory research tool should start with the
reality of the community motivate it to discuss
subjects that directly affect it by using videos as
discussion starters.
C. Components of the Methodology
1. Discussion Guide Includes the description of the videos, exercises and
the questions that will be asked during the
participatory video discussion meetings. It is a guide
for
8
facilitating dialogue, and should not be used as a
questionnaire.
(This discussion guide can be found in Appendix
1.)
2. Introduction and Development The way the project, program, organization,
institution and team of facilitators are introduced will
motivate those present to participate and express their
viewpoints freely.
One of the people responsible for making this happen
will be the facilitator, who will:
Explain in simple terms and in the language of the
majority the objective of the project he/she
represents. In addition, he will indicate that the
health and municipal authorities have given their
endorsement so that the activity may take place. It
is best if the introduction of the activity can be
done in conjunction with the mayor or deputy
mayor and a local representative of the Ministry of
Health as members of the team, who will say a few
words to the group.
Briefly explain the objective of the meeting.
Explain that this methodology is different from the
traditional approach; it is not “like school,” that is,
lecturing, but is “participatory.”
Thank the participants for coming.
Mention that the subject of discussion is the health
of pregnant women, mothers and their newborns.
State that the group of facilitators wishes to learn
with the community and get to know the points of
view of its members regarding health issues.
NOT offer money or create false expectations
among the participants.
Explain that the team wants to support them by
facilitating a brainstorming session on how to
organize to “save the lives” of people who are in a
health crisis and getting worse by the minute.
Assure them that what they say will be kept private
and only used for the purpose of the investigation.
Explain the need to record the session so that what
they say may be taken into account. In addition,
promote respect for what each one says, and
respect the decision of the group if it does not wish
the meeting to be recorded.
Explain the procedure that will be followed during
the discussion meeting. Example: “We are going
to watch a short film together that has been
prepared for this meeting, and afterwards we will
talk about what each one thinks of what we have
seen in the film.”
Invite them to interrupt him at any time if he says
anything that is unclear.
9
Introduce the members of the team or have them
introduce themselves to the participants.
State how long the session will last.
If staff members from the health services are
present, it is recommended that they not give their
titles when introducing themselves, as this may
intimidate the participants.
Explain that the meeting will start with a small
exercise or game to help them “get to know each
other better.”
Choose an exercise that is active, that allows
participants to interact with each other, that involves
the entire group and contains some humor.
3. Prioritization of the Subject Matter
The objective of a prioritization exercise is to probe a
subject that has been presented in the video, for
example, identifying which indicators of quality are
most important from the community’s point of view.
Note:
An example of prioritization is presented
subsequently in the content and objectives of two
videos.
10
a. Video 1 Objectives
To explore what the community does in case of an
emergency during childbirth or immediately after
childbirth.
To identify customs and traditions relating to care
of the mother and of the newborn.
To explore, “What prevents a woman from being
taken to a health center or hospital?”
To explore what could facilitate the transportation
of a woman to a health center or hospital.
To explore who the decision-makers are in the
community.
To explore what the community knows about the
danger signs of pregnancy and childbirth.
11
b. Video 2 Objectives
To explore what the community likes and does not
like about its health services and how it would like
the health services to be (“quality attributes or
indicators”).
To explore what the barriers are to using the health
services.
To explore what might facilitate greater use of
health services.
c. Rationale for conducting the prioritization exercise
For example, the participants might have mentioned
in the discussion of the video that they do not like
being treated badly or being yelled at when they bring
a pregnant woman with complications to the hospital,
but that they appreciate the fact that the doctor helps
them find a solution to the woman’s complication.
Therefore: What is most important to the participants?
The treatment given to the people accompanying
the woman to the hospital, or
The competence of the attending physician?
That is, they are pointing to a problem, but they are
also sharing “something positive” (opportunity) that
could be shared with the personnel in the health
centers to build up their self esteem and improve care.
d. Procedure for conducting the prioritization exercise
Ask participants to divide into two or three groups
(depending on the number of people), and say the
following: “Each group is going to act out how
they would like the story we have just seen to end
(video 2) from the moment the lady arrives at the
health center until they save her life.”
Each group presents its dramatization. The
facilitator asks the participants to comment on the
dramatizations of the other group and of their own
group, using questions such as these:
How did you feel in the health center?
What did you like and what didn’t you like?
How did they treat you?
How was the sick woman’s life saved?
12
The facilitator or observer draws pictures on a flip
chart of what the people are saying. As an
alternative, it is recommended to bring to the
meeting cutouts prepared in advance representing
the figures that might possibly be used, for
example, a man, a woman, a nurse, an injection,
money, transportation, etc.
When all comments have been made and all the
pictures are on the flip chart, the facilitator asks
questions to help the participants arrange the
components mentioned in order of priority:
- If you had to put everything that you have
mentioned in order of importance, what would
you put first? What next?
- The facilitator arranges the figures following
the order of priority indicated by the
participants (write number 1, 2, 3, etc. in a list
going down the side of the flip chart), letting
them know that their contributions have been
very important, since the information will be
used to design community emergency plans,
moreover, it will help in the development of
projects and interventions to improve the
quality of care in the health centers.
4. Community Mapping
The objective of this exercise is for the members of
the community to draw a map showing the location of
people who can help families in emergency cases,
including representatives of: the local institutional
authority, the local traditional authority, the traditional
health care system, the social network (for example,
neighbors and relatives), etc.
a. Procedure for Community Mapping
Ask participants to divide up into two or three
groups (depending on the number of people).
Say the following: “Each group is going to act out
how they would like the first story to end (Video
1) from the moment the lady’s condition becomes
critical until a decision is made about what to do.”
13
Explain to the participants that this dramatization
or representation needs to show what should
happen next:
- How the community can organize itself to bring
a successful outcome to a critical case like this
one.
- What do they decide to do? When do they
make the decision? How do they manage to get
the woman out of her house to save her life?
Who helps them?
Each group presents its dramatization.
The facilitator asks the participants to comment on
the dramatizations of the other group and of their
own group.
Following the discussion guide in Appendix 1, the
facilitator brings out who the key people are and
what resources are available in the community for
emergency cases, drawing figures on a flip chart to
represent these characters, or uses cutouts prepared
ahead of time.
Next, to identify the people and resources available
in the community for emergency cases, the
facilitator poses the questions suggested in the
guide.
The facilitator draws a map of the community with
the help of the participants and verifies that the
illustration matches what they are saying. If
possible, he may ask one of the participants to
come up front to help him make the map of
community resources. When this is done, the
facilitator poses the following questions to the
group:
1. What can the community do to help in cases of
emergency?
2. Is it possible for all of us to mobilize to save a
person’s life?
(These questions conclude the exchange on the central
theme of discussion.)
14
To conclude the meeting a. As a follow-up to the last question posed to the
participants, the facilitator explains the
objective of the team facilitating the meeting.
b. He/she thanks the group for participating and
invites participants to offer any final comments.
c. He/she concludes the session and explains what
the next steps will be. He/she indicates that this
is the beginning of a joint effort, and that the
team will return to the communities to follow
up and to share the results of the investigation.
After the meeting The facilitating team should get together immediately
after each session to:
Go over the strengths and weaknesses of the
team’s performance;
Determine whether or not the subject matter was
adequately covered;
Determine whether or not the information sought
was gathered from the discussion;
Ask, What themes were the most difficult to
address?
Did new themes come out of the discussion?
Discuss how to plan for the next meeting and how
to correct any mistakes or make any changes that
might improve the process.
D. Production of the Videos
The videos should be produced in advance and should
follow an established script. Each team can prepare
its own script, and should be sure to have the elements
necessary for filming: actors, costumes, materials,
camera, video cassette, etc.
The script is a proposal that can be adapted to the
context and needs of the community.
There are teams that prefer to go into the field and
have the resources to travel to a community and
videotape the local people, and in the best case
scenario, that is the ideal.
Others prefer to bring the actors to a neutral location
where they act out scenes that are taped and edited
into a video.
Before holding the meetings, you should make sure
there is electricity to be able to show “a video;”
however, if there is none, you can organize a group of
volunteers to act out “a social drama or
dramatization.” You will need to explain the
objectives and who should make the presentation with
each group that participates in the meetings.
15
An example of the script for video 1 is presented in
Appendix 6.
E. Human Resources The necessary members and their functions:
a. A facilitator: This is (ideally) a person from
the community who speaks the language of the
place, and who guides the group discussion.
b. A participating observer: This is the person
who takes notes during the meeting and helps
the facilitator, indicating, for example:
That there is someone in the meeting who
has something to say;
That it is necessary to bring into the
discussion a participant who is sleeping or
not participating;
That it would be good to return to a theme
that one of the participants mentioned, to
complete it, etc.
c. A camera operator: This is the person who
will record images of the discussion meeting
for the purpose of sharing them. This is part of
the learning process with the people and can be
used as a medium for promoting community
mobilization to develop Emergency Plans.
F. Advance Planning and Logistics
Conducting meetings in the country’s remote
communities requires a considerable amount of
organization and coordination. The port of entry into
the community is formal local authorities.
Steps to follow:
Visit the selected community ahead of time to
confirm its interest and the possibility of
conducting meetings in the area.
If this is confirmed, plan the visit and make
arrangements for the necessary human and
material resources.
16
G. Resource Management (the things you need)
Set up a table of human resources with names of
specific members of the facilitating team for each
locality. An example of the Table of Human
Resources can be found in Appendix 3.
Set up a table of the material resources with the list
of supplies that will be needed for the meeting, and
use it as a checklist a day before going out to the
community. And example of a Table of Material
Resources can be found in Appendix 4.
Prepare a socio-demographic information sheet for
recording the data (most important) concerning the
participants. See the example in Appendices 5A
and 5B.
Other preparatory tasks such as the translation of
the research guide or instrument into another local
language, should be performed ahead of time, and
the translation should respect the formulation and
the order of the questions in the original
instrument.
Make preparations for the work of transcription:
before going into the field, the team should locate
and contact with sufficient lead time the people
who will be doing the transcriptions, to ensure that
they will be completed as soon as possible.
Preferably, the facilitating team should also be
responsible for this task. These people should
speak the language of the place where the meeting
will take place, be fast typists, and, if possible, be
experienced in this type of work. They should be
given a sheet of instructions on how to do the
transcriptions. A model of instructions on how to
do transcription is presented in Appendix 7.
H. Time Management Calculating time is important at specific moments:
before, during, and after the meetings.
Before the meetings
Plan the meetings in advance and, as much as
possible, send a reminder one or two days before
the date of the meeting, in conjunction with health
personnel and/or local authorities.
Arrive at the location sufficiently ahead of time so
that the team can meet and iron out the final details
for each discussion meeting.
17
Plan the transcription of the sessions in advance,
taking into account the fact that it takes at least 8
hours to transcribe one hour of audio tape.
Anticipate follow-up activities and the outputs to
be presented as a result of the process.
Prepare a detailed workplan, taking into account
the points mentioned above.
During the meetings Plan each meeting taking into account the
characteristics of the community and the time
available to the participants. Keep in mind that the
participants’ time is valuable. You need to explain to
them the timeframe and process selected for the
discussion meeting and then keep to the times that you
have set. A table with the pattern for organizing
these meetings is presented in Appendix 8.
After the meetings Plan ahead of time the tasks of consolidation and
analysis of the information so that you can, in a
reasonable amount of time, transfer the information to
the stakeholders: the community itself and the
decision makers.
Refer to the workplan and respect the deadlines that
have been set. If this is not possible, communicate the
changes to the individuals involved (that is, those who
are waiting for the results from the team).
I. Space Management
You will need to take into account the physical
conditions in which you will be working, for example,
whether there is electricity or not (and if it is possible
to use an electric generator).
See to it that the room is as spacious as possible, but
not so large that it becomes a distraction. See to the
arrangement of the chairs, making sure that the
facilitator and his team are not positioned before the
audience as if in a lecture hall.
18
J. Systematizing (documenting) the experience
You can develop a journal of the most outstanding
moments, events and actions and, in this way, build a
vivid record of the process with the community. This
brief document of reflection and self examination
should be filled out at each meeting, including
everything having to do with preparation, invitations,
logistics and organization, facilitation, the use and
understanding of the instrument, the content of the
discussions, and the process with the community.
You can also keep a travelogue in which you can
document the formal and informal interviews and
observations of the facilitating team during their time
of residence in or visits to the community.
You can make tables summarizing the data
concerning the resources identified in the
communities, such as traditional and technical
communication media, sources of information,
networks, etc.
19
III. Creating Bonds of Trust To establish an open dialogue, you have to develop
bonds of trust and maintain them over time—
something that is not done from one day to the next.
Many times, the need to respect the rhythm of this
long term process runs up against the urgent need to
present results within precise workplans. So, how to
reconcile processes and outcomes? Within the
process of participatory research there are always
results that can and should be shared with the
stakeholders as they appear, and shared within
reasonable timeframes.
As the initiative progresses, it is necessary to work
within deadlines and offer useful outputs to the
stakeholders (communities and decision makers). The
success of this initiative has more to do with the
quality of the participation and the long term benefits
than with the number of people or communities
covered and the short term impact of the activities.
Bonds of trust are as much outputs as processes. It is
important to achieve a balance between short term
outputs and long term processes.
Important note It is recommended that on the day of the meeting you:
Try to create a good relationship with the
participants;
Arrive early at the meeting place;
Converse informally with everyone;
Invite the participants to share their information
(socio-demographic) with the person responsible
for collecting it and explain to them how the
information will be used. For example, get an idea
of the age of each person, how many children they
have, etc.
Make sure that the lunch break is free and that no
one lacks for anything.
20
THE COMMUNITY SHARES ITS IDEAS DURING PARTICIPATORY VIDEO DISCUSSION MEETINGS
“In practice, the one who has the last word is the lady’s husband; even if her brothers and sisters
would like for her to go to the health center, that depends on the husband. Although we might be in
the woman’s house, that is by choice; it must be the husband who gives the last word.” (Group of
Leaders, Totnicapán)
“…there are families that do want to, and there are others that don’t, even when the midwife insists
that they take her patient to the hospital; but if those involved don’t want to, it doesn’t happen.”
(Group of women, Totnicapán)
“…they came to look for me, since I have a car…” “…the husband came to tell us, but only when
his wife was at the point of death. And he said, do me a favor, take my wife to the hospital. We left
at 11 at night and arrived at 1 in the morning. And the doctor said, it is by the pure grace of God that
your wife did not die. Why did you wait until now to bring her in?” (Group of midwives, Zona
Reina, La Parroquia, Uspantán, Quiché)
“…what I saw in the film happened to me, because our husbands don’t stay home and you can’t
decide on your own.” (Group of women, Zona Reina, La Parroquia, Uspantán, Quiché)
21
IV. Appendices
APPENDIX 1
DISCUSSION GUIDE
THE DATA COLLECTION INSTRUMENT FOR PARTICIPATORY VIDEO DISCUSSION MEETINGS
INTRODUCING THE PROJECT AND THE TEAM The facilitator
Explains, in general terms, the objective of the
meeting and thanks the participants for coming.
Explains to the participants that the information
they share will be confidential and anonymous.
Explains the need to record the session to have a
“souvenir” of the meeting (he can offer, where
possible, to let them see the tape later).1 If possible,
he should ask their permission to make the tape,
assuring them once again of their anonymity and
confidentiality.
Explains to them that they will watch together a
couple of short videos that have been prepared for
the meeting, and that they will converse informally
about what each person thinks.
Asks them to interrupt him at any time if there is
anything that is not clear.
Introduces the other members of the team by name
and function (during the meeting). It is suggested
that their positions in the health care system not be
mentioned, to avoid bias.
Explains to them that they are going to begin with
a short exercise to get to know each other better.
1
It is very important to ensure the confidentiality and anonymity of the participants. To reassure them more concretely, the ideal would be for those of one region to meet with users of ANOTHER region than their own. Or, as we have agreed, that those who facilitate be people from the outside with good facilitation skills. Take care that the health workers who sometimes play the role of participating observers do not affect the outcome by their very presence.
22
ICE-BREAKER: To be chosen based on the characteristics of the
participants.
PART 1 Presentation of Video 1, followed by discussion.
The facilitator explains the process to the participants:
that he will show them part of a film which they will
discuss after seeing it.
Observation: watch whether the participants are
following the video attentively. Play it a second time
to make sure that all have seen and understood it from
beginning to end.
Video 1: Situation—emergency
Dramatization: a woman lies ill at home; the
person who is with her explains the woman’s
symptoms to another person, but none of them
know that these are warning signs. The midwife
arrives and states that in this case she can no
longer do anything. At the same time, a health
care provider arrives and insists that they take the
woman to the nearest health center. The husband
is not there, and the mother-in-law does not want
the woman to be taken to the health center. A
heated argument ensues among those who are
around the woman about what should be done.
You see the woman becoming weaker the whole
time, beginning to faint. The film cuts off here.
Video 1, discussion questions:
1. What does what you have just seen remind you of?
Have you experienced anything like this? Have
you heard of a case like this in your community?
2. What happens in the film? What problem does the
sick woman have? Who are the people arguing?
Why are they arguing?
3. In cases like this, what do people of your
community do? What does the woman do?
4. (If necessary, pick up the thread of the story to
help the participants remember). In your opinion,
what would happen next? When and how does the
family realize that the woman’s condition is
serious? Who are the ones who decide what to do?
What do they do (accept that she is going to die,
call in a traditional healer, take her to a health
center: church based, institutional, women’s
practice)? What happens to the sick woman at the
end (dies, survives)?
5. What problems will they have to face in trying to
save this lady’s life? What do they need to resolve
these problems? Who helps them? Who does not
help them (at various levels: family, community,
networks outside the community)? How hard is it
to resolve these problems?
6. If you were in this situation, what would you do?
7. What happens when a woman dies in the
community? Who are the children left with? Who
takes care of them? What happens to the husband?
23
PART II Presentation of Video 2, followed by discussion.
The facilitator explains to the participants that they
are going to see part of another film and discuss it
afterwards as before.
Observation: watch whether the participants are
following the video attentively. Play it a second time
to make sure that all have paid attention.
Video 2: hypothetical case in which it was decided to
take the lady to a health center (system financed with
state funds)
Dramatization: they arrive at the Health Service
and a service provider receives them saying why
did they wait so long. He is rude to the family and
to the midwife. The medical health care provider
on duty arrives (a young man). He does not speak
the language, and willingly explains what is wrong
with the patient. The interpreter has difficulty
translating because the doctor has used technical
terms that do not exist in the local language. The
doctor starts gathering the instruments needed for
the intervention, and everyone around begins to
mobilize—and the film cuts off.
Clip 2, discussion questions:
1. What did you see in the film? (have them explain
what is happening in the film: “What is
happening?”)
2. Has anything like this happened to you or to
someone you know? What happened?
3. What is it that most draws your attention in this
second film? What else do you see? Is it like this
in the health services that you know?
4. (If necessary, pick up the thread of the story to
help the participants remember). Do you
remember that we showed you only one part of the
film?
What do you think happened at the beginning (in
the part of the film that we did not show: when the
family arrives at the health center)?
4.1 (If the subject was not addressed in the
previous section) What did the family do to
get to the health center?
4.2 How was the family received at the health
center? How do you think that the health
workers treated the family, the lady, the
midwife? Did they let them ask questions?
How did they answer?
4.3 What did the health workers say to the
midwife?
5. And in the film clip that we saw, how do you think
the lady and her family feel in the place where she
is being treated? How does the place where the
lady is being treated seem to you? How do you
see this place? What is present and what is lacking
in the health center? What do you like and what
don’t you like?
24
6. If it were you in this situation, what would you do?
7. At the end of the film (which we haven’t seen
either because we cut it off before it got there)
what do you think happens to the lady (does the
lady live or die)?
8. What would be a happy ending to this second
film? What would be needed to get to this happy
ending?
9. How would you like to be treated in the health
centers?
PART III Dramatization followed by prioritization
Ask participants to divide up into two or three groups
(depending on the number of people). Each group
will act out how they would like the first story that we
just saw to end: from the moment the lady arrives at
the health center until her life is saved.
ATTENTION: We will begin with a dramatization of
the happy ending related to video 2 that we just
finished showing.
Dramatization of the gravely ill woman in the
health center: happy ending.
Each group presents its dramatization (taped as
they occur, like the rest of the meeting).
Dramatization 1, discussion, prioritization
Ask the participants to comment on the
dramatizations of the other group and their own
group:
Facilitator’s questions: How did you feel in the
health center? What did you find that you liked?
How did they treat you? How was the life of the
sick woman saved?
The facilitator draws pictures on the flipchart of
what the people are saying (this can also be done
by another member of the team who has an
aptitude for drawing).2 Facilitator and observer
write down the points mentioned by the
participants to complete the pictures on the
flipchart.
Once the two groups have completed their
comments, the facilitator poses the following
question (prioritization):
1. If you had to arrange everything you mentioned
in order of importance, what would come first?
2 Another possibility would be to use
a flannel board with figures prepared ahead of time. For this, you could see in the first meetings what
elements came out of the discussion with the participants and, on that basis, start making the flannel board, which would serve as a tool for discussion in subsequent meetings throughout the investigation and in other phases of the project, to the extent that they related to participatory research.
25
What next? Explore the reasons for this order of
priority. Arrange the components in the order of
priority indicated by the participants (write
numbers 1, 2, etc. on the list on the flipchart).
PART IV Dramatization followed by community mapping
Ask participants to divide up into two or three groups
(depending on the number of people). Each group
will act out how they would like the first story that
theyjust saw together to end (Video 1): from the time
the lady falls ill until it is decided what to do. Explain
to them that the dramatization or presentation must
show how the community is organized to deal with a
serious case (emergency in the community): What do
they decide to do? When do they make the decision?
How do they manage to get the woman out of her
house to save her life? What helps them? Who helps
them?
Dramatization of an emergency in the community:
happy ending.
Each group presents its dramatization (taped as
they occur, like the rest of the meeting).
Dramatization 2, discussion: mapping
Ask the participants to comment on the
dramatizations of the other group and their own
group.
Facilitator’s questions:
1. Who can help bring about these happy endings?
For example, to take the woman to a health center
where they can save her life? Who can help make
the decision in time? Who can help with
transportation? Who can inform other members of
the community and the health service of the
emergency?
The facilitator draws figures on the flipchart
representing these players.
2. Where are these people in the community? Near
the home? Far from the home? What can be done
to locate them? Is it possible to speak with them?
The facilitator, using the information supplied by the
participants, draws a map of the community on which
can be placed the key people who can help families in
case of emergency: local institutional authority, local
traditional authority, traditional health care system,
neighbors, etc. Showing the map to participants, the
facilitator verifies that his drawing corresponds to
3 You might also consider making a flannel board, as in the previous exercise.
26
what they said, and poses a final question to the
group:
3. What can the community do to help in emergency
cases? Can we all work together to save lives?
Conclude the meeting by:
Explaining that the objective is really to work with the
community to improve health services, to help them
prevent health problems, and support them in dealing
with emergencies in order to save lives. Reiterate that
we are engaged in a long term process, and this is
only the beginning. Thank them for their participation
and invite them to make their final comments (if they
have anything to add). Then conclude the
conversation by explaining what the follow-up will
be. In doing this, it is suggested that you reiterate that
this is the beginning of a common endeavor; that we
will be returning to the communities to continue the
process.
NOTE: As follow-up to this investigation, you might
hold a debriefing session with the community on the
results of the participatory research, in the form of
developing local emergency plans (the name to be
given to this type of initiative will come out of the
groups themselves). We should not forget to involve
(in one way or another) the people who agreed to
participate in the discussion and in the other phases of
the project.
27
APPENDIX 2
A FEW TIPS
Basic Rules: I. Practice “active listening”
That means, listen in a way that communicates
respect, interest, and empathy. These attitudes
can be conveyed verbally and non verbally.
How can I verbally communicate to the person
that I am listening to him/her?
How can I non verbally communicate to the
person that I am listening to him/her?
II. Use language that is simple and clear No professional jargon
Use terms that the participants understand
Culturally appropriate language
Some techniques for clarifying answers or probing into what a person is saying:
1. Paraphrasing: that is, repeating in other words
what the person has just said
Example:
2. Posing follow-up or “checking” questions: this
is a KEY technique in this kind of
investigation. It is used to understand the
reasons for people’s behaviors, attitudes, or
motivations. It is a question that CLARIFIES
an answer given by someone. It helps us to
PROBE a point that we consider important.
How to do it:
Give the person time to keep on talking (wait in
silence for a short time after the person has
answered).
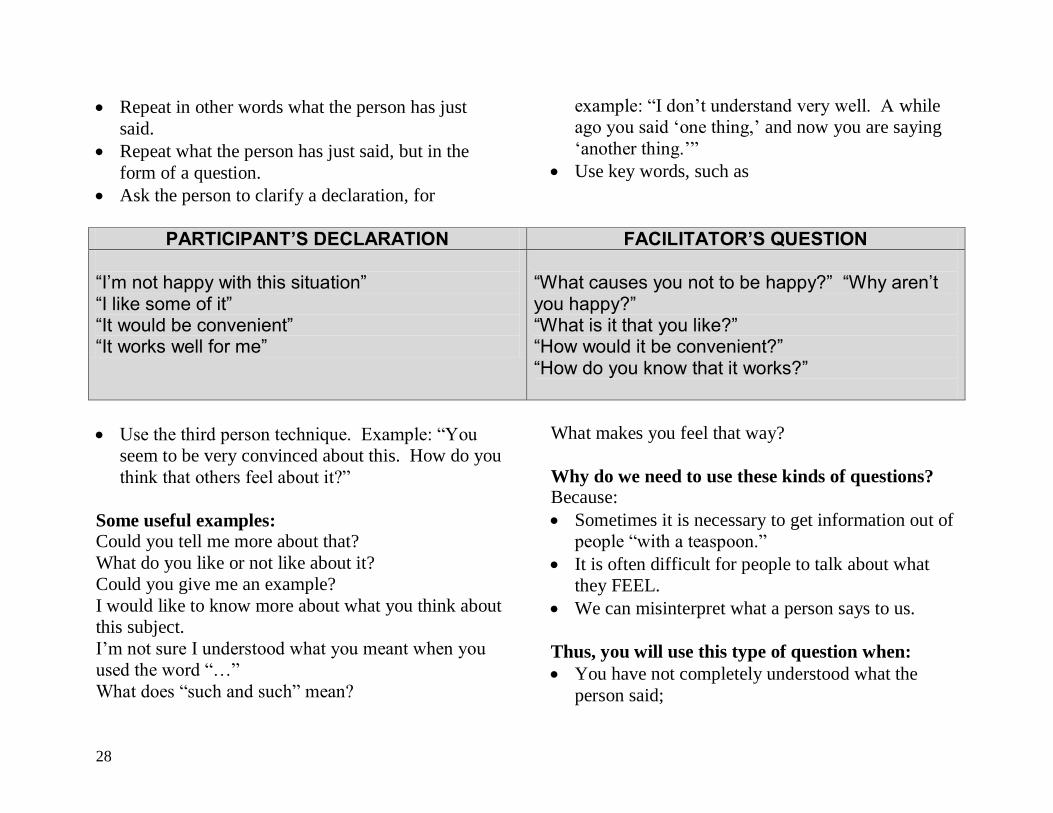
28
Repeat in other words what the person has just
said.
Repeat what the person has just said, but in the
form of a question.
Ask the person to clarify a declaration, for
example: “I don’t understand very well. A while
ago you said ‘one thing,’ and now you are saying
‘another thing.’”
Use key words, such as
PARTICIPANT’S DECLARATION FACILITATOR’S QUESTION
“I’m not happy with this situation” “I like some of it” “It would be convenient” “It works well for me”
“What causes you not to be happy?” “Why aren’t you happy?” “What is it that you like?” “How would it be convenient?” “How do you know that it works?”
Use the third person technique. Example: “You
seem to be very convinced about this. How do you
think that others feel about it?”
Some useful examples: Could you tell me more about that?
What do you like or not like about it?
Could you give me an example?
I would like to know more about what you think about
this subject.
I’m not sure I understood what you meant when you
used the word “…”
What does “such and such” mean?
What makes you feel that way?
Why do we need to use these kinds of questions? Because:
Sometimes it is necessary to get information out of
people “with a teaspoon.”
It is often difficult for people to talk about what
they FEEL.
We can misinterpret what a person says to us.
Thus, you will use this type of question when:
You have not completely understood what the
person said;
29
You want more details or specific examples;
You are trying to uncover feelings and
motivations;
You are not familiar with the terms that the person
is using;
You think the person is saying only part of what he
is thinking.
3. Giving “positive feedback”
That is, praise or encourage the person
concerning what he says he has done. This
helps people feel more comfortable with the
facilitator (who is not making value judgments
and not “criticizing” the person), and thus
encourages them to give more information.
This technique can also help reinforce a desired
behavior. Sometimes this is difficult to do
because the person could be describing a
behavior we disapprove of or consider “bad.”
Example: a man decided not to take his wife to
the health center but then realized that it would
have been better to have taken her. The
facilitator can say to him, “It’s good that you
have realized it would have been better to take
her. What made you change your mind? What
would you do now?”
Other advice:
4. Avoid questions that lead to “yes” or “no”
answers, that is, closed questions.
5. Rephrase questions when necessary to ensure
understanding and cultural adaptation.
6. Don’t give the impression that you are testing the
participants’ knowledge.
7. Put yourself in the participants’ place to see if you
would feel threatened by a particular question or
the way it is formulated.
8. Don’t guess any answer. What you think might
not coincide with what the other person is
thinking.
9. Don’t include ANSWERS in your questions.
10. If people are speaking in a “neutral” manner about
a subject, or if the participants are not talking, you
can sometimes play the “devil’s advocate,” always
being careful not to obstruct the process of
communication.
11. Remember that you are leading a group discussion
and not individual interviews. Refer the comments
and answers of one participant to the group to
encourage other comments. Connect the answers
of different participants to further explore a
subject.
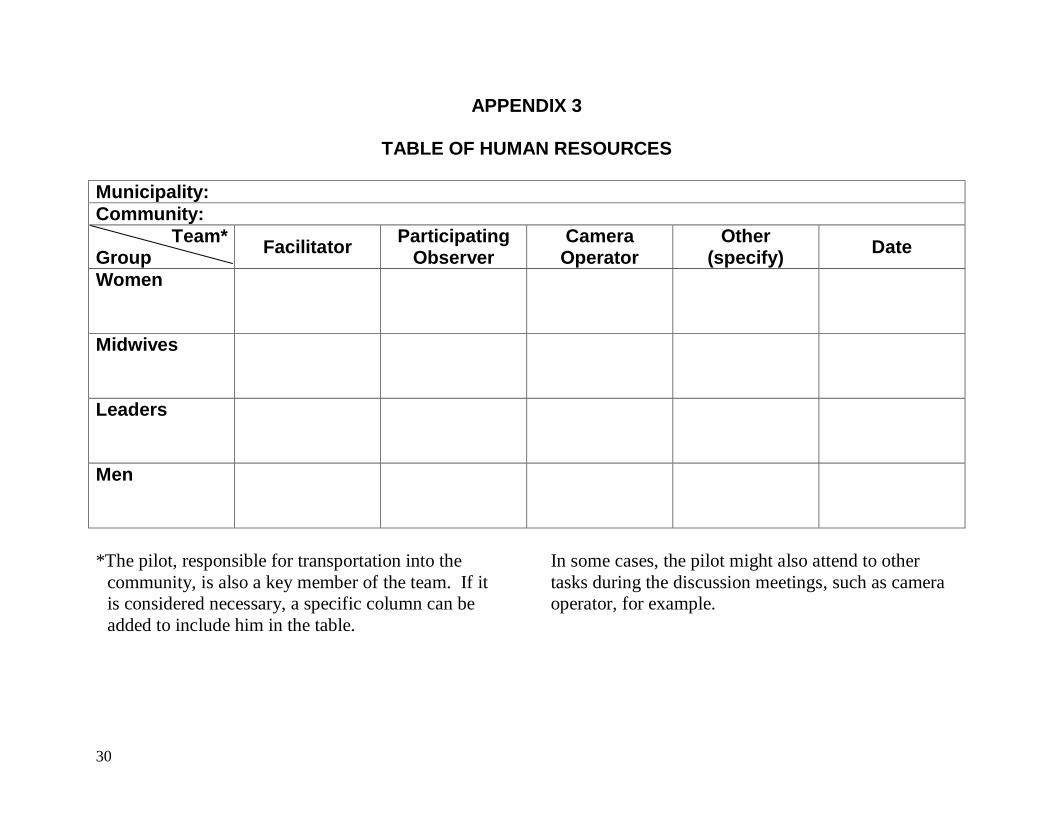
30
APPENDIX 3
TABLE OF HUMAN RESOURCES
Municipality:
Community:
Team* Group
Facilitator Participating
Observer Camera
Operator Other
(specify) Date
Women
Midwives
Leaders
Men
*The pilot, responsible for transportation into the
community, is also a key member of the team. If it
is considered necessary, a specific column can be
added to include him in the table.
In some cases, the pilot might also attend to other
tasks during the discussion meetings, such as camera
operator, for example.
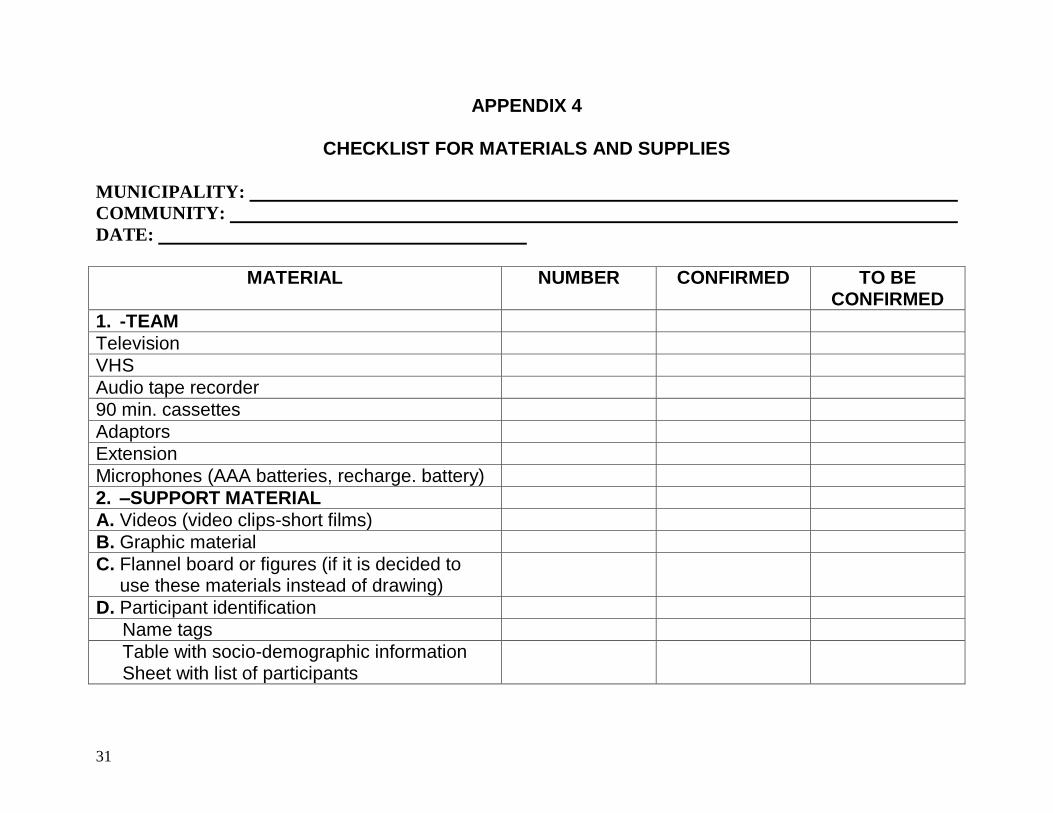
31
APPENDIX 4
CHECKLIST FOR MATERIALS AND SUPPLIES
MUNICIPALITY:
COMMUNITY:
DATE:
MATERIAL NUMBER CONFIRMED TO BE CONFIRMED
1. -TEAM
Television
VHS
Audio tape recorder
90 min. cassettes
Adaptors
Extension
Microphones (AAA batteries, recharge. battery)
2. –SUPPORT MATERIAL
A. Videos (video clips-short films)
B. Graphic material
C. Flannel board or figures (if it is decided to use these materials instead of drawing)
D. Participant identification
Name tags
Table with socio-demographic information Sheet with list of participants
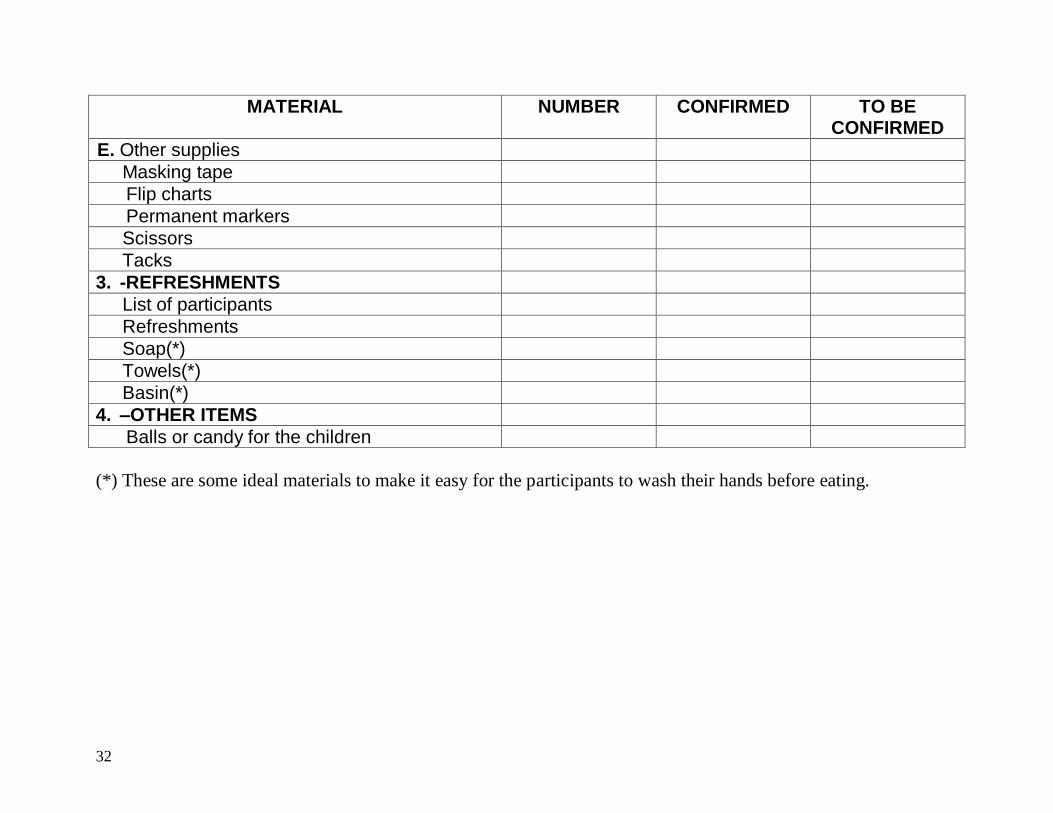
32
MATERIAL NUMBER CONFIRMED TO BE CONFIRMED
E. Other supplies
Masking tape
Flip charts
Permanent markers
Scissors
Tacks
3. -REFRESHMENTS
List of participants
Refreshments
Soap(*)
Towels(*)
Basin(*)
4. –OTHER ITEMS
Balls or candy for the children
(*) These are some ideal materials to make it easy for the participants to wash their hands before eating.
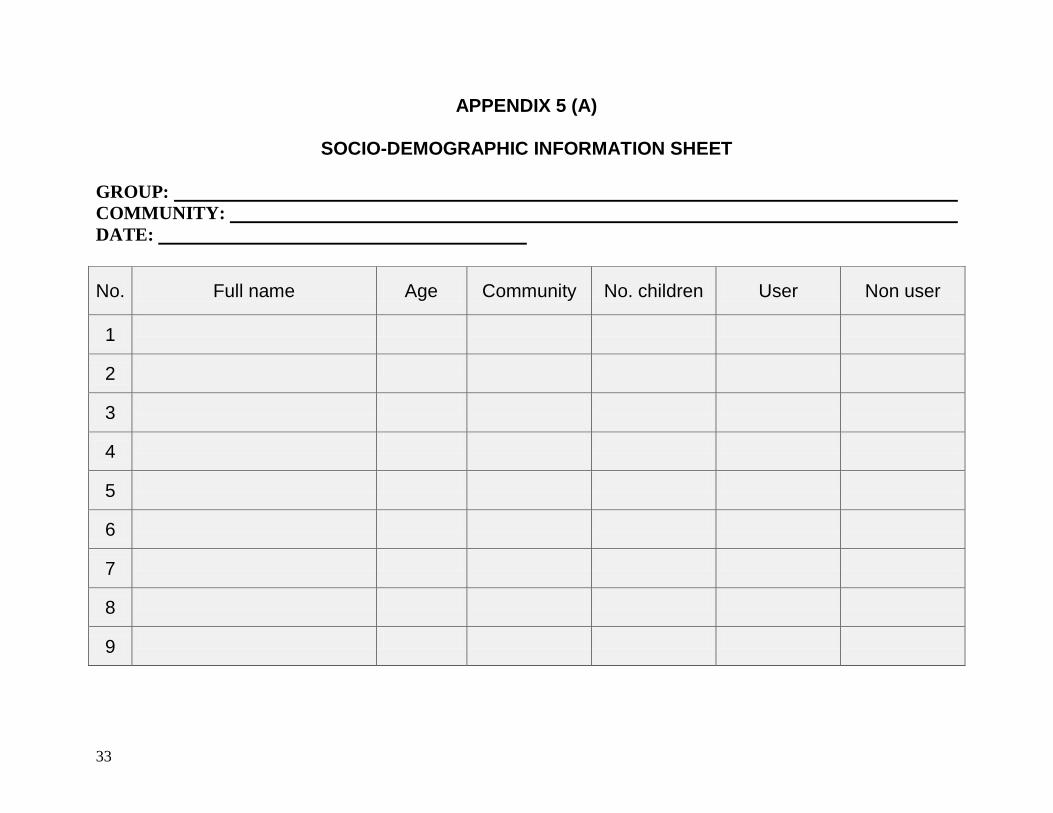
33
APPENDIX 5 (A)
SOCIO-DEMOGRAPHIC INFORMATION SHEET
GROUP:
COMMUNITY:
DATE:
No. Full name Age Community No. children User Non user
1
2
3
4
5
6
7
8
9
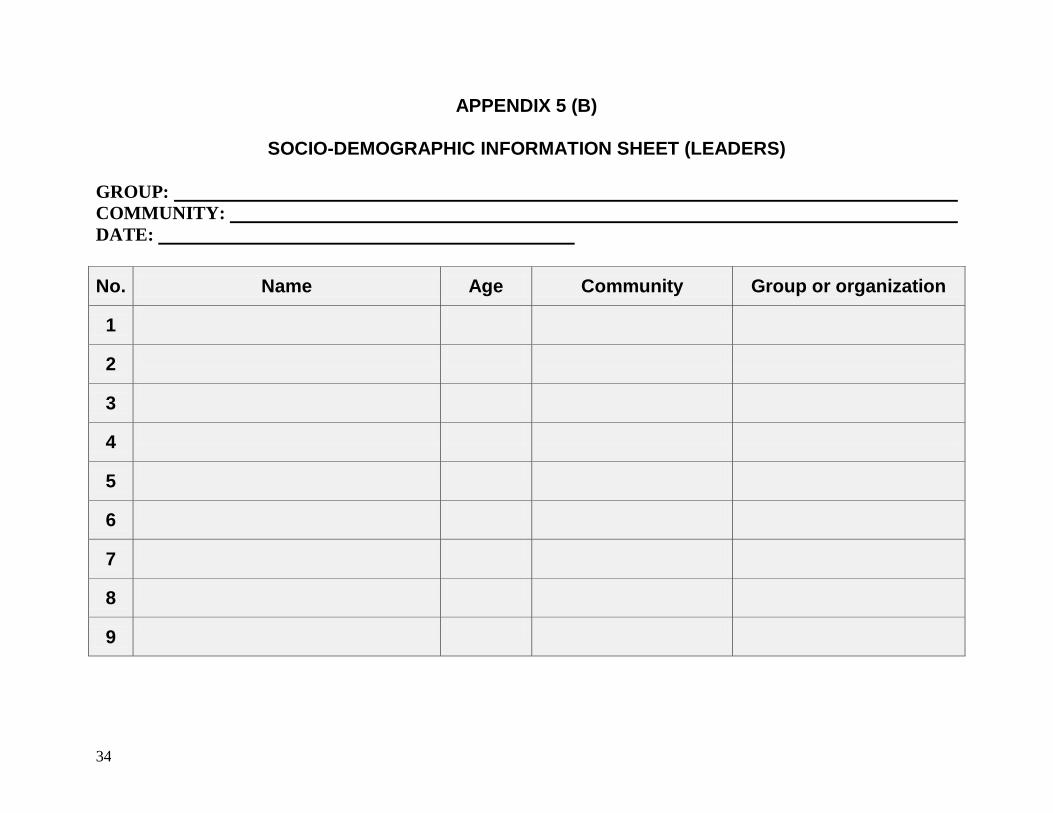
34
APPENDIX 5 (B)
SOCIO-DEMOGRAPHIC INFORMATION SHEET (LEADERS)
GROUP:
COMMUNITY:
DATE:
No. Name Age Community Group or organization
1
2
3
4
5
6
7
8
9
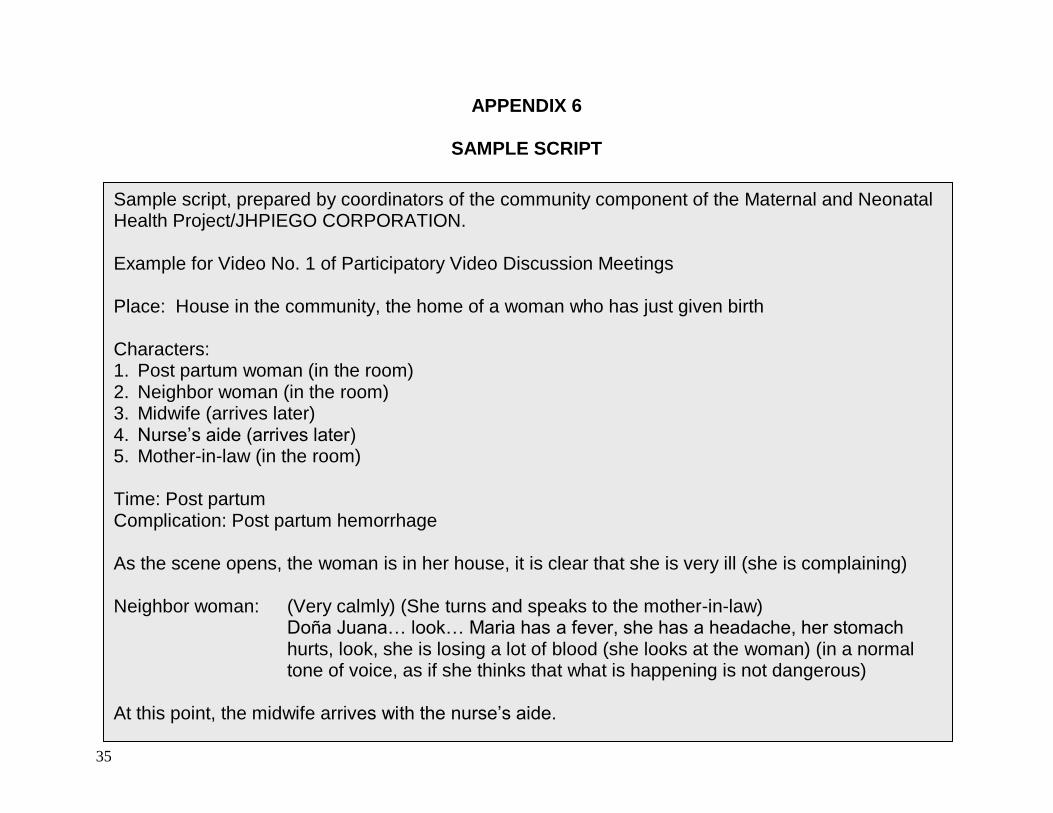
35
APPENDIX 6
SAMPLE SCRIPT
Sample script, prepared by coordinators of the community component of the Maternal and Neonatal Health Project/JHPIEGO CORPORATION. Example for Video No. 1 of Participatory Video Discussion Meetings Place: House in the community, the home of a woman who has just given birth Characters: 1. Post partum woman (in the room) 2. Neighbor woman (in the room) 3. Midwife (arrives later) 4. Nurse’s aide (arrives later) 5. Mother-in-law (in the room) Time: Post partum Complication: Post partum hemorrhage As the scene opens, the woman is in her house, it is clear that she is very ill (she is complaining) Neighbor woman:
(Very calmly) (She turns and speaks to the mother-in-law) Doña Juana… look… Maria has a fever, she has a headache, her stomach hurts, look, she is losing a lot of blood (she looks at the woman) (in a normal tone of voice, as if she thinks that what is happening is not dangerous)
At this point, the midwife arrives with the nurse’s aide.
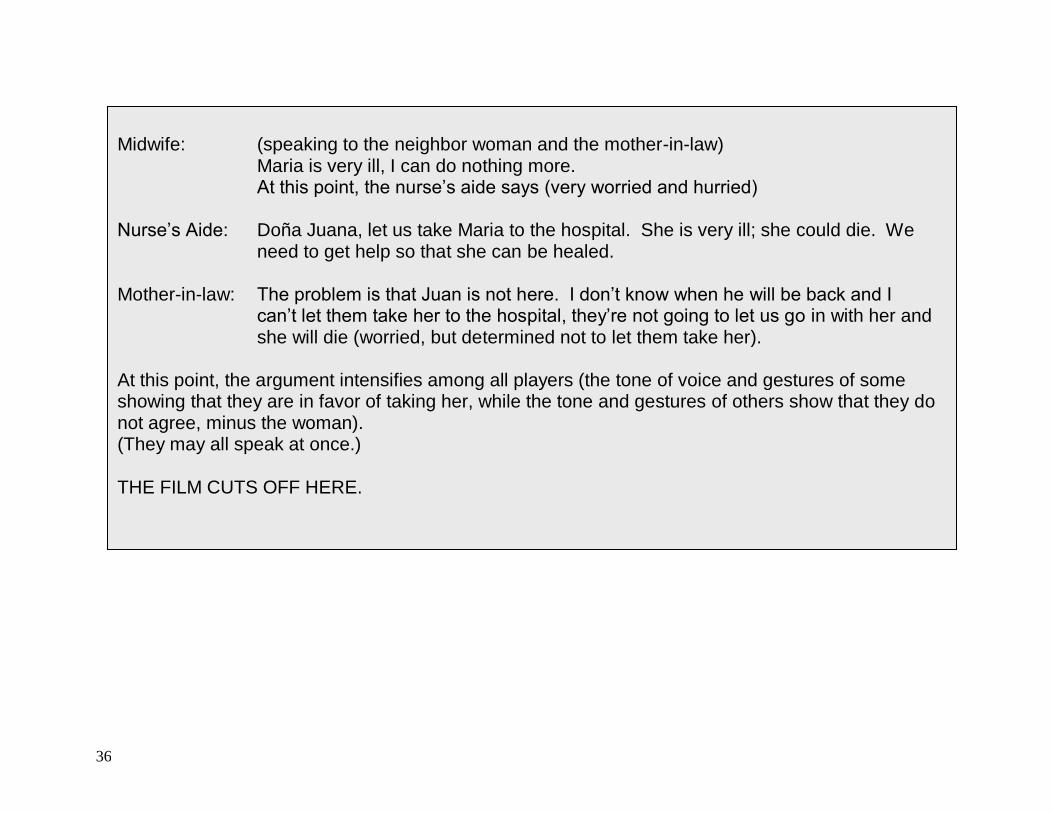
36
Midwife: (speaking to the neighbor woman and the mother-in-law)
Maria is very ill, I can do nothing more. At this point, the nurse’s aide says (very worried and hurried)
Nurse’s Aide:
Doña Juana, let us take Maria to the hospital. She is very ill; she could die. We need to get help so that she can be healed.
Mother-in-law:
The problem is that Juan is not here. I don’t know when he will be back and I can’t let them take her to the hospital, they’re not going to let us go in with her and she will die (worried, but determined not to let them take her).
At this point, the argument intensifies among all players (the tone of voice and gestures of some showing that they are in favor of taking her, while the tone and gestures of others show that they do not agree, minus the woman). (They may all speak at once.) THE FILM CUTS OFF HERE.
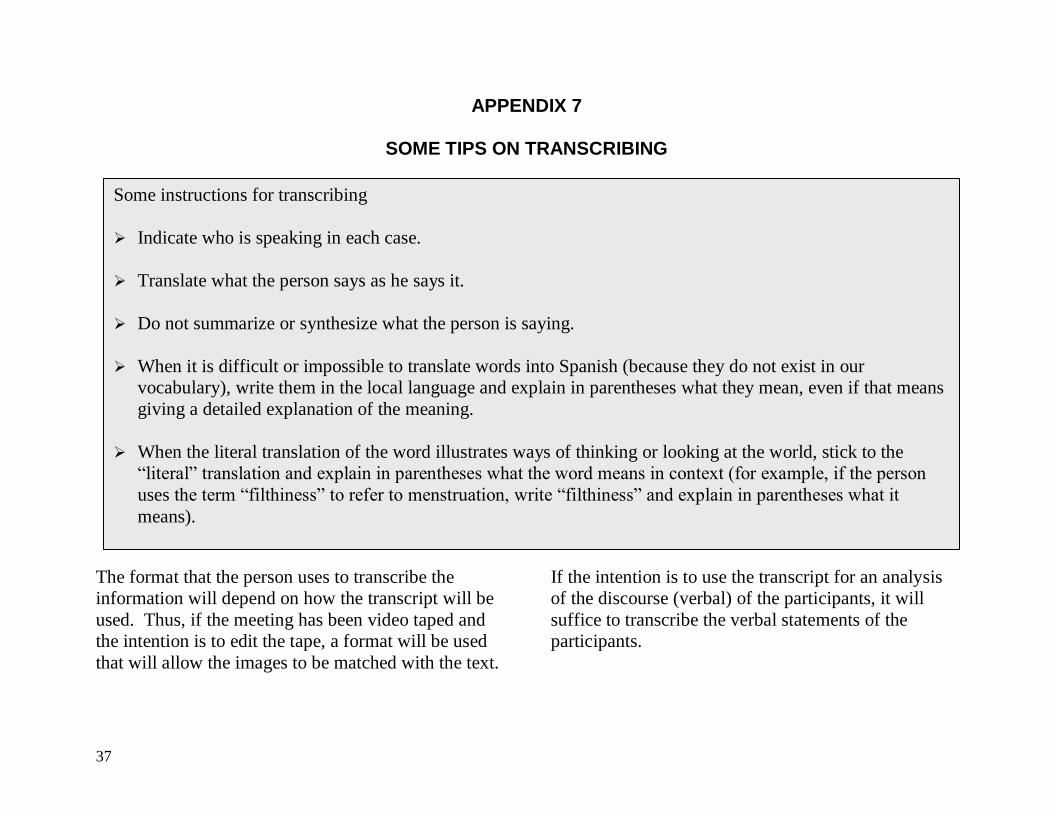
37
APPENDIX 7
SOME TIPS ON TRANSCRIBING
The format that the person uses to transcribe the
information will depend on how the transcript will be
used. Thus, if the meeting has been video taped and
the intention is to edit the tape, a format will be used
that will allow the images to be matched with the text.
If the intention is to use the transcript for an analysis
of the discourse (verbal) of the participants, it will
suffice to transcribe the verbal statements of the
participants.
Some instructions for transcribing
Indicate who is speaking in each case.
Translate what the person says as he says it.
Do not summarize or synthesize what the person is saying.
When it is difficult or impossible to translate words into Spanish (because they do not exist in our
vocabulary), write them in the local language and explain in parentheses what they mean, even if that means
giving a detailed explanation of the meaning.
When the literal translation of the word illustrates ways of thinking or looking at the world, stick to the
“literal” translation and explain in parentheses what the word means in context (for example, if the person
uses the term “filthiness” to refer to menstruation, write “filthiness” and explain in parentheses what it
means).
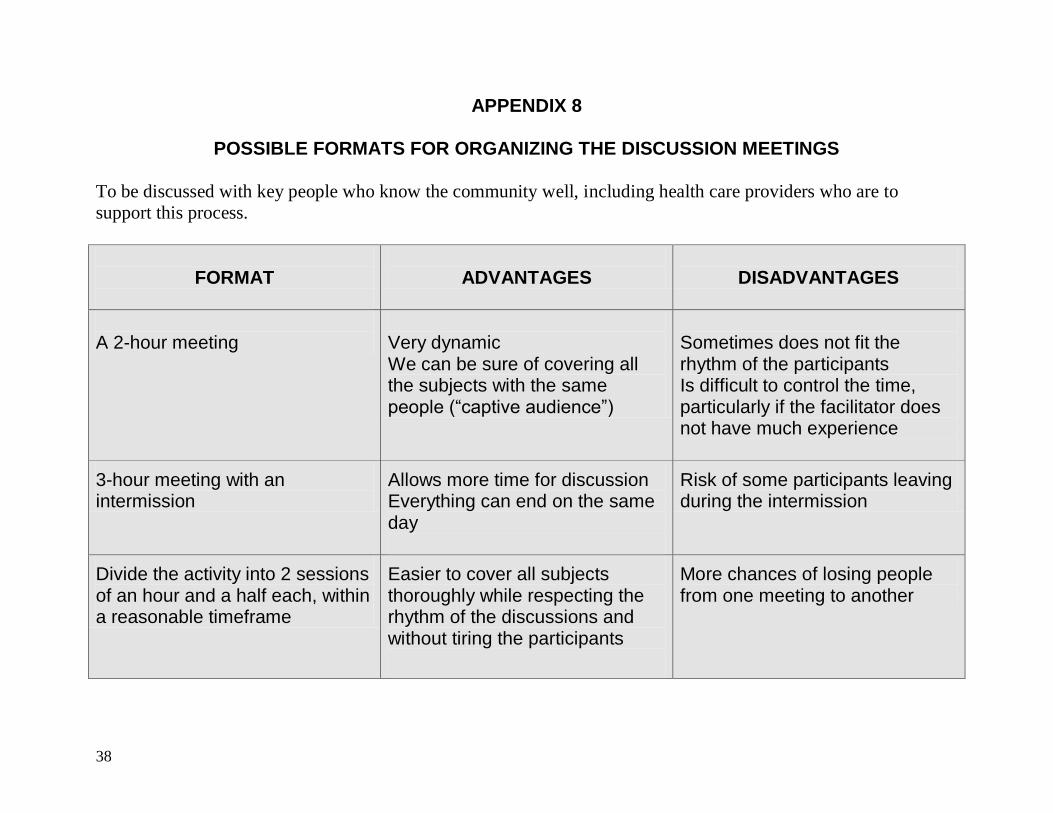
38
APPENDIX 8
POSSIBLE FORMATS FOR ORGANIZING THE DISCUSSION MEETINGS
To be discussed with key people who know the community well, including health care providers who are to
support this process.
FORMAT
ADVANTAGES
DISADVANTAGES
A 2-hour meeting
Very dynamic We can be sure of covering all the subjects with the same people (“captive audience”)
Sometimes does not fit the rhythm of the participants Is difficult to control the time, particularly if the facilitator does not have much experience
3-hour meeting with an intermission
Allows more time for discussion Everything can end on the same day
Risk of some participants leaving during the intermission
Divide the activity into 2 sessions of an hour and a half each, within a reasonable timeframe
Easier to cover all subjects thoroughly while respecting the rhythm of the discussions and without tiring the participants
More chances of losing people from one meeting to another
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Method of Participatory Research and Action Using Video Discussion Meetings User’s Manual
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Thank you for your support!
Educational Producers and Evaluators Marcela Tapia, Patricia Poppe, Robert Ainslie
Adaptation for Guatemala
Human Resources Responsible for the Investigation
Technical Reviewers Ministry of Public Health and Social Welfare of Guatemala
National Program for Reproductive Health, Executive
Board, USAID
Collaborators Technical and Administrative Personnel of the Maternal and
Neonatal Health Project
Regional Health Offices: El Quiché, Totonicapán and Sololá
Midwives of Cantel, Quetzaltenango
Midwives of Santa Catarina Palopó
Groups of women, men, leaders, midwives, providers
(purpose of the investigation)
Photographs
Graphic Design and Diagrams
Note: It is important to indicate that in this document the masculine gender has been used on most occasions in which the text might refer to either
men or women. This measure has been adopted with the sole intention of simplifying the text, without any suggestion of preference.
This publication was made possible with the support of the Agency for International Development (AID), under Contract No. C.A. HRN-A-0098-
00043-00. The opinions expressed are those of the authors and do not necessarily reflect the point of view of AID.
Guatemala, January 2004
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
TABLE OF CONTENTS
INTRODUCTION
PART I:
THE RAW MATERIAL 1. The various change agents as resources
2. Visions of the world and visions of health
3. Starting from reality: working with existing organizations and
initiatives
4. Towards gender inclusion
5. From soliciting help to empowerment
PART II:
THE INSTRUMENT
PARTICIPATORY VIDEO DISCUSSION MEETINGS
1. Objectives of participatory research
2. The instrument: Participatory video discussion meetings and how to use them
Step #1. Creating a good relationship
Step #2. Introducing the facilitating team and the participants and
presenting the project
Step #3. Creating a friendly atmosphere: Ice-breaking exercise
Step #4. Presenting stories from life: Videos 1 and 2
Step #5. Prioritizing the attributes of quality that a health center
should have from the community’s perspective
Step #6. Conducting community mapping
Step #7. Wrapping up the meeting and continuing the collective
action
3. The facilitating team for participatory video discussion meetings 3.1 The facilitating team
3.2 The qualities and skills of the facilitating team
3.3 Practical tips for leading group discussions
4. The participants from the community invited to the participatory
video encounters
4.1 The process of inviting the participants
4.2 Criteria for selecting participants
5. Planning ahead and logistics 5.1 Resource management
5.2 Time management
5.3 Space management
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
6. Processing the information
6.1 Processing the experience
6.2 Analyzing the discussion meetings
7. Use of the instrument within the process
PART III:
THE “KNOTS”
1. Recognition and incentives
2. Giving back to the community
3. Tying the knots
PART IV:
APPENDICES
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
INTRODUCTION
This manual has been designed to lead the reader step by
step through the application of a participatory research tool
in a maternal and neonatal health project. This method of
investigation (instrument or tool) is called the “participatory
video discussion meeting.” A participatory video discussion
meeting is a meeting for discussion in which testimonies,
stories and images on video are used to stimulate dialogue.
The “tapestry of knots” we know today reflects the
components and characteristics of the participatory research
process that includes this particular method of investigation.
We have chosen this analogy because the “tapestry of knots”
is an “indigenous” cultural element, that is, it is created from
the community itself and represents it. The knots represent
at once permanence and change, since every tradition has a
past (has history), and at the same time has a future and
evolves with time. The knots are, therefore, not only outputs
but also processes since they are continually created and
recreated over time. Moreover, the knots symbolize
community, mutual support, the formation of networks, and
solidarity.
This manual proposes to “tie knots” for healthy motherhood
through a process that involves learning, reflection and
action. The first part of the manual, “The Raw Material,”
highlights the essential and most valuable resource for this
work—the human element, that is, the community, health
care providers, and external agents working together to
create and strengthen the “knots” for improved health. The
second part, entitled “The Instrument,” contains a detailed
description with precise instructions for using “participatory
video discussion meetings” as a method/tool of participatory
research. The third part, “The Knots,” presents in detail the
process of dialogue and community participation that is the
very essence of the process of participatory research.
Parts II and III are the most condensed sections of the
manual, but essential to contextualize and help the reader
understand the principles that guide the use of the
instrument. Part II of the manual is the most extensive,
since it contains detailed instructions that will allow the
reader to take ownership of the instrument step by step, and
use it to forge bonds with the community. To complete the
manual, we have included in the appendices section various
documents that the reader can photocopy when needed.
To gain a more complete vision of the participatory research
process, and to use the instrument in harmony with the
objectives of mutual learning established within the
framework of this project, it is recommended to read this
manual as a whole. Although each part of the manual
addresses different themes and provides elements for
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
reflection that can be used separately, the three parts
complement each other and represent, in effect, a whole
within the process of participatory research.
The commitment of this manual corresponds to the ultimate
goal that inspired the development of the instrument, that is,
to “tie ever stronger knots” to support life and the need to
take action within the community when it and its families
are confronted with cases of obstetrical emergency. It is one
attempt to contribute to social change, to make long term
commitments and actions, and to strengthen existing social
networks in the community.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
PART I: THE RAW MATERIAL
Every process of participatory research for social change
should focus on the potential existing in the communities.
Without denying the lack of resources and infrastructure that
afflict communities, it is essential to recognize existing
resources as a point of departure for working in the
community. Along these lines, beyond the material
resources available, we need to highlight the great human
potential existing in each community. Added to this are the
working groups and external agents committed to supporting
the community in its own process of social change. The
different paragraphs in this first part of the manual suggest
themes to guide your thinking regarding the valuable “raw
material” existing in communities, and the necessity and
relevance of building on what is there, on the strengths and
potential of each community. Farther along, some models
are proposed to guide the reader in the use and adaptation of
this manual, taking into account the need to include the
community’s most vulnerable groups in the process of
participatory research. We will look at:
1. The various change agents as resources A project or collective endeavor does not get started by
spontaneous generation. Thus, the role of community
“change agents” and of external catalysts is fundamental
during the startup of any project. Community “change
agents” are people who have influence over others and who
are capable of generating change within the community. It
is often they who become aware of the existence of a
problem and begin to mobilize the community in search of a
solution. Those who come from outside to support the
community are called “external catalysts.” Their role is to
facilitate the process of change in the community, using
tools such as those suggested in this manual. Sometimes
they are the ones who suggest that the community work on a
specific problem that has been identified, through research
studies, for example. Their role as facilitators is not to
impose an agenda on the community, but rather to work with
the community to help it:
identify and become aware of the problem, and
decide what should be done to resolve it.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
The facilitator orients the community and enters into a
dialogue with it in order to take appropriate action, without
unilaterally imposing his point of view. Together, the
community change agents and the external catalysts can help
the community identify a problem and establish common
goals for solving it.
There are sectors of the community particularly affected by
the problem that is being addressed, and it is essential to
involve them in the process: in this case, maternal and
neonatal health issues directly affect women of reproductive
age and their midwives. The heads of families are another
key group, since the actions taken in cases of emergency
often depend on them. When conducting participatory
research, it is important to take into account the real or
potential role that each of these figures plays in the
community. Special consideration should be paid to the
question of how to involve groups that are usually absent
from the arena of decision making in the community.
There is no one, predetermined model for initiating the
process of change within a community with the help of
participatory research. The characteristics that the
experiment assumes will depend on the people involved, the
existing means of organization, and the surroundings. In
every case, what is important in the process is to turn the
focus of the endeavor away from the deficiencies and
shortcomings of the community. Instead, we propose to
focus the intervention on the strengths of the community
and the specific players involved. It is important to be
aware that the role of each of the following:
women
husbands
midwives
leaders
community change agents
external catalysts
authorities
is essential, and that what each one brings from his/her
position to the participatory research should be appreciated
and respected.
Using the strengths of the players involved as a
starting point helps to strengthen the bonds
between the community and the external catalysts.
Both parties will be joined by the conviction that
they can move forward together:
reappropriating the past
focusing on the present, and
incorporating in their actions a vision of the
future.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
2. Visions of the world and visions of health
Many development projects have failed in the past because
they did not take into account the point of view of the
interested parties and tried to impose patterns of behavior
that were foreign to the local culture. The focus on
community strengths goes hand in hand with the recognition
of the cultural differences between the external catalysts and
the community. The recognition of these differences also
implies the need to understand how “the Other,” the one
who is different from me, conceives his own problems and
his reality. Without needing to blindly accept traditions that
might be harmful to the people’s health, it is important to
know what health means to the community, and what are its
priorities, values, and traditions. An open exchange with the
community about its customs and beliefs can lead us to
discover traditional practices that will need to be modified as
well as customs that should be reinforced and integrated into
the practice of western medicine.
In the context of this participatory research activity, it is
particularly important to know the community’s point of
view concerning health services, or what we call “the
attributes of quality” with regard to health care. The
“attributes of quality” are the characteristics of health care
services that determine whether or not the users appreciate
them. For example, a person might complain that she is
made to wait a long time before being seen at the health
center. In this case, the quality attribute is “rapid attention.”
Another person may say that she is going to the health center
because she knows that the staff who see her there will treat
her well. In this case, the quality attribute is “good
treatment.” In the first case, the service lacked the attribute
in question, while in the second, the service possessed the
attribute or characteristic that was important to the user. The
fact that a health center does or does not have a certain
attribute may lead the user to choose one service over
another, or simply not use any services. This is why it is
important to know the attributes of quality from the
community’s point of view.
The process of participatory research proposes a perspective
from within, that is, that starts with the community’s point of
view. Listening to the community’s point of view will help
to better understand the community’s ways of being and
doing. This means that we are going to listen to what people
are telling us and learn from them and with them. We are
not going to be empowerers, but rather facilitators who go to
the communities to learn the point of view of their members
concerning health and health services. This perspective
from within will help, for example, in the case we are
looking at, to better understand what people like about their
services and what could be improved to make the people
satisfied with them. The perspective from within will also
help better understand how members of the community deal
with obstetric emergencies and what causes them to act in
one way or another. This will make it possible to develop
activities adapted to the context, that take into account the
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
point of view and the reality (psychosocial, socio-economic
and cultural) of those involved.
In holding conversations with members of the community,
the most important thing is to clearly distinguish between
what “I” think and what “they” think. We must strive to put
aside all the ideas we have about the community in order to
listen to the people with fresh ears and be able to understand
what they are telling us.
In an intercultural exchange, the act of opening your eyes to
the community’s vision of the world goes hand in hand with
an awareness of your own prejudices, values and cultural
norms.
3. Starting from reality: working with existing initiatives and organizations
The approach used in this manual implies starting from the
reality that exists instead of trying to impose an agenda or
program that is not relevant to the community. To the extent
possible, you should try to integrate participatory research
into the initiatives and areas of intervention of the
organizations already working in the community.
For example, the project of building a birthing center or
community maternity clinic might be the motor that drives
the process of participatory research in the community. In
the same way, you must be aware at all times that the
process begun in the community should be given back to the
community to which it belongs, and that the best ways to do
this are often through the health committees or groups
already working in the community. On many occasions,
when it comes to maternal and neonatal health, you may
consider expanding and/or strengthening the fundraising
activities that are already carried out in a particular way in
the community. For example, there are communities in
which funds are collected for cases of death or emergency.
Instead of proposing something new, you can improve the
organization, planning and management of these activities as
part of a “Community Emergency Plan,” a name that could
The community’s experiences in:
Project development
Community organizations
Collective management (e.g.,
fundraising)
are part of the community’s baggage that should
be taken into account during the participatory
research.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
well be changed according to what the community decides.
When you start with what is already there, you are better
adapted to your surroundings. The process of participatory
research can help to both identify and improve on
experiments already taking place in the community. This is
important because:
You need to be attentive to the opportunities for
mobilization and participation existing in the community
You need to get involved in the existing nuclei of
community organization
You need to improve what already exists instead of
“reinventing the wheel”
It is also important to take into consideration the calendar
of agricultural activities and the agendas particular to
each community in order to collaborate more effectively
with them. For example, it is no use to try to organize
meetings with men at harvest time when everyone is
outside the community. Nor would it be useful to
organize meetings to talk about the health of the mother
and the newborn when the community is in a week of
celebration or has some other urgent problem to deal with
(for example, a flood).
It must not be forgotten that the other key players in the
process of participatory research are the health care
providers. The same thing that we advocate for the
community also applies to the service providers involved in
this intervention. For example, it would not be realistic to
think that the nurses or social workers could put aside their
work in the clinics to dedicate themselves completely to
facilitating “participatory video discussion meetings.”
Those who might be interested in doing it will need to: 1)
plan their work in such a way that these discussion meetings
complement it; 2) analyze to what extent they can assume
the functions of the facilitating team for the discussion
meetings and have the participants feel free to “tell it like it
is” and not how it “ought to be.” At the same time, we
know that some of the activities planned within the
participatory research can reinforce the operations of the
health care providers. For example, the “community
mapping” to take place during and after the participatory
video encounters is a tool for locating the resources
available in cases of emergency in the community, which
reinforces one of the functions of the community facilitators
in the emergency rooms. Since we know that community
facilitators need to make maps of the communities, the tool
of community mapping within the context of participatory
research will necessarily help them in this task. It is a matter
of identifying in the field the best way to involve health care
workers in participatory research activities from where they
are.
The use of participatory video discussion meetings as a tool
of participatory research must be adapted to the reality of the
community and of the service providers, starting with what
is already there in order to strengthen it. The very process of
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
reflection and action will lead to the collective formulation
of proposals for effecting changes that will benefit everyone.
4. Towards gender inclusion
Starting from reality does not mean accepting the status quo
(things as they are) and the unequal power relationships that
might exist in a community. It is about including and not
excluding and, within vulnerable groups, women are often
excluded from decision making, even in matters that directly
affect them, such as death in childbirth. Despite the
preponderant role that women play in the community as a
whole and in health matters in particular, they are often
absent from the health committees, the pro-maternity
committees, and other nuclei of community organization.
However, when given the opportunity to participate, they are
capable of articulating their ideas and making suggestions
that can benefit the committees as well as the community as
a whole.1 It is necessary to support the participation of
women at every level and at specific times in the
participatory research, including active participation in the
health and pro-maternity committees. This can be achieved
through specific measures, such as:
1 We were able to confirm this during participatory video discussion meetings
that were carried out in Zona Reina.
Providing incentives for participation in the participatory
video discussion meetings by women in the community
who are not used to participating
Discussing with the community how women leaders,
midwives, and community women in general might be
included in the committees that make important health
decisions.
The external catalysts in the participatory research can play
an important role in this regard, since they bring a different
point of view (that is, that women can and should
participate), and are able to influence the opinions of
members and leaders in the community.
5. From soliciting help to empowerment It may happen that, when a team comes into a community,
its members and representatives ask the team to solve the
problems that afflict it. The community may also express:
Its feeling of impotence when faced with the conditions
that confront it.
Its feeling of helplessness to solve its problems.
Its belief that only the people coming in from outside are
capable of changing the situation.
Often the members of the community lose sight of what they
are doing day by day to improve their situation and that of
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
their children. They have an image of themselves centered
more on what they lack than on their strengths. And the
same thing often happens with some of the people from
outside the community, who see above all its shortcomings
and not its strengths. Participatory research seeks precisely
to reverse this situation and bring to light the strengths and
the worth of the community’s own initiatives.
We should not deny the community’s concrete need for
help; on the contrary, we should be attentive to it. The thing
to avoid is falling into “paternalism” or “aidism” that
consists of doing things for the community instead of doing
them with it. We must remember that the mutual learning
process we have begun should help develop in individuals
and in the community:
Confidence in themselves;
The sense of being able to do things;
The skills required to complete projects.
It is a matter, for example, of showing the community the
steps to follow in formalizing an agreement, not to take the
steps for it. You need to bring to light past and present
successes to encourage people to continue on. In other
words, you need to try to emphasize at all times the
community’s own capacity for transformation. In this way,
a request for help can be converted into an opportunity for
empowerment. Starting with community dialogue, you can
promote a process of social change, in which the community
takes the reins and feels capable of finding solutions to its
problems—a guarantee of sustainability and of long term
actions. The use of the instrument, as described in the
following section of the manual, is embedded within this
context of social change and empowerment.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
PART II: THE INSTRUMENT Participatory Video Discussion Meetings
Once we have a clear view of the potential existing in the
community and the value of the “raw material,” it is
necessary to find the right instrument and methodological
process for working with community groups, based on the
ultimate goal of the project, which is to promote healthy
motherhood through:
The next step is to analyze the potential of video as a
generator of ideas and discussion, of reflection and
internalization of health issues. Of equal importance, the
active participation of the community analyzing its problems
and empowering itself to identify solutions and mobilizing
collectively leads to the objective of making room for
dialogue, collaboration and collective action at the
community level. Thus, this manual proposes “participatory
video discussion meetings” as an instrument and process for
reaching the above mentioned goal. Further on, it explains
in detail the objectives of participatory research, the
characteristics of the instrument of the participatory video
discussion meeting, the methodology and process for using
it, the facilitating role to be fulfilled by the team, the active
participation of the community in the “discussion meetings,”
and the logistical work that will ensure that the “discussion
meetings” flow with confidence, and the analytical capacity
and desire for action on the part of the community to arrive
at a commitment to saving lives.
1. The objectives of participatory research
The central theme of participatory research is to investigate
in partnership with the community the causes of maternal
and neonatal deaths, as well as the availability of health
services to assist in the presence of a case of obstetric
emergency. Our objectives are:
Enhancing and strengthening community participation
in the different components, caring for maternal and
neonatal health, and continual improvement of life
saving services.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
To get the community’s point of view on health services,
specifically as they relate to maternal and neonatal
health.2
To facilitate the active participation of the community in
analyzing its own reaction to an obstetric emergency,
observing the decisions and actions taken.
To support the community in its process of buying into a
program aimed at developing Community Emergency
Plans3 to save the lives of mothers and children.
In general terms then, the instrument and process of
“participatory video discussion meetings” serve to bring us
closer to the community, to “tie knots” with it, and learn
together:
What the community thinks and feels about health
services and the causes of maternal and neonatal deaths.
The real and potential barriers to and facilitators of use of
services.
2 To address other subjects using the same method, it would be necessary to
adapt both the content of the videos and the discussion guide. 3 The development of Community Emergency Plans implies, among other
things, the creation or consolidation of community networks for treating emergency cases.
The beliefs, attitudes and practices that influence
decisions on health in the community.
The aspirations of the community concerning: (a)
organizing to handle emergency cases; and (b) the
treatment and care provided in health care facilities.
The resources existing in the community that offer, or
could offer organizational opportunities for the
formulation of Community Emergency Plans.
2. The instrument: participatory video discussion meetings and how to use them
As mentioned earlier, the instrument developed to move
forward the process of participatory research has been called
“participatory video discussion meetings.” One of its key
approaches is the use of pictures to record testimonials and
life stories related to a particular health topic. When these
life stories are presented, especially when they are
developed and produced in partnership with the community,
the participants in the meetings or “discussion groups”
identify with the characters and situations portrayed and
relate it to what they experience in their own community. A
very fruitful discussion follows, in which the participants are
encouraged to tell their own stories, offer different and/or
complementary points of view, think about what they have
seen and heard and, in many cases, negotiate proposals for
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
taking action. Hence the use of what we call “participatory
video discussion meetings” with the communities, as
opposed to the use of techniques for collecting data on the
community. In effect, it is an instrument of mutual learning
more than a technique, a tool for encouraging and
maintaining social change in the community.
Since the organization of the “discussion meetings” takes
place in the community, an implementation and discussion
guide is available to help us move through the process of
“participatory video discussion meetings.” The “discussion
meeting” is organized around the following seven key steps:
1. Creating a good relationship
2. Presenting the project and introducting the facilitating
team and the participants
3. Creating a friendly atmosphere: ice breaking exercise
4. Presentation of short life stories: videos 1 and 2
5. Prioritization of the attributes of quality from the
community’s perspective
6. Community mapping
7. Wrapping up the discussion and continuing collective
action
Step #1. Creating a good relationship
This is the first contact of the facilitating team with the
participants in the handling of the working sessions and
the “participatory video discussion meetings.” The
facilitating team4, although not in its own community,
plays the role of host and, and such, is in a position to
welcome the participants from the moment they arrive at
the meeting place. To successfully play the role of host,
the facilitating team should:
Get set up ahead of time in the room where the
discussion meeting will take place, so that they can
greet the participants as they arrive.
Converse informally with the participants and give
them a respectful and friendly welcome.
Invite them to give their information (socio-
demographic) to the person responsible for
collecting it, who can explain to them that this
information is only being asked to get an idea of
their ages, the number of children they have, and if
they are already using health services.
The team should take advantage of the refreshment break
to continue developing a good relationship with the
community. At this time, whether it is in the middle or at
the end of the discussion meeting, the facilitating team
serves the refreshments and interacts with the
participants. Just as if they were entertaining a friend at
home, they wait on the participants as graciously as
possible, making sure that no one wants for anything and
conversing with them.
4The composition of this team will be explained in the next section.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
One barrier to interaction between the facilitating team and
the participants might be the fact that they do not all speak
the same language. In this case, the members of the
facilitating team who speak the participants’ language will
act as a bridge between them and the rest of the team. It is
also important to remember that, more than verbal
communication, the non verbal communication, the attitude,
the care that is taken to ensure that no one lacks anything are
signs that the participants notice, and that contribute to
creating a good relationship with them.
Step #2. Introducing the facilitating team and the participants, and presenting the project
The presentation of the project, the facilitating team and the
assembled participants is essential. How this presentation is
done will motivate “spectators” to become “real
participants” and to feel free to express their points of view.
During the presentation of the project and of the facilitating
team, the facilitator should:
Explain the objectives of the discussion meeting and
thank the participants for coming: Mention that the
subject of particular interest is the health of mothers
and newborns. The participants may be used to
participating in skills building sessions or in
discussion groups in which an outside team comes in
to impart or obtain information from the community.
During the presentation of the project, the facilitator
can clarify that this is not a skills building session and
that what the group of facilitators wants is to learn
with the community and gain a better understanding of
its points of view concerning health. Nor is the team
going to gather information and leave. What it wants
is to see how it can support the community. In this
regard it is also important not to create false
expectations in the community: the facilitator should
clarify, if necessary, the type of support that the team
can provide and the parameters within which they
have to operate. For example, it must be made clear
that the team does not have any funding to offer the
community. The one thing it can do is support them
with ideas on how to organize to save the lives of
people who may be confronted with an emergency
from one moment to the next in the community.
Explain to the participants the confidential nature
and anonymity of its interventions: It is very
important to assure the participants that no one will
be quoted by first and last name, and that the
opinions shared during the discussions will not be
repeated or used without their consent.
Explain the need to record the meeting in order to
have a “souvenir” of the discussion: The
facilitating team should see to it that each
discussion meeting is recorded. Each tape is
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
transcribed to facilitate the analysis of the
information gathered later on. The participants
might ask why they are being taped, and feel
intimidated by the tape recorder placed in the
middle of the room. It is recommended to ask the
participants’ permission to record the session,
assuring them once more of their anonymity and
confidentiality. In some circumstances, not asking
permission to record can create mistrust among the
participants. In such cases, it is best to limit
yourself to explaining as clearly as possible the
need for a document that will help to remember
what was discussed: it is also a way to respect
what the people have said, since we cannot trust
our memory alone. If, in addition to the audio
recording, the meeting is being videotaped, you
can offer to let the participants see the tape
afterwards. People generally like to see their
picture on the screen, and it is a way to share with
them what we share during the discussion
meetings.
Explain the process that will be followed during
the discussion meeting: The facilitator explains to
the participants that they are going to watch
together a couple of short films prepared for the
meeting and that they will converse informally
about what each one thinks. He also explains to
them that afterwards they will also make a couple
of presentations as a group.5
Asks them to interrupt him at any time if there is
anything that is not clear: What we want is for
everyone to participate, and for that, we need to
understand each other well. He can use the
opportunity to ask the participants if they have any
questions or if they would like some clarification
before going on.
Introduces the other members of the team and asks
the participants to join in the introductions: The
facilitator can introduce the members of the team
or, better still, the other members of the team can
stand in front of the participants and introduce
themselves briefly. Each one can give his name
and mention what his role will be during the
meeting. If they are health workers (HW), they
should not mention their responsibilities in that
area, since that could, on the one hand, intimidate
the participants, and on the other, create an
atmosphere more like that of a skills building
session than of an informal exchange. In the same
way, those present at the meeting should also
5 Note that we are using the words “short film or video” instead of “video clip,”
and “presentation” instead of “dramatization.” It is necessary to simplify the language and avoid new or complicated words with which the participants might not be familiar.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
introduce themselves, adding a few words if they
so choose. The facilitating team can also
participate in the ice breaking exercise, as one
more member of the group, to encourage trust and
enable people to communicate with one another as
equals.
Explain that they are going to begin with a little
exercise to get to know each other better: At which
point the ice breaking exercise takes place.
Step #3. Creating a friendly atmosphere: Ice breaking exercise
There are various techniques for leading a group with the
main objective of creating a friendly and participatory
atmosphere. An ice breaking technique is one that helps the
participants and the facilitating team get to know each other
and thus begins to create a friendly and relaxed atmosphere
for conversation. Taking into account the characteristics of
the participants and the context, a technique6 should be
chosen for the discussion meetings that:
Is active;
6 A useful reference for selecting a participatory and ice breaking technique is
the book edited by the Alforja Center for Studies and Publications entitled, “Participatory Techniques for Popular Education” (Volumes I and II, San José, Costa Rica: Alforja Center for Studies and Publications, 1988).
Helps the participants relax;
Involves the participation of the participants; and
Includes humor.
Step #4. Presenting stories from life: Videos 1 and 2
The videos show the participants short stories from life,
“slices of real life” that reflect what is happening in the
community. We will describe later the objectives and
content of the videos and the discussion guide used to
stimulate dialogue and discussion for the purpose of learning
and investigating together with the community how it acts
when faced with an emergency case involving a pregnant
woman and what the community thinks of the quality of
services offered in the health facilities for cases of
obstetrical emergency.
Video #1: Story of a mother in crisis set in the community
Objectives:
Explore what the community usually does when an
emergency arises during or immediately after delivery.
Find out what the customs and traditions are regarding
the care of the mother and the newborn.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Investigate what might prevent a woman from being
taken to the appropriate health center.
Investigate what might facilitate the transportation of the
woman to the appropriate health center.
Synopsis of the Story:
A woman lies ill at home. The person who is with her
explains to another the woman’s symptoms, but neither
of them knows that these are danger signs. The midwife
arrives and says that in this case she can no longer do
anything for the patient. At the same time, a health
professional (or provider) arrives and insists that the
woman be taken to the nearest health center. The
husband is not there, and the mother-in-law does not
want the woman to be taken to the health center. A
heated argument ensues among those who are around the
woman about what should be done. You see the woman
becoming weaker the whole time, beginning to faint.
The film cuts off here.
Screening of Video 1:
The facilitator explains to the participants that he is going to
show them a film,7 after which they will discuss what they
have seen. While the video is playing, the facilitating team
7 The words “film” or “video” are used instead of “video clip,” which is a term
the participants are probably not familiar with.
checks to see if the participants are following it attentively.
In remote rural areas, it may be that the people are not used
to watching television, and at first may not pay enough
attention to the content, but rather focus on the form. It is
recommended to show the video a second time to make sure
that all have seen and understood it from beginning to end.
You should also ask the participants if they want to see the
film from beginning to end.
Dialogue and Discussion8:
After watching the video, proceed to group work using the
following discussion guide:
1. What do you remember of what you have just seen?
Have you experienced anything like this? Have you
heard of a case like this in your community?
2. What happens in the film? What is wrong with the
woman who feels ill? Who is arguing? Why are they
arguing?
3. In cases like this, what do the people in the community
do? What is done with the woman?
4. (If necessary, pick up the thread of the story to help the
participants remember). In your opinion, what would
happen next? When and how does the family realize that
the woman’s condition is serious? Who decides what to
8 The discussion guide for the dialogue and discussion following the video
screening can be found in Appendix #1.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
do? What do they do? (accept that she is going to die,
call in a traditional healer, take her to a health center:
church based, institutional, women’s practice)? What
happens to the sick woman at the end (dies, survives)?
5. What problems will they have to face in trying to save
this lady’s life? What do they need to resolve these
problems? Who helps them? Who does not help them
(at various levels: family, community, networks outside
the community)? How hard is it to resolve these
problems?
6. If you were in this situation, what would you do?
7. What happens when a woman dies in the community?
Who are the children left with? Who takes care of them?
What happens to the husband?
Video #2: Story of a pregnant woman who goes to a health center in an emergency
Objectives:
To explore what the community likes and does not like
about its health services and how it would like the health
services to be (quality attributes).
To explore what the barriers are to using the health
services.
To explore what might facilitate greater use of health
services.
Content:
They arrive at the Health Service and a service provider
receives them saying why did they wait so long. He is rude
to the family and to the midwife. The medical health care
provider on duty arrives (a young man). He does not speak
the language, and willingly explains what is wrong with the
patient. The interpreter has difficulty translating because the
doctor has used technical terms that do not exist in the local
language. The doctor starts gathering the instruments
needed for the intervention, and everyone around begins to
mobilize—and the film cuts off.
Screening of Video 2:
The facilitator explains to the participants that they are going
to see part of another film and discuss it afterwards.
Dialogue and Discussion9
1. What did you see in the film? What is happening?
2. Has anything like this happened to you or to someone
you know? What happened?
3. What is it that most draws your attention in this second
film? What else do you see? Is it like this in the health
services that you know?
9 The discussion guide for the dialogue and discussion following the
screening of Video 2 can be found in Appendix #1.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
4. (If necessary, pick up the thread of the story to help the
participants remember). Do you remember that we
showed you only one part of the film? What do you
think happened at the beginning (in the part of the film
that we did not show: when the family arrives at the
health center)?
(If the subject was not addressed in the previous
section) What did the family do to get to the health
center?
How was the family received at the health center?
How do you think that the health workers treated the
family, the lady, the midwife? Did they let them ask
questions? How did they answer?
What did the health workers say to the midwife?
5. And in the film clip that we saw, how do you think the
lady and her family feel in the place where she is being
treated? How does the place where the lady is being
treated seem to them? How do they see this place? What
is present and what is lacking in the health center? What
do they like and what don’t they like?
6. If it were you in this situation, what would you do?
7. At the end of the film (which we haven’t seen either
because we cut it off before it got there) what do you
think happens to the lady (does the lady live or die)?
8. What would be a happy ending to this second film?
What would be needed to get to this happy ending?
9. How would you like to be treated in the health centers?
Step #5. Prioritizing the attributes of quality that a health center should have from the community’s perspective
During the dialogue and discussion generated by Video 2,
explore the attributes of quality and satisfaction regarding
the health center from the perspective of the participants.
The objective of this exercise is precisely to prioritize in
order of importance the attributes or characteristics that a
good health center should practice and/or demonstrate. For
example, the participants might have mentioned in the
discussion of the video that they do not like being treated
badly or being yelled at when they bring a pregnant woman
with complications to the hospital, but that they appreciate
the fact that the doctor who treats the woman cures her: what
is most important to the participants, the treatment given to
the people accompanying the woman to the hospital, or the
technical competence of the attending physician?
Procedure:
1. Ask participants to divide into two or three groups
(depending on the number of people). Each group is
going to act out how it would like the story they just saw
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
to end (video 2) from the moment the lady arrives at the
health center until they save her life.10
2. Each group presents its dramatization. The facilitator
asks the participants to comment on the dramatizations of
the other group and of their own group, using questions
such as:
How did you feel in the health center?
What did you find in the health center that you liked?
How did they treat you there?
How was the sick woman’s life saved?
3. The facilitator or observer draws pictures on a flip chart
of what the people are saying. This can be done by a
member of the facilitating team who has a talent for
drawing.11
10
It is appropriate to mention here that in the first version of the instrument,
the participants were asked to act out the “happy ending” of the story they had just seen. We realized that those words had no meaning to the people in some communities, so we decided to ask them to act out how they would like the story to end.
11 Another possibility is to use
a flannel board with figures prepared ahead of
time. If you decide to make one, you can pull out from the first meetings the elements of the discussion with the participants that come up the most often. On that basis, a flannel board could be made which would serve as a tool for discussion in this and other phases of the project with the communities. You can also choose to conduct this exercise with figures, chosen in advance, that can be attached to a flipchart during the discussion.
4. Once all the comments have been made and all the
images have been placed on the flipchart, the facilitator
poses questions that will help them arrange the elements
mentioned in order of priority:
If you had to arrange everything you mentioned in
order of importance, what would come first? What
next?
The facilitator explores where the points of view
diverge and converge and the reason for the order of
priority selected by the participants.
He reorders, simultaneously, the elements following
the order of priority indicated by the participants
(numbering the elements in a list on the flip chart).
5. He checks the final list of priorities to make sure the
order reflects what the group thinks.
Step #6. Community mapping
The objective of the community mapping exercise is locate
the key people and resources that can help families in
emergency cases, including representatives of: the local
institutional authority, the local traditional authority, the
traditional health care system, the social network (for
example, neighbors and relatives). One of the
characteristics of community mapping is that the map is
drawn with the active participation of community members
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
to identify existing resources and networks that can be
mobilized in the case of maternal and neonatal emergency.
Procedure:
1. Ask participants to divide up into two or three groups
(depending on the number of people). Each group is
going to act out how they would like the first story to end
(Video 1) from the moment the lady’s condition becomes
critical until a decision is made about what to do.
Explain to the participants that this dramatization or
representation needs to show how the community can
organize itself to bring a successful outcome to a critical
case (emergency). What do they decide to do? When do
they make the decision? How do they manage to get the
woman out of her house to save her life? What helps
them? Who helps them?
2. Each group presents its dramatization. The facilitator
asks the participants to comment on the dramatizations of
the other group and of their own group. The facilitator
then explores:
Who can help ensure that the mother or the child are
saved?
For example, to take the woman to a health center
where they can save her life
Who can help make the decision in time?
Who can help with transportation?
Who can inform other members of the community and
the health service of the emergency?
The facilitator draws figures on the flipchart representing
these players.12
Where are these people in the community? Near the
home? Far from the home? What can be done to
locate them? Is it possible to speak with them?
The facilitator, using the opinions of the participants,
draws a map of community resources on which can be
placed the key people who can help families in case of
emergency. If possible, he may ask one of the
participants to come up front to help him make this little
map. Showing the map to the participants, the facilitator
checks that his representation corresponds to what they
are saying, and poses the following final questions to the
group:
What can the community do to help in cases of
emergency?
Is it possible for all of us to mobilize to lives?
Who are the key people in the community for
emergency cases?
What resources exist in the community? 12
You might also consider making a flannel board as in the previous case.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
The facilitator draws figures on a flipchart that represent
these persons or identified players, as well as resources
available in emergency cases within the geographic space
of the community.13
Once the map has been completed, the discussion leader
poses the following question to the group, with which the
dialogue on the central theme concludes:
What can the community do to help in emergency
cases?
Can we all work together to save lives?
Step #7. Wrapping up the meeting and continuing the collective action Following the last question posed to the participants, the
facilitator explains that the objective is really to work with
the community to improve health services, to help them
prevent health problems, and support them in dealing with
emergencies in order to save lives. At the same time, he
emphasizes that we are engaged in a long term process, and
this is only the beginning. He thanks them for their
participation and invites them to make their final comments,
if they have anything to add.
13
As in the previous exercise of prioritization, you might also consider
making a flannel board or using figures chosen ahead of time.
He then explains what the follow-up will be, that is, an effort
to “devolve” the joint discussion for participatory research
into the community. He outlines how, with all the findings
coming out of this process, it will be possible to follow
through by taking collective action with some initiatives that
have already been developed in many other communities
through their local authorities and their community
assembly, such as the development of a Community
Emergency Plan14
and the Family Emergency Plan15
to
protect the lives of mothers and children.
3. The facilitating team for participatory video discussion meetings
In this section, we specify the composition of the team
responsible for moving forward the process of “participatory
video discussion meetings,” and the functions of each of its
members. Here we will explain in detail some of the
characteristics and qualities that the facilitating team should
14
This is the expression of an organized community working together to
solve a health problem: an emergency that places at risk the life of a mother or a child. The Community Emergency Plan is the instrument that gives concrete expression to the community’s empowerment to save lives.
15 The Family Emergency Plan is worked out by the pregnant woman with
her husband, within the family, making in advance decisions such as the following on what to do if confronted with an obstetric emergency, then going to the community health committee for help: Where to go? How to go? Who will go with me? Who will look after my house and my other children? How much money do I have saved up?
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
display, and finally, we will address the subject of
moderating group discussions, giving helpful tips for
conducting participatory video discussion meetings. We
invite you to review Appendix #2, which further develops
the practical tips for conducting participatory video
discussion meetings presented in this section.
3.1 The facilitating team
The facilitating team for the participatory video discussion
meetings is composed of:
(a) A facilitator (or moderator), the person who leads the
group discussion
(b) A participating observer who takes notes during the
meeting and supports the moderator (or facilitator),
indicating, for example:
That there is someone in the meeting who has
something to say;
That it is necessary to bring into the discussion a
participant who is sleeping or not participating;
That it would be good to return to a theme that one
of the participants mentioned, to complete it, etc.
The participating observer also looks after the tape
recorder to make sure the meeting is being properly
recorded, and changing the cassettes in time.
(c) A camera operator (if necessary). In some cases, a
person is needed to video tape the discussion meeting.
Sharing the video taped images with the participants
can be part of their process of learning and mobilizing
to develop emergency plans.
In this first phase, it may be appropriate for the team that
is facilitating the discussion meetings to not be the same
as the institutional health care providers working in the
same locality or community. This has a dual purpose: (i)
to avoid the label of “capacity builders” that the health
workers already have because of the work they do, and
that would lead the participants to confuse the discussion
meeting with a capacity building session; (ii) to ensure
that the people feel completely free to express their
opinions. One possibility is that the health care workers
in one locality could meet with communities in a region
other than their own. The other possibility is that the
facilitating team could be made up of people from the
outside, not necessarily health care providers, who are
skilled as moderators and co-moderators. In cases in
which the health professional or health care provider acts
as moderator or participating observer in the community
where he works, it is important to make sure that his
presence does not affect the results of the process.
3.2 The qualities and skills of the facilitating team
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
The facilitating team will need to do detailed work that is
rigorous and requires organizational ability, but that is also
fun. To do this successfully, it is important to practice
certain qualities, such as:
Knowing how to listen
Acting with modesty
Keeping open
Having a sense of humor
The basic, guiding principles of this activity are:
Respect (including respect for differences)
Equity
Veracity
The golden rules to follow are:
Punctuality
Fulfillment (of promises, offers, etc.)
Always keep in mind that it takes years to cultivate bonds of
trust with the community, but only seconds to destroy them.
The community can tell whether the relationship that the
team is establishing with it is authentic or not, and confirms
it, for example, when it sees that the team:
Is not creating false expectations in the community
Respects the confidentiality of the participants
The facilitating team must be:
Participatory and structured at the same time.
What does that mean? It means that participation
does not happen spontaneously, but is the result of
a conscious and deliberate effort to create the
necessary conditions for people to participate.
To be successful, participation must:
Be structured and organized
Respect the time available for the discussion
meetings
Be flexible enough to adapt to circumstances
and to the environment
Be creative in finding the best way to adapt
to the environment without losing sight of
the objectives that have been set
Be disciplined in documenting
systematically the results of the discussion
meetings, so as to be able to give them back
to the community and transmit them to
decision makers in a reliable manner.
Finally, it is important that the facilitating team:
Know how to develop empathy with the
community, while at the same time maintaining
an objective distance that will enable it to
document things the way they are.
To the extent that the team is aware of its own subjectivity,
of its values and beliefs, it will be able to attain the
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
objectivity needed to complete the work proposed in this
manual.
3.3 Practical tips for leading group discussions During the discussion meetings, the facilitator plays many
roles, acting at times as a “journalist” who:
is “at the center of the action”;
is seeking the opinion of the “experts” who are
the members of the community;
wants to know the truth;
at times as an “anthropologist”:
who is learning with the community
is always ready to discover new things;
and is, at the same time, a “craftsman”:
who works with great detail and
who is patient and persevering.
4. The participants from the community invited to the participatory video discussion meetings
The participants in the participatory video discussion
meetings are chosen using specific criteria within a process
of selection that includes all the community.
4.1 The process of inviting the participants
The external agents, in this case the facilitating team, often
go through the formal local authorities to conduct meetings
in the communities. It is important that these key people,
who are going to convene the meetings, have a copy of the
list of criteria for selecting the participants in each meeting.
But beyond these criteria, it is essential to make clear that
we want to invite to the discussion meetings members of the
most vulnerable groups within the community.
Every community and society is a complex universe, in
which can be found distinct social strata. Taking into
account the limitations that the environment may impose, it
is important to try to promote the participation of those who
may have been marginalized because:
It is believed that they are not able to or interested
in participating,
They belong to marginalized groups (for example,
the poorest) within the community,
They do not belong to the group of voters who
elected the reigning authorities.
Experience has taught us that a restricted and biased
invitation can cause resentment and mistrust in the
community. At the same time, the presence of external
agents, who come with a point of view that is foreign to the
community, can sometimes contribute to the inclusion of
groups that have traditionally been left behind, and open
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
areas of dialogue in which those particularly vulnerable
groups may participate.
4.2 Criteria for selecting participants
In the case in question, we have identified at least four
groups of people that we are interested in meeting with in
separate groups, since each of them brings a different
perspective to maternal and neonatal health and dealing with
emergency cases in the community. These are: women,
midwives, leaders, and men. It is important that each group
be homogeneous to facilitate a free exchange among the
participants. For example, if we invite a midwife who is a
traditional leader in her community to participate in a
discussion meeting with mothers of families, we will find
that her discourse is different from theirs; she will probably
talk more than the other women, and may influence their
opinions. Hence the importance of meeting with these
groups separately.
The criteria for selecting the participants are, in each case:
GROUP OF WOMEN
Should be pregnant or have been pregnant (may
have lost children). You might want to also
include women in union of reproductive age who
have not yet become pregnant.
It is important to include young future mothers and
women who have borne many children.
Users and non users of health services.
Should speak the local language.
GROUP OF MIDWIVES
Should represent different levels of experience as
midwives.
With and without formal training (in traditional health
services).
Should speak the local language.
GROUP OF LEADERS
Institutional leaders (deputy mayor, president of the
church committee, evangelical pastor, school
committee, etc.) and traditional leaders (midwife,
Mayan priest, traditional healer).
Men and women (gender balance), but taking into
account the actual make-up of the community.
Diversity in type of leadership (religious, political,
etc.).
Should speak the local language.
Invite influential midwifes to participate in the
leaders’ discussions (or they could lead the discussion
in the groups of less influential midwives).
GROUP OF MEN
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Husbands or partners. They may or may not be the
partners of the participants in the women’s group.
Users or non users of health services.
Should speak the local language.
Concerning the selection criteria: In no case is age
considered a criterion of selection. Especially in the
women’s group, the highest rate of mortality occurs at the
beginning of reproductive life; and therefore it is important
to also include young future mothers. On the other hand, it
is also important to invite the participation of women who
have borne many children, who are also a group at risk.
5. Planning ahead and logistics
Conducting meetings in the country’s remote
communities requires a considerable amount of
organization and coordination. The port of entry into the
community, as we have just mentioned, is formal local
authorities. A visit to the selected community ahead of
time will allow the members of the facilitating team
tomake an initial contact with the community and
confirm its interest and the feasibility of conducting
meetings in the area. Once the possibility of conducting
them in the given community is confirmed, you should
proceed to carefully plan the visit and make
arrangements for the human and material resources
needed for the meetings.
5.1 Resource management
It is recommended to use checklists for the purpose of
providing for the human and material resources needed for
each discussion meeting. The preparation ahead of time of
other documents, such as the socio-demographic information
sheet for each discussion meeting, or the guides for dialogue
and debate translated into the local language, will also
contribute to the successful realization of the activities.
Table of human resources
Prepare a table on which you can write the names of the
members of the facilitating team for each locality. This
table will serve to check whether enough team members
are available on the dates scheduled, and for each
discussion meeting. An example of the Table of Human
Resources can be found in Appendix 3.
Table of material resources
Set up a table of the material resources with the list of
supplies that will be needed for the meeting, and use it as
a checklist before going out to the field. An example of a
Table of Material Resources can be found in Appendix 4.
The socio-demographic information sheet
Do not forget to prepare, for each meeting, a sheet on
which you can record the data (most important)
concerning the participants. Examples of socio-
demographic information sheets can be found in
Appendices 5A and 5B.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Translation of the instrument
The instrument should be translated, preferably ahead of
time, for use in meetings conducted in languages other
than Spanish. This translation should respect the
formulation and the order of the questions in the original
instrument.
It is important not to rely on the facilitator’s memory for
the translation, nor on his ability to make simultaneous
translations. It should not be forgotten that the work of
simultaneous translation and interpretation requires
specific training and experience that the majority of
moderators do not have.
Transcribing the discussion meetings
The team should make preparations for the work of
transcription before going into the field. The team
should locate and contact with sufficient lead time the
people who will be doing the transcriptions, to ensure
that they will be completed as soon as possible. These
people should speak the language of the place where the
meeting will take place, be fast typists, and, if possible,
be experienced in this type of work.
They should be given a written sheet of precise
instructions on how to do the transcriptions. (This can be
found in Appendix 7).
Some instructions for transcribing:
Indicate who is speaking in each case.
Translate what the person says as he says it.
Do not summarize or synthesize what the person is
saying.
When it is difficult or impossible to translate words into
Spanish (because they do not exist in our vocabulary),
write them in the local language and explain in
parentheses what they mean.
When the literal translation of the word illustrates ways
of thinking or looking at the world, stick to the “literal”
translation and explain in parentheses what the word
means in context (for example, if the person uses the
term “filthiness” to refer to menstruation, write
“filthiness” and explain in parentheses what it means).
The format that the person uses to transcribe the information
will depend on how the transcript will be used. Thus, if the
meeting has been video taped and the intention is to edit the
tape, a format will be used that will allow the images to be
matched with the text. If the intention is to use the transcript
for an analysis of the discourse (verbal) of the participants, it
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
will suffice to transcribe the verbal statements of the
participants.16
5.2 Time management
Managing time is important at specific moments: before,
during, and after the meetings.
Before the meetings:
Plan the meetings in advance and, as much as
possible, send a reminder one or two days before the
date of the meeting, in conjunction with health
personnel and/or local authorities.
In consultation with key people who know the
community well, including the health care providers
who work in the area, select the appropriate
organizational model for each case. Table 1
summarizes three formats for organizing the
discussion meetings from which the facilitating team
may choose. It is important that once the most
appropriate format has been chosen, you plan for the
specific resources and time required for each one.
16
In some cases, in which the researchers have opted to analyze the
information with the help of computer programs, precise instructions must be given so that the format of the transcriptions is compatible with the program.
Arrive at the location sufficiently ahead of time so
that the team can meet and iron out the final details
for each discussion meeting.
Plan the transcription of the sessions in advance,
taking into account the fact that it takes at least 8
hours to transcribe one hour of audio tape.
Anticipate follow-up activities and the outputs to be
presented as a result of the process and prepare a
detailed workplan, taking into account the points
mentioned above.
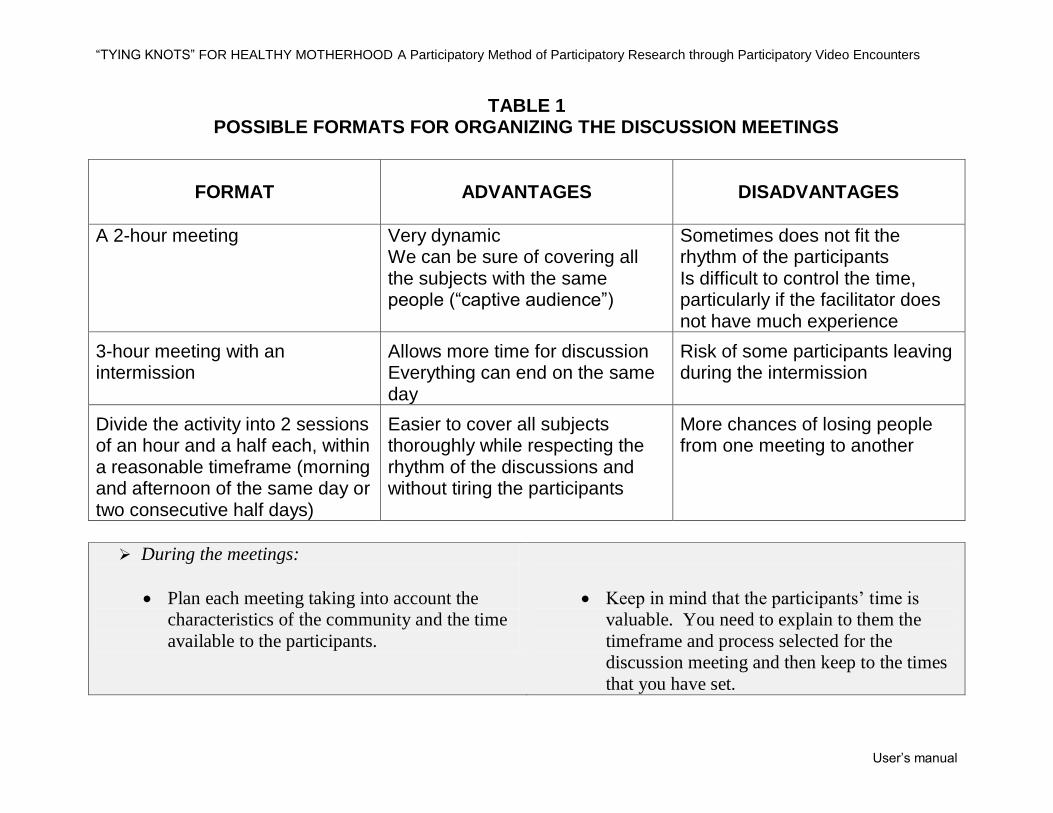
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
TABLE 1 POSSIBLE FORMATS FOR ORGANIZING THE DISCUSSION MEETINGS
FORMAT
ADVANTAGES
DISADVANTAGES
A 2-hour meeting Very dynamic We can be sure of covering all the subjects with the same people (“captive audience”)
Sometimes does not fit the rhythm of the participants Is difficult to control the time, particularly if the facilitator does not have much experience
3-hour meeting with an intermission
Allows more time for discussion Everything can end on the same day
Risk of some participants leaving during the intermission
Divide the activity into 2 sessions of an hour and a half each, within a reasonable timeframe (morning and afternoon of the same day or two consecutive half days)
Easier to cover all subjects thoroughly while respecting the rhythm of the discussions and without tiring the participants
More chances of losing people from one meeting to another
During the meetings:
Plan each meeting taking into account the
characteristics of the community and the time
available to the participants.
Keep in mind that the participants’ time is
valuable. You need to explain to them the
timeframe and process selected for the
discussion meeting and then keep to the times
that you have set.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
After the meetings:
Plan ahead of time the tasks of
consolidation and analysis of the
information so that you can, in a reasonable
amount of time, transfer the information to
the stakeholders: the community itself and
the decision makers.
Refer to the workplan and respect the
deadlines that have been set. If this is not
possible, communicate the changes to the
individuals involved (that is, those who are
waiting for the results from the team).
5.3 Space management
You will also need to take into account during the
organization of the discussion meetings the physical
conditions in which you will be working, for example:
Electricity. Find out if there is electricity in
the community. If there is no electricity,
find an electric generator in the community
that you can borrow. If this is not possible,
contact a group of volunteers who will be
willing to do a dramatization or social drama
at each of the discussion meetings.
Location of the meeting. The location where
the discussion meetings will be carried out is
critical to ensure availability. The
characteristics of the site to be considered
include:
That it be sufficiently spacious to hold
the group and, if possible, not so large
that it echoes or the participants scatter.
That it not be so close to a point of sale
or a noisy environment. This can be
distracting during the discussions and
make recording difficult.
The physical arrangement of the chairs or
benches for the participants is also
important: Form a semi-circle or circle
that includes the facilitating team.
Having the participants close to each
other will create a more intimate
atmosphere that will promote
conversation and at the same time
facilitate recording.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Position of the facilitating team in relation
to the participants. Make sure that the
facilitator and his team are not positioned in
front of the audience as if in a lecture hall.
This arrangement gives the impression that
those on one side (those who are in front)
“know” (are coming to teach) and the others
(those who are listening) “don’t know” (and
are coming to learn). On the contrary, what
we want to promote in this case is an equal
exchange between the facilitating team and
the participants.
Arrange lodging for the facilitating team. If
the facilitating team needs to spend a few
days in the community, you will need to find
a place where they can sleep. As we will
see later, the visit or stay in the community
is in itself an opportunity to forge bonds
with the community and meet informally
with people who are not participating in the
discussion meetings.
6. Processing the Information
It is not enough to gather information and interact
with the community. If you want to use the
information to support a process of change in the
community, it is necessary to process it and analyze it
to pass it on to the community, so that the latter can
share it with decision makers. This is necessary so
that, on the one hand, you can process the experience,
and on the other, you can complete an analysis of the
discussion to find useful proposals that come from the
participants themselves, and in which they can see
themselves reflected.
6.1 Processing the experience
Processing is a separate methodological subject in
itself, which we will not attempt to cover in this
manual. Here we are only suggesting a couple of
basic tools that can be used to process the experience
for the facilitating team and the community. We are
talking here about developing tools for recording the
most outstanding moments, events and actions and, in
this way, building a vivid record of the process with
the community.
The document of reflection and self-
examination should be filled out at each
meeting, and should mention the outstanding
points (barriers, facilitators, findings,
surprises) regarding:
Preparation
Invitations
Organization/logistics
Facilitation and instrument
Content of the discussions
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
The process with the community
A travelogue can document the formal and
informal interviews and observations of the
facilitating team during their time of
residence in or visits to the community:
Date
Description
Outstanding elements
Follow-up planned
Glossary of terminology used in the
community
Tables for compiling and organizing data
concerning:
the resources identified in the
communities, such as the commonly used
traditional and technical communication
media, principal communication
channels and sources of information and
formal and informal communication, key
people and groups, existing networks,
etc. This data serves to develop
strategies for social participation and IEC
(information, education and
communication), as well as the creation
or consolidation of life support systems.
Periodic processing meetings planned
ahead of time for:
The interaction and socialization with
the community and with the health
care providers working at various
levels.
These meeting are neither
spontaneous nor casual. They should
be organized ahead of time following
a precise agenda and a participatory
methodological framework that is
coherent with the process of
participatory research.
6.2 Analyzing the discussion meetings
Data analysis is a complex subject that goes beyond
the limits of this manual. Suffice it to say that a
detailed analysis of the discussion meetings will make
it possible to better understand the psycho-social and
socio-cultural dynamics that influence the ways of
doing and being in a community. This understanding
will, at the same time, allow the development of
strategies appropriate to the context and the
identification and planning for potential problems that
might be encountered in the communities having to do
with the health of mothers and newborns. In addition
to its usefulness from the point of view of external
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
agents who want to improve the way they work with
the community, data analysis in this context starts
from the community’s point of view, and seeks to
give back the results so as to reinforce the process of
community empowerment.
To complete this type of analysis, you should take
into account certain steps that require planning and
organization, such as:
Preparing the transcripts;
Arranging data in matrices;
Analyzing the information;
Disseminating the results.
It is recommended to rely on experts in qualitative
analysis to jointly carry out this task. The
contribution of those involved—both the facilitating
team and the participants from the community—is
essential during the analysis phase. The process of
giving back to the community often becomes an
opportunity to validate and refine the results of the
analysis.
7. Use of the Instrument within the Process
The participatory research instrument that we suggest
is a learning tool placed within a context that goes
beyond participatory video discussion meetings. It is
essential to not lose sight of the fact that, beyond the
“collection of information” there is the process that is
started with the community, whose success will
depend on completing the following steps in the
partnership. During the visits to the community, there
is a series of parallel tasks to be carried out, that
complement and reinforce each other:
Conducting participatory video dis-
cussion meetings with various groups
Creating and developing contacts with
grassroots organizations, committees,
non governmental organizations, etc. that
are active in the community.
Developing a strategy for how these
groups formed by the discussion
meetings and the people and key groups
contacted in the community can remain
involved throughout the life of the
project to carry on the work.
Continue with the “community mapping
outside the discussion meetings, going to
see what is there.
Taking the opportunity to converse with
the other members of the community as
well, and not only with those who
participated in the meetings.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
These conversations will revolve
initially around more general themes
that will give us an idea of the reality
and the trajectory of the community,
as for example: how the community
was formed, what life in the
community is like, if there are many
children, what the holidays are, how
they celebrate them, where the school
is, where the parish church is, who the
authorities are (traditional and
formal), where people gather, if
people in the surrounding areas know
each other well, what the main
problems in the community are, if
they help each other, etc.
Little by little, in a second phase, you
can address themes such as: What do
you do when someone is sick? How
far do you have to go to be treated, or
does someone come to your homes?
Do you know any woman who has
had problems with her pregnancy or
at childbirth? What do people do in
such cases: Where do they go?
Whom do they see? Do they go to a
health center? When do they go?
Where? How is it for you? What
type of care do you prefer? Do you
know of people or organizations
(formal or informal networks) that are
important in the community and that
we should be contacting? Etc.17
Strengthening the bonds with the
community based, for example, on
participation (by invitation) in community
meetings.
It is essential in this phase to establish and/or
consolidate the work with networks and develop
bonds of trust and collaboration with members of the
community. The success of the initiative can be
measured in terms of the continuity and strengthening
of these bonds over the long term.
17
All of this information should be documented using the tools
suggested above for processing the experience.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
PART III: THE “KNOTS”
It is not enough to have excellent raw material and an
appropriate instrument to “tie the knots.” You must
ensure the quality and continuity of the bonds being
forged with the community. To do this, the most
important thing is to promote dialogue and
participation. Dialogue and participation are, in
effect, the main ingredients in the process of creating
bonds within this participatory research. These
elements carry the work from beginning to end. In
this section, we will offer guidelines for two practical
issues regarding participation that may come up
during the work: the issue of incentives and giving
back the information collected from the community.
We will conclude with a reflection on dialogue and
participation as processes and as results to be
actualized in the community through the methodology
that we propose.
1. Recognition and Incentives
Often, the members of the community are interested
in participating. They are inclined not only to
participate in group discussions in which they can
express their opinions, but also to voluntarily carry
out a few specific tasks. For example, there are
members of the community who throw themselves
enthusiastically into doing dramatizations, which
allows us to replace the video images with “real life”
images when there is no electricity in the community.
Others act as interpreters when there are people from
outside who do not understand the local language in
which the meeting is being conducted.
The question of compensation for individuals who
collaborate and participate at various levels is a matter
of debate. There are those who think that it is
important for members of the community to get
involved voluntarily, without expecting immediate
material compensation in return. There are also those
who think that it is important to compensate people,
that it is a way to recognize their efforts and the time
they dedicate to an activity. Between those two
positions, which one is best for us to adopt? An
intermediate position would be one that:
Recognizes and provides incentives for
community participation and
Avoids, at the same time, giving the
impression that people are being “paid” to
participate.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
One way to do this is to find within the community a
“symbol” that at once:
Takes the form of an object that can be
distributed as an incentive during the
activities, and
Serves to reinforce the work in maternal and
neonatal health, without giving the
impression that it is a “remuneration” or
material compensation.
The “white ribbon” is an example of a “symbol” that
is also an object that can be distributed to the
participants. Ribbons are used all over the world to
symbolize various causes.18
The white ribbon
represents, among other things, the struggle against
violence towards women; the red represents support
for the cause of AIDS education, the yellow
represents support for the cause of defending human
rights. You might consider introducing into the
communities a ribbon or other object chosen with the
community as a sign of recognition and as a symbol
of the bonds of collaboration for improving maternal
and neo natal health. The ideal would be for this
18
The site www.sltrib.com gives information on ribbons of various
colors and the causes they represent at the world level or in various countries of the world.
symbolic object to be designed and fabricated with the
community, adapting it to the local culture. In this
case, the object would represent or would be a
“symbol” of the cause of maternal and neo natal
health. Based on this object a whole system of
incentives can be developed aimed at reinforcing the
participation of members of the community at
different levels.
2. Giving Back to the Community
Giving back the information gathered during the
participatory video discussion meetings is an essential
component of the participatory research process, since
through it the process of community dialogue is
strengthened and the community is encouraged to play
an ever more active role in seeking solutions to the
problems afflicting it. This giving back of
information should not take the form of a
“presentation of results” but rather as a basis of
interaction with the community.
At the same time that you are reporting back to the
community what its members think about the
handling of emergency cases or the use of services,
you are checking with them whether the information
seems correct and whether there are other opinions
that do not appear and which should be added. If you
have not yet begun to work with the community in
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
developing local life support plans, this meeting to
exchange opinions and information might be the right
time to begin this work. These plans will take on a
different name, according to what the community
decides.
Since the purpose is to create a space for sharing, this
meeting with the community should be organized in
such a way that it facilitates the presence of those who
participated in the discussion meetings, as well as
those who did not have the opportunity to participate
in them. This meeting will probably take the form of
a town meeting during which those attending will be
encouraged to actively participate. The health
workers that work closely with the community should
also be invited to the meeting and, if possible, co-
facilitate the meeting. There could then be one or two
facilitators during the meeting that would divide up
the work during the group discussion. The facilitator
or facilitators of the meeting should make use of
participatory techniques such as drawings, figures and
images to achieve a dynamic interchange with the
participants.
The themes of the meeting could be prioritized taking
into account the outstanding interests of the
community. To facilitate participation during the
meeting, the facilitators can follow the tips for leading
a group offered in Appendix #2 and be sure to check:
That what they are saying is clear and
comprehensible to the participants
What the participants think about what they
are saying:
If there is anything to add
If there is anything to correct
What the participants think of the proposals
made (for working together for example)
What suggestions the participants have.
It is important to plan this meeting carefully, both in
terms of content and in the provision of the human
and material resources to carry it out. To organize the
discussion on the Follow-up to the Meeting with the
Community it is recommended to use a table that the
facilitators can fill out with the help of the
participants. For this, you should plan on having
either a large chalk board or markers and flipchart
paper so that the facilitators can take notes on what is
discussed in the group. In this process of community
dialogue, the facilitators do not impose a program, but
rather negotiate the best way to include in the local
agenda the prevention of maternal and neonatal deaths
as one of the priorities in the community. This is an
opportunity to forge bonds between the community
and the health care staff, and to lay the foundation for
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
an endeavor that will require a long term commitment
from both parties.
3. “Tying the Knots”
As we indicated at the beginning of the manual, the
“knots” are not only an output but also a process. The
“knots,” or bonds of trust, are formed in dialogue with
members of the community, within a process of
participation that includes the most vulnerable groups.
Community participation should be sought at various
levels and at different times inside and outside the
meetings for discussion and interchange. But this
participation does not happen automatically.
Achieving it requires time, effort and perseverance.
On the one hand, many people have not yet had the
opportunity to participate, and it will take them time
to realize that they can do it and then learn how to do
it. On the other hand, to establish an open dialogue, it
is necessary to develop bonds of trust and maintain
them over time, something that is not accomplished
from one day to the next. At times, it is necessary to
begin developing bonds of trust in contexts in which,
for historical reasons, there is currently mistrust and
resistance to proposals the come from outside, or that
represent government interests.
Participation is:
A long and slow process
A goal to pursue, but also a series of problems
to solve
Participation:
Does not happen automatically
Requires “the work of ants” (one grain of sand
at a time)
Frequently, the need to respect the rhythm of this long
term process is confronted with the urgency of
delivering results within precise work plans. How,
then, to reconcile processes with outputs? We will
not presume to give an absolute answer to this
question within the limited space that remains within
this manual, since every case is different and would
require specific treatment. However, in general terms,
within the process of participatory research, there are
always results that can and should be shared with the
stakeholders--as they emerge, and within reasonable
time frames. For example, if discussion meetings are
conducted in a community and the results are returned
more than a year later, by that time, there is no
continuity and the process breaks down. In the same
way, there is information that can be useful to the
decision makers and should be passed on to them as it
is uncovered.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
It is necessary to work within deadlines and
offer useful outputs to the players involved
(communities and decision makers) as the
initiative progresses.
Yet, at the same time that useful outputs are
offered, both to the community and to decision
makers, it is important to keep in mind that the
process we have begun takes time and requires
“the work of ants”—one grain of sand at a time.
The success of this type of initiative is
measured more in terms of the quality of
participation and the long range benefits than in
terms of numbers of people or communities
covered and the short term impact of the
activities.
It is necessary to educate those involved and the
decision makers, especially those most
accustomed to working to produce concrete
outputs, concerning the nature and implications
of a participatory activity within the processes
of long term change.
The “knots,” or bonds of trust and
collaboration, are both outputs and processes.
It is important, therefore, to achieve a balance
between short term outputs and long term
processes.
There is no doubt that dialogue and participation, like
the knots in the tapestry, have a usefulness and a
purpose that translate—and should be translated—into
concrete results. The communities themselves insist
time and again on seeing these results, and that their
participation not be “in vain.”19
At the same time, the
value of dialogue and participation is that they have to
do with processes that represent continuity and
promote the long term sustainability of initiatives. In
effect, it is through dialogue and participation that
community members take ownership of initiatives and
acquire the tools that will enable them to ensure their
continuity over time.
The “knots” have a past, a present, and a future.
Dialogue and participation, like the knots in a
tapestry, become part of the history of the community,
helping it to redeem its past, analyze its present, and
develop a common vision for a better future. The
purpose of this manual has been to not only
familiarize the reader with the methodology of
participatory research through participatory video
discussion meetings, but also to share some ideas to
think about concerning its use in the wider context of
working with communities in a participatory way.
19
According to the results of the discussion meetings conducted in
Momostenango and in Zona Reina.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
PART IV. APPENDICES
APPENDIX 1
DISCUSSION GUIDE
THE DATA COLLECTION INSTRUMENT
FOR PARTICIPATORY VIDEO DISCUSSION MEETINGS INTRODUCING THE PROJECT AND THE TEAM The facilitator
Explains, in general terms, the objective of the
meeting and thanks the participants for coming.
Explains to the participants that the information
they share will be confidential and anonymous.
Explains the need to record the session to have a
“souvenir” of the meeting (he can offer, where
possible, to let them see the tape later).2O If
possible, he should ask their permission to make
the tape, assuring them once again of their
anonymity and confidentiality.
Explains to them that they will watch together a
couple of short videos that have been prepared for
the meeting, and that they will converse informally
about what each person thinks.
Asks them to interrupt him at any time if there is
anything that is not clear.
Introduces the other members of the team by name
and function (during the meeting). It is suggested
that their positions in the health care system not be
mentioned, to avoid bias.
Explains to them that they are going to begin with
a short exercise to get to know each other better.
20
It is very important to ensure the confidentiality and anonymity of the participants. To reassure them more concretely, the ideal would be for those of one region to meet with users of ANOTHER region than their own. Or, as we have agreed, that those who facilitate be people from the outside with good facilitation skills. Take care that the health workers who sometimes play the role of participating observers do not affect the outcome by their very presence.
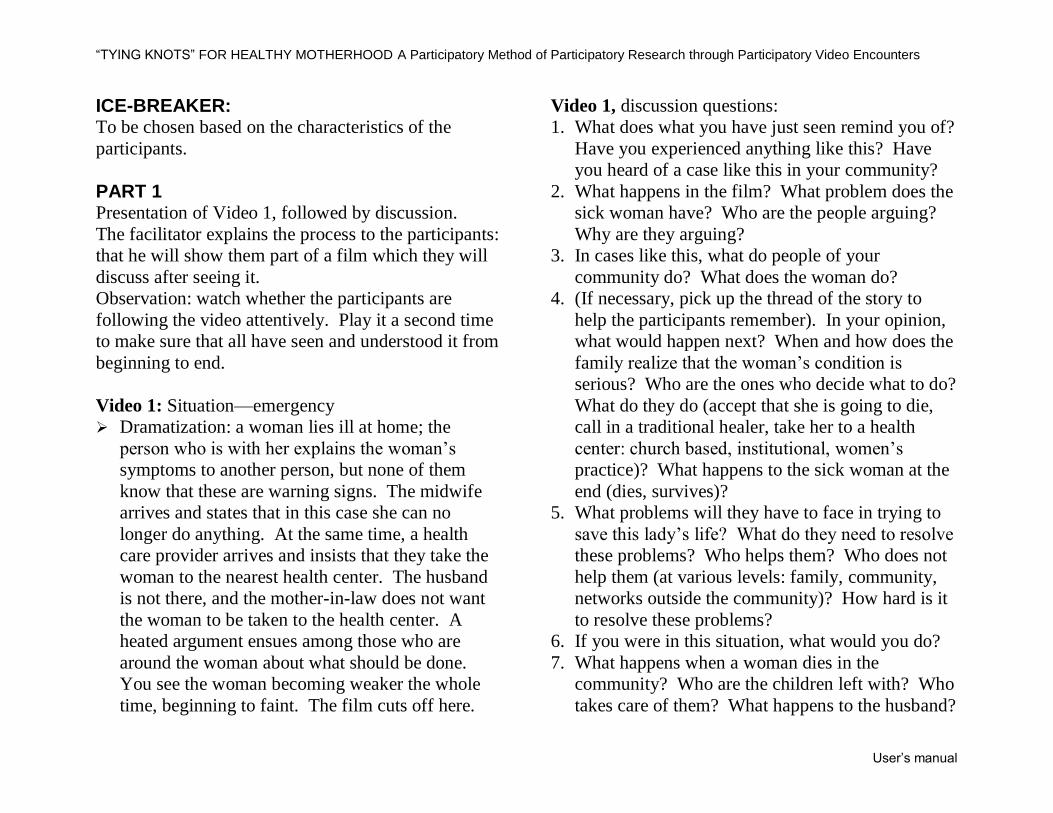
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
ICE-BREAKER: To be chosen based on the characteristics of the
participants.
PART 1 Presentation of Video 1, followed by discussion.
The facilitator explains the process to the participants:
that he will show them part of a film which they will
discuss after seeing it.
Observation: watch whether the participants are
following the video attentively. Play it a second time
to make sure that all have seen and understood it from
beginning to end.
Video 1: Situation—emergency
Dramatization: a woman lies ill at home; the
person who is with her explains the woman’s
symptoms to another person, but none of them
know that these are warning signs. The midwife
arrives and states that in this case she can no
longer do anything. At the same time, a health
care provider arrives and insists that they take the
woman to the nearest health center. The husband
is not there, and the mother-in-law does not want
the woman to be taken to the health center. A
heated argument ensues among those who are
around the woman about what should be done.
You see the woman becoming weaker the whole
time, beginning to faint. The film cuts off here.
Video 1, discussion questions:
1. What does what you have just seen remind you of?
Have you experienced anything like this? Have
you heard of a case like this in your community?
2. What happens in the film? What problem does the
sick woman have? Who are the people arguing?
Why are they arguing?
3. In cases like this, what do people of your
community do? What does the woman do?
4. (If necessary, pick up the thread of the story to
help the participants remember). In your opinion,
what would happen next? When and how does the
family realize that the woman’s condition is
serious? Who are the ones who decide what to do?
What do they do (accept that she is going to die,
call in a traditional healer, take her to a health
center: church based, institutional, women’s
practice)? What happens to the sick woman at the
end (dies, survives)?
5. What problems will they have to face in trying to
save this lady’s life? What do they need to resolve
these problems? Who helps them? Who does not
help them (at various levels: family, community,
networks outside the community)? How hard is it
to resolve these problems?
6. If you were in this situation, what would you do?
7. What happens when a woman dies in the
community? Who are the children left with? Who
takes care of them? What happens to the husband?
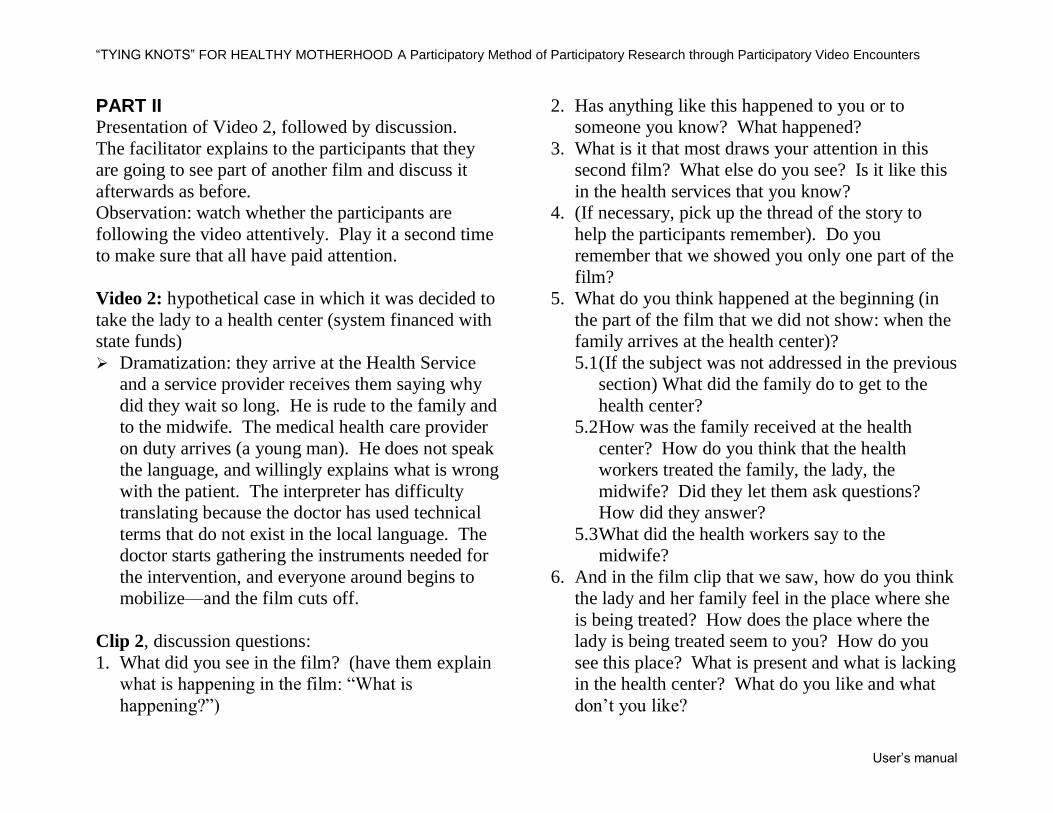
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
PART II Presentation of Video 2, followed by discussion.
The facilitator explains to the participants that they
are going to see part of another film and discuss it
afterwards as before.
Observation: watch whether the participants are
following the video attentively. Play it a second time
to make sure that all have paid attention.
Video 2: hypothetical case in which it was decided to
take the lady to a health center (system financed with
state funds)
Dramatization: they arrive at the Health Service
and a service provider receives them saying why
did they wait so long. He is rude to the family and
to the midwife. The medical health care provider
on duty arrives (a young man). He does not speak
the language, and willingly explains what is wrong
with the patient. The interpreter has difficulty
translating because the doctor has used technical
terms that do not exist in the local language. The
doctor starts gathering the instruments needed for
the intervention, and everyone around begins to
mobilize—and the film cuts off.
Clip 2, discussion questions:
1. What did you see in the film? (have them explain
what is happening in the film: “What is
happening?”)
2. Has anything like this happened to you or to
someone you know? What happened?
3. What is it that most draws your attention in this
second film? What else do you see? Is it like this
in the health services that you know?
4. (If necessary, pick up the thread of the story to
help the participants remember). Do you
remember that we showed you only one part of the
film?
5. What do you think happened at the beginning (in
the part of the film that we did not show: when the
family arrives at the health center)?
5.1 (If the subject was not addressed in the previous
section) What did the family do to get to the
health center?
5.2 How was the family received at the health
center? How do you think that the health
workers treated the family, the lady, the
midwife? Did they let them ask questions?
How did they answer?
5.3 What did the health workers say to the
midwife?
6. And in the film clip that we saw, how do you think
the lady and her family feel in the place where she
is being treated? How does the place where the
lady is being treated seem to you? How do you
see this place? What is present and what is lacking
in the health center? What do you like and what
don’t you like?
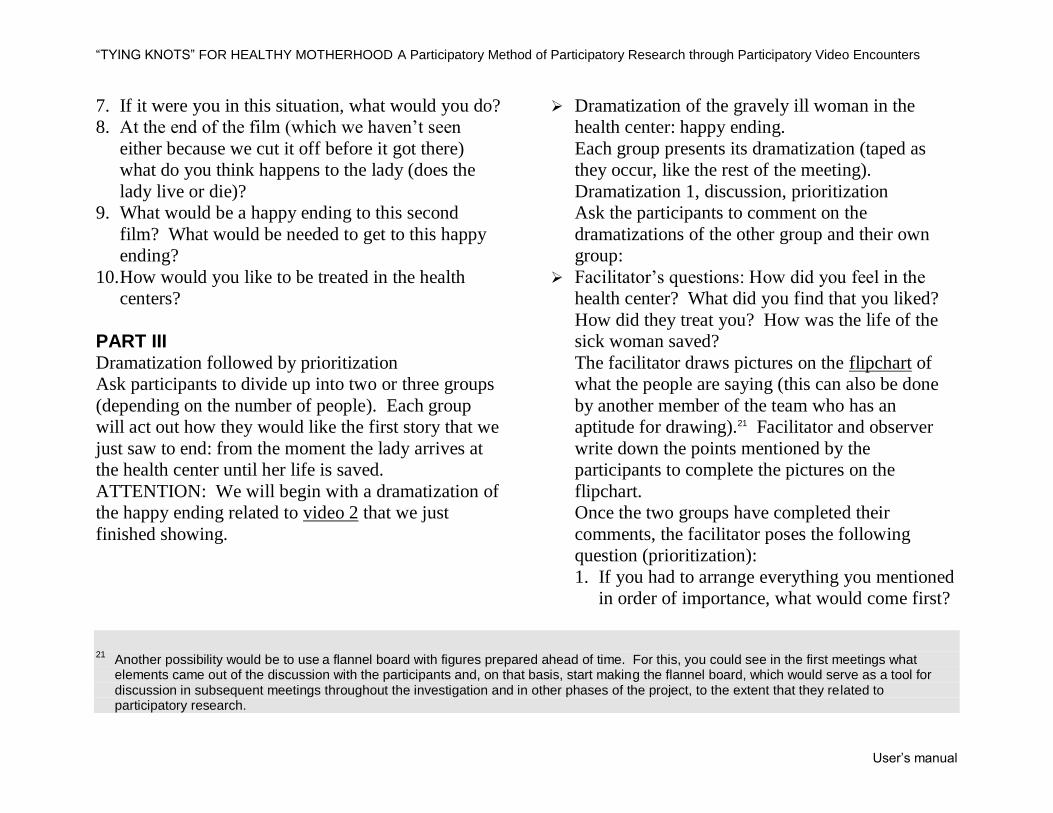
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
7. If it were you in this situation, what would you do?
8. At the end of the film (which we haven’t seen
either because we cut it off before it got there)
what do you think happens to the lady (does the
lady live or die)?
9. What would be a happy ending to this second
film? What would be needed to get to this happy
ending?
10. How would you like to be treated in the health
centers?
PART III Dramatization followed by prioritization
Ask participants to divide up into two or three groups
(depending on the number of people). Each group
will act out how they would like the first story that we
just saw to end: from the moment the lady arrives at
the health center until her life is saved.
ATTENTION: We will begin with a dramatization of
the happy ending related to video 2 that we just
finished showing.
Dramatization of the gravely ill woman in the
health center: happy ending.
Each group presents its dramatization (taped as
they occur, like the rest of the meeting).
Dramatization 1, discussion, prioritization
Ask the participants to comment on the
dramatizations of the other group and their own
group:
Facilitator’s questions: How did you feel in the
health center? What did you find that you liked?
How did they treat you? How was the life of the
sick woman saved?
The facilitator draws pictures on the flipchart of
what the people are saying (this can also be done
by another member of the team who has an
aptitude for drawing).21 Facilitator and observer
write down the points mentioned by the
participants to complete the pictures on the
flipchart.
Once the two groups have completed their
comments, the facilitator poses the following
question (prioritization):
1. If you had to arrange everything you mentioned
in order of importance, what would come first?
21
Another possibility would be to use a flannel board with figures prepared ahead of time. For this, you could see in the first meetings what
elements came out of the discussion with the participants and, on that basis, start making the flannel board, which would serve as a tool for discussion in subsequent meetings throughout the investigation and in other phases of the project, to the extent that they related to participatory research.
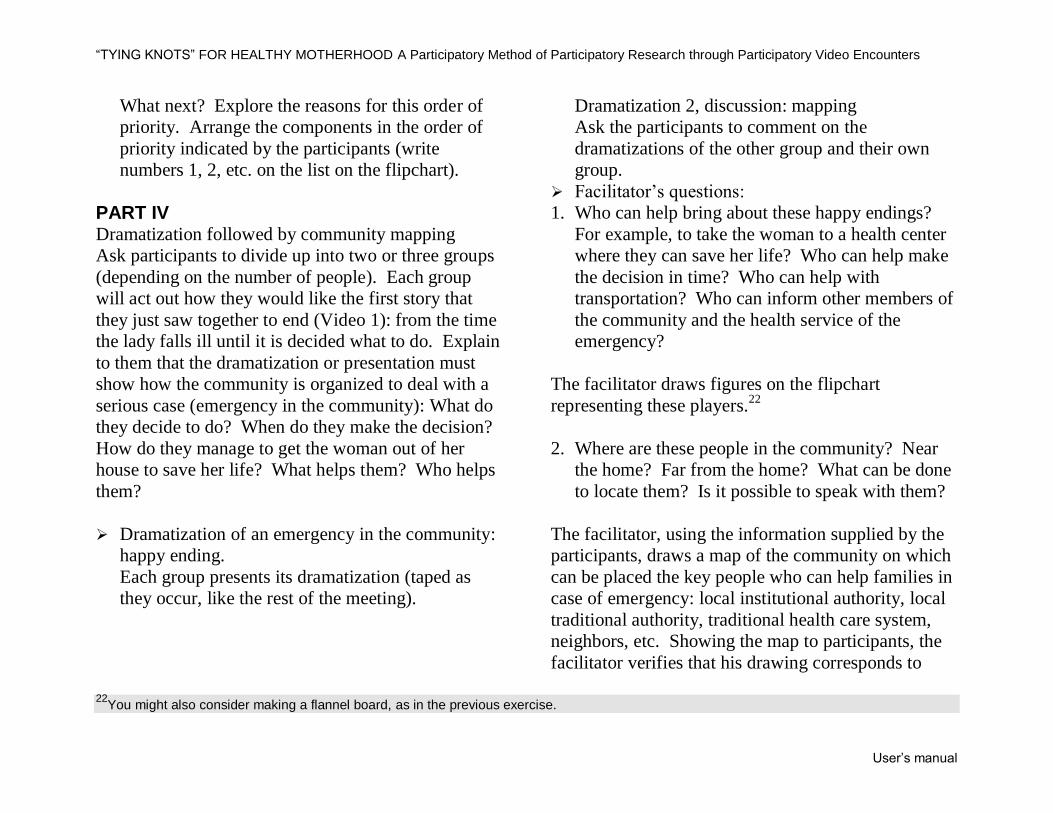
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
What next? Explore the reasons for this order of
priority. Arrange the components in the order of
priority indicated by the participants (write
numbers 1, 2, etc. on the list on the flipchart).
PART IV Dramatization followed by community mapping
Ask participants to divide up into two or three groups
(depending on the number of people). Each group
will act out how they would like the first story that
they just saw together to end (Video 1): from the time
the lady falls ill until it is decided what to do. Explain
to them that the dramatization or presentation must
show how the community is organized to deal with a
serious case (emergency in the community): What do
they decide to do? When do they make the decision?
How do they manage to get the woman out of her
house to save her life? What helps them? Who helps
them?
Dramatization of an emergency in the community:
happy ending.
Each group presents its dramatization (taped as
they occur, like the rest of the meeting).
Dramatization 2, discussion: mapping
Ask the participants to comment on the
dramatizations of the other group and their own
group.
Facilitator’s questions:
1. Who can help bring about these happy endings?
For example, to take the woman to a health center
where they can save her life? Who can help make
the decision in time? Who can help with
transportation? Who can inform other members of
the community and the health service of the
emergency?
The facilitator draws figures on the flipchart
representing these players.22
2. Where are these people in the community? Near
the home? Far from the home? What can be done
to locate them? Is it possible to speak with them?
The facilitator, using the information supplied by the
participants, draws a map of the community on which
can be placed the key people who can help families in
case of emergency: local institutional authority, local
traditional authority, traditional health care system,
neighbors, etc. Showing the map to participants, the
facilitator verifies that his drawing corresponds to
22
You might also consider making a flannel board, as in the previous exercise.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
what they said, and poses a final question to the
group:
3. What can the community do to help in emergency
cases? Can we all work together to save lives?
Conclude the meeting by:
Explaining that the objective is really to work with the
community to improve health services, to help them
prevent health problems, and support them in dealing
with emergencies in order to save lives. Reiterate that
we are engaged in a long term process, and this is
only the beginning. Thank them for their participation
and invite them to make their final comments (if they
have anything to add). Then conclude the
conversation by explaining what the follow-up will
be. In doing this, it is suggested that you reiterate that
this is the beginning of a common endeavor; that we
will be returning to the communities to continue the
process.
NOTE: As follow-up to this investigation, you might
hold a debriefing session with the community on the
results of the participatory research, in the form of
developing local emergency plans (the name to be
given to this type of initiative will come out of the
groups themselves). We should not forget to involve
(in one way or another) the people who agreed to
participate in the discussion and in the other phases of
the project.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 2
A FEW TIPS
Basic Rules:
I. Practice “active listening” That means, listen in a way that communicates
respect, interest, and empathy. These attitudes
can be conveyed verbally and non verbally.
How can I verbally communicate to the person
that I am listening to him/her?
How can I non verbally communicate to the
person that I am listening to him/her?
II. Use language that is simple and clear
No professional jargon
Use terms that the participants understand
Culturally appropriate language
Some techniques for clarifying answers or probing into what a person is saying:
1. Paraphrasing: that is, repeating in other words
what the person has just said
Example:
2. Posing follow-up or “checking” questions: this
is a KEY technique in this kind of
investigation. It is used to understand the
reasons for people’s behaviors, attitudes, or
motivations. It is a question that CLARIFIES
an answer given by someone. It helps us to
PROBE a point that we consider important.
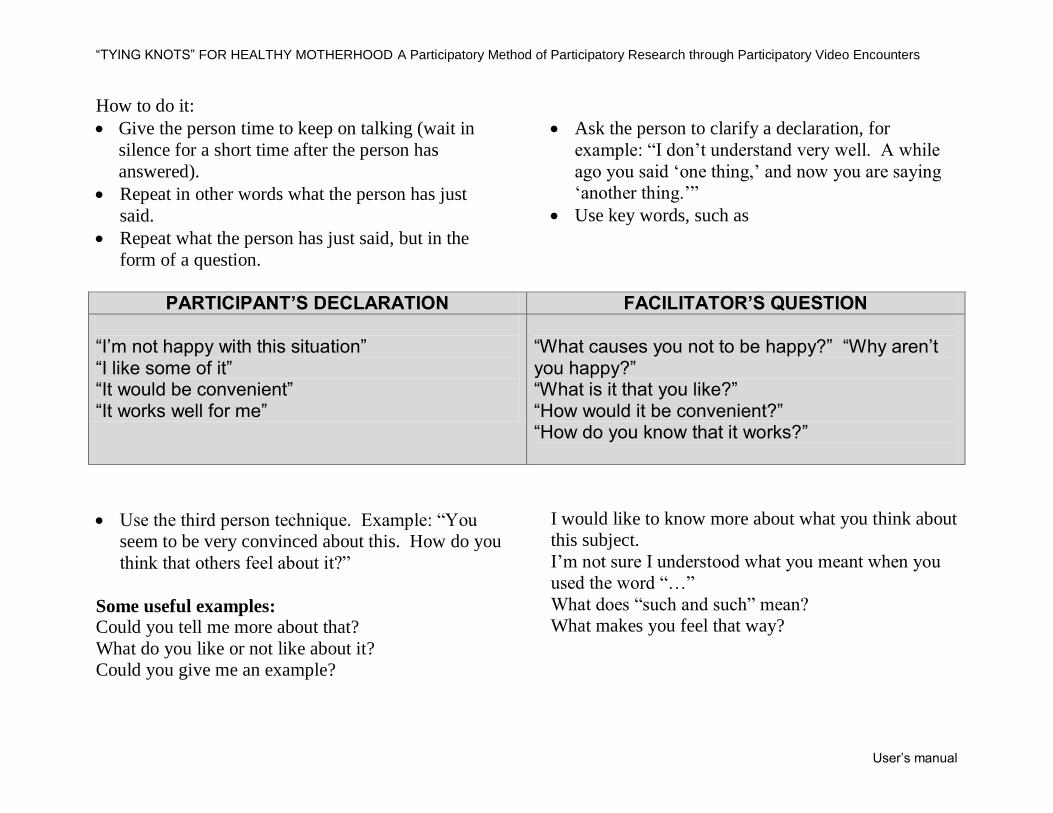
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
How to do it:
Give the person time to keep on talking (wait in
silence for a short time after the person has
answered).
Repeat in other words what the person has just
said.
Repeat what the person has just said, but in the
form of a question.
Ask the person to clarify a declaration, for
example: “I don’t understand very well. A while
ago you said ‘one thing,’ and now you are saying
‘another thing.’”
Use key words, such as
PARTICIPANT’S DECLARATION FACILITATOR’S QUESTION
“I’m not happy with this situation” “I like some of it” “It would be convenient” “It works well for me”
“What causes you not to be happy?” “Why aren’t you happy?” “What is it that you like?” “How would it be convenient?” “How do you know that it works?”
Use the third person technique. Example: “You
seem to be very convinced about this. How do you
think that others feel about it?”
Some useful examples: Could you tell me more about that?
What do you like or not like about it?
Could you give me an example?
I would like to know more about what you think about
this subject.
I’m not sure I understood what you meant when you
used the word “…”
What does “such and such” mean?
What makes you feel that way?
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Why do we need to use these kinds of questions? Because:
Sometimes it is necessary to get information out of
people “with a teaspoon.”
It is often difficult for people to talk about what
they FEEL.
We can misinterpret what a person says to us.
Thus, you will use this type of question when:
You have not completely understood what the
person said;
You want more details or specific examples;
You are trying to uncover feelings and
motivations;
You are not familiar with the terms that the person
is using;
You think the person is saying only part of what he
is thinking.
3. Giving “positive feedback”
That is, praise or encourage the person concerning
what he says he has done. This helps people feel
more comfortable with the facilitator (who is not
making value judgments and not “criticizing” the
person), and thus encourages them to give more
information. This technique can also help
reinforce a desired behavior. Sometimes this is
difficult to do because the person could be
describing a behavior we disapprove of or consider
“bad.” Example: a man decided not to take his
wife to the health center but then realized that it
would have been better to have taken her. The
facilitator can say to him, “It’s good that you have
realized it would have been better to take her.
What made you change your mind? What would
you do now?”
Other advice:
4. Avoid questions that lead to “yes” or “no”
answers, that is, closed questions.
5. Rephrase questions when necessary to ensure
understanding and cultural adaptation.
6. Don’t give the impression that you are testing the
participants’ knowledge.
7. Put yourself in the participants’ place to see if you
would feel threatened by a particular question or
the way it is formulated.
8. Don’t guess any answer. What you think might
not coincide with what the other person is
thinking.
9. Don’t include ANSWERS in your questions.
10. If people are speaking in a “neutral” manner about
a subject, or if the participants are not talking, you
can sometimes play the “devil’s advocate,” always
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
being careful not to obstruct the process of
communication.
11. Remember that you are leading a group discussion
and not individual interviews. Refer the comments
and answers of one participant to the group to
encourage other comments. Connect the answers
of different participants to further explore a
subject.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 3
TABLE OF HUMAN RESOURCES
Municipality:
Community:
Team* Group
Facilitator Participating
Observer Camera
Operator Other
(specify) Date
Women
Midwives
Leaders
Men
*The pilot, responsible for transportation into the
community, is also a key member of the team. If it
is considered necessary, a specific column can be
added to include him in the table.
In some cases, the pilot might also attend to other
tasks during the discussion meetings, such as camera
operator, for example.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 4
CHECKLIST FOR MATERIALS AND SUPPLIES
MUNICIPALITY:
COMMUNITY:
DATE:
MATERIAL NUMBER CONFIRMED TO BE CONFIRMED
1. -TEAM
Television
VHS
Audio tape recorder
90 min. cassettes
Adaptors
Extension
Microphones (AAA batteries, recharge. battery)
2. –SUPPORT MATERIAL
A. Videos (video clips-short films)
B. Graphic material
C. Flannel board or figures (if it is decided to use these materials instead of drawing)
D. Participant identification
Name tags
Table with socio-demographic information Sheet with list of participants
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
MATERIAL NUMBER CONFIRMED TO BE CONFIRMED
E. Other supplies
Masking tape
Flip charts
Permanent markers
Scissors
Tacks
3. -REFRESHMENTS
List of participants
Refreshments
Soap(*)
Towels(*)
Basin(*)
4. –OTHER ITEMS
Balls or candy for the children
(*) These are some ideal materials to make it easy for the participants to wash their hands before eating.
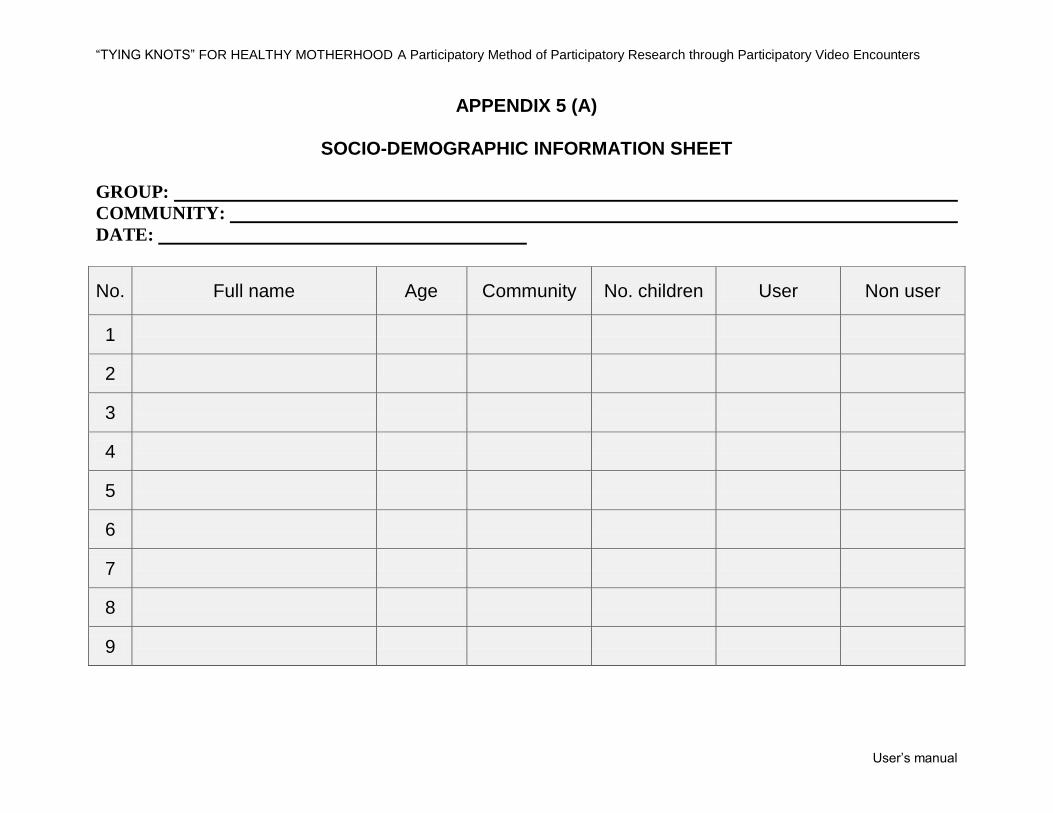
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 5 (A)
SOCIO-DEMOGRAPHIC INFORMATION SHEET
GROUP:
COMMUNITY:
DATE:
No. Full name Age Community No. children User Non user
1
2
3
4
5
6
7
8
9
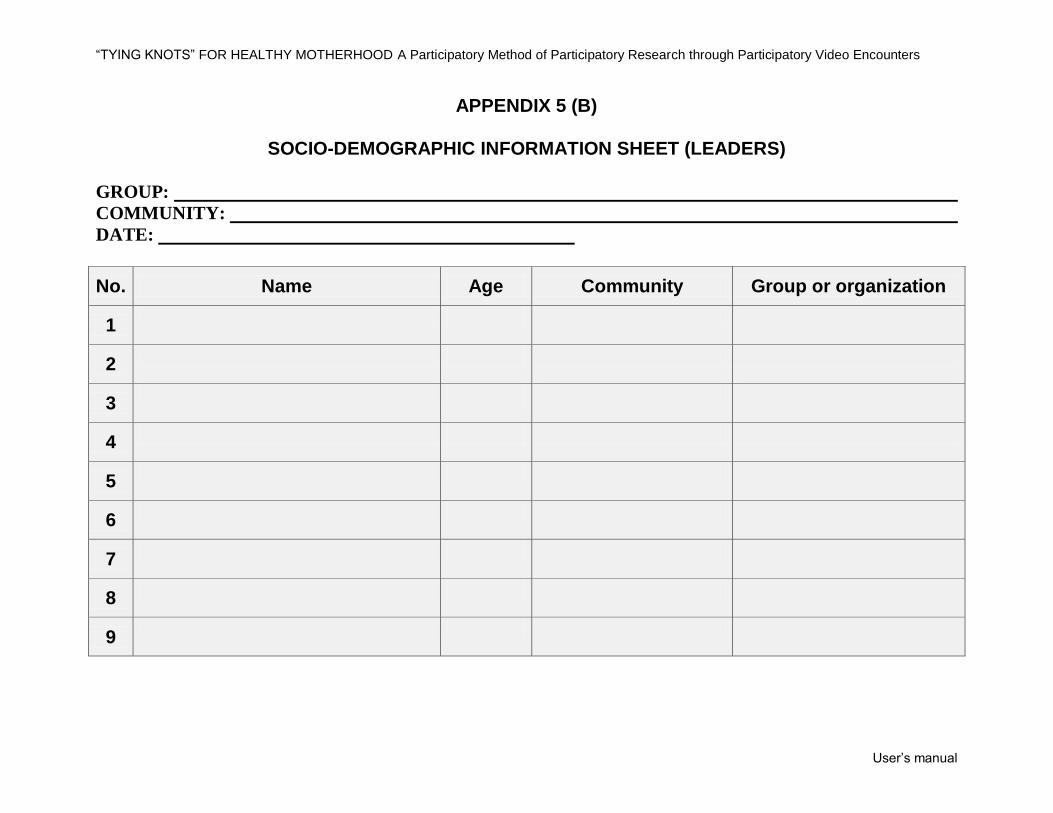
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 5 (B)
SOCIO-DEMOGRAPHIC INFORMATION SHEET (LEADERS)
GROUP:
COMMUNITY:
DATE:
No. Name Age Community Group or organization
1
2
3
4
5
6
7
8
9
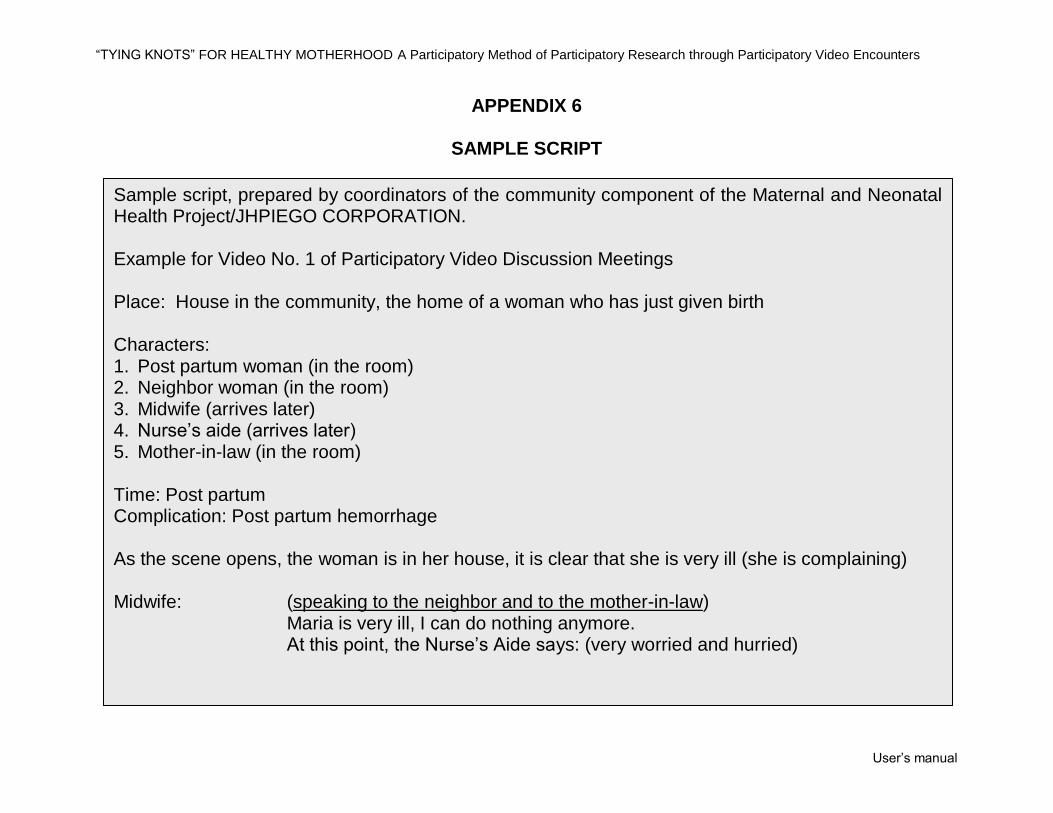
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 6
SAMPLE SCRIPT
Sample script, prepared by coordinators of the community component of the Maternal and Neonatal Health Project/JHPIEGO CORPORATION. Example for Video No. 1 of Participatory Video Discussion Meetings Place: House in the community, the home of a woman who has just given birth Characters: 1. Post partum woman (in the room) 2. Neighbor woman (in the room) 3. Midwife (arrives later) 4. Nurse’s aide (arrives later) 5. Mother-in-law (in the room) Time: Post partum Complication: Post partum hemorrhage As the scene opens, the woman is in her house, it is clear that she is very ill (she is complaining) Midwife:
(speaking to the neighbor and to the mother-in-law) Maria is very ill, I can do nothing anymore. At this point, the Nurse’s Aide says: (very worried and hurried)
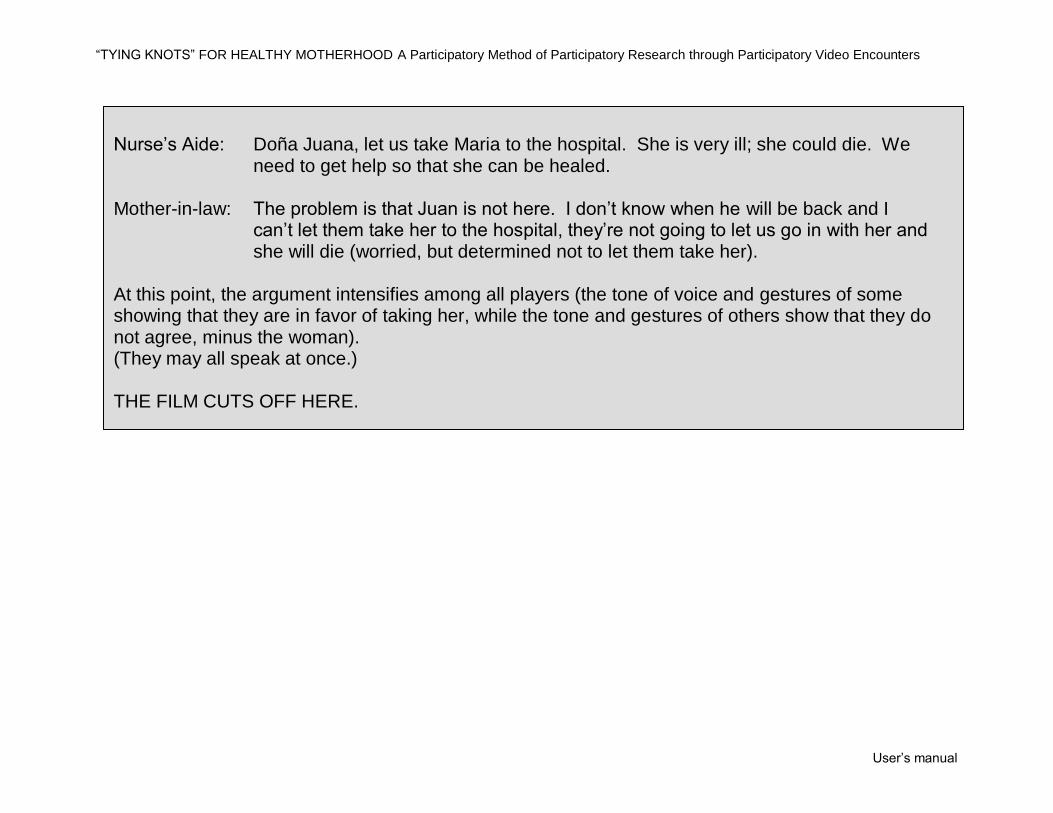
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
Nurse’s Aide:
Doña Juana, let us take Maria to the hospital. She is very ill; she could die. We need to get help so that she can be healed.
Mother-in-law:
The problem is that Juan is not here. I don’t know when he will be back and I can’t let them take her to the hospital, they’re not going to let us go in with her and she will die (worried, but determined not to let them take her).
At this point, the argument intensifies among all players (the tone of voice and gestures of some showing that they are in favor of taking her, while the tone and gestures of others show that they do not agree, minus the woman). (They may all speak at once.) THE FILM CUTS OFF HERE.
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual
APPENDIX 7
SOME TIPS ON TRANSCRIBING
The format that the person uses to transcribe the
information will depend on how the transcript will be
used. Thus, if the meeting has been video taped and
the intention is to edit the tape, a format will be used
that will allow the images to be matched with the text.
If the intention is to use the transcript for an analysis
of the discourse (verbal) of the participants, it will
suffice to transcribe the verbal statements of the
participants.
Some instructions for transcribing
Indicate who is speaking in each case.
Translate what the person says as he says it.
Do not summarize or synthesize what the person is saying.
When it is difficult or impossible to translate words into Spanish (because they do not exist in our
vocabulary), write them in the local language and explain in parentheses what they mean, even if that means
giving a detailed explanation of the meaning.
When the literal translation of the word illustrates ways of thinking or looking at the world, stick to the
“literal” translation and explain in parentheses what the word means in context (for example, if the person
uses the term “filthiness” to refer to menstruation, write “filthiness” and explain in parentheses what it
means).
“TYING KNOTS” FOR HEALTHY MOTHERHOOD A Participatory Method of Participatory Research through Participatory Video Encounters
User’s manual