Vestibular Presentation
46
Vestibular Physical Therapy in the Inpatient Setting A brief introduction and helpful tips for diagnosis, treatment, and proper referral Nathan Dugan, PT, DPT Kalispell Regional Medical Center January 20, 2016
-
Upload
nathan-dugan-pt-dpt -
Category
Documents
-
view
534 -
download
2
Transcript of Vestibular Presentation

Vestibular Physical Therapy in the Inpatient SettingA brief introduction and helpful tips for diagnosis, treatment, and proper referral
Nathan Dugan, PT, DPT Kalispell Regional Medical CenterJanuary 20, 2016

Objectives
● Overview of the vestibular system○ Anatomy and physiology○ Vestibular disorders
● History taking● Screening● Oculomotor/vestibular assessment
○ Tests and measures○ Outcome measures
● BPPV diagnosis and treatment● Outpatient vestibular therapy● Practical portion

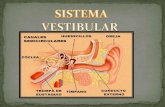
Vestibular Anatomy and Physiology

Vestibular AnatomyBony Labyrinth
● 3 semicircular canals (SCCs), cochlea, vestibule (central chamber)
Membranous Labyrinth● Suspended within bony labyrinth by
perilymphatic fluid● Contains 5 sensory organs
○ Membranous portions of SCCs
○ Otolith organs■ Utricle■ Saccule

Vestibular Anatomy
Hair Cells
● Contained in each ampulla and otolith organ, convert displacement of the head into neural firing

Vestibular Anatomy
Semicircular Canals
● Register angular rotations and velocity of the head● Anterior, posterior, and horizontal
○ Arranged perpendicularly to each other, form coplanar pairs
● Each coplanar pair forms a push-pull relationship○ Why is this important?

Vestibular Anatomy
Otolith Organs
● Register forces related to linear acceleration (linear head motion/tilt)● Saccule
○ Vertical○ Senses anterior-posterior and occipital-caudal motion
● Utricle○ Horizontal○ Senses anterior-posterior and interaural motion

Vestibular Reflexes
Vestibulo-ocular Reflex (VOR)
● Acts to maintain stable vision during head motion● With head turn to the left
○ Firing rate from hair cells in left increase, right decrease○ Excitatory impulses transmitted to ipsilateral medial rectus/contralateral lateral rectus○ Inhibitory impulses transmitted to antagonists○ If retinal image motion is >2 deg/sec, firing rate is modified - VOR IS TRAINABLE
Vestibulospinal Reflex (VSR)
Vestibulocollic Reflex (VCR)

Cervical Reflexes
Cervico-ocular Reflex (COR)
● Interacts with VOR● Eye movements driven by neck proprioceptors● Facilitated when vestibular apparatus is injured, however it is rare that COR
has any clinical significance
Cervicospinal Reflex (CSR)
● Acts when body is rotated on stable head
Cervicocollic Reflex (CCR)

Vestibular DisordersTypical clinical presentations of common disorders

Vestibular Disorders - Clinical PresentationBenign Paroxysmal Positional Vertigo (BPPV)
● Vertigo lasting 30 seconds to 2 minutes○ Disappears even if offending head position
is maintained○ Usually self-limiting and resolves
spontaneously within 6-12 months● Brought about by assuming specific head
postures● Common in elderly, any age group after
mild head trauma, F > M● Very specific nystagmus patterns
depending on canal involvement● HEARING LOSS, TINNITUS, AURAL
FULLNESS NOT SEEN WITH BPPV
Vestibular Neuritis
● Sudden onset vertigo lasting 48-72 hours○ Exacerbated by head movement○ Associated with horizontal - rotatory
nystagmus, postural imbalance, nausea○ Normal balance returns in ~6 weeks
● Often preceded by a viral infection of upper respiratory or GI tract (up to 2 weeks)
● Age of onset: 30-60 years○ Female peak: 40s○ Male peak: 60s

Vestibular Disorders - Clinical PresentationMeniere’s Disease/Endolymphatic Hydrops
● Episodic in nature, over many years● AURAL FULLNESS, HEARING LOSS,
TINNITUS○ Accompanied by vertigo, imbalance,
nystagmus, nausea, vomiting○ Vertigo persists from 30 minutes to 24
hours○ Patient generally ambulatory within 72
hours● Hearing generally returns but will
eventually fail to return as disease progresses
● Usually burns itself out● Age of onset: 40-60 years
Perilymphatic Fistula/Superior SCC Dehiscence
● Patient generally has a history of trauma, may report a “pop”
● May lead to episodic vertigo and sensorineural hearing loss
● Tullio phenomenon○ Vestibular symptoms caused by auditory
stimuli● Rest generally alleviates symptoms
○ Sneezing, nose blowing may precipitate

Vestibular Disorders - Clinical PresentationVestibular Migraine
● Migraine is a common cause of vertigo and disequilibrium
● Question about headaches and migraines to determine a link with vestibular symptoms
● Greater incidence of motion sickness associated with migraine
Mal de Debarquement Syndrome
● Defined by prolonged/inappropriate sensations of movement after exposure to motion
● Occurs after activity such as boat trip, airplane travel, train travel, etc
● Persistence of symptoms for >/= 1 month● Find relief when moving

History TakingWhat is important to know?

History Taking
● The MOST IMPORTANT part of the initial evaluation○ Devote some time to this area
● Clinical symptoms will likely begin to lead you to a diagnosis
● This is a big part of what separates a good vestibular therapist from other medical professionals with less knowledge about the vestibular system
● BPPV is a “catch-all” diagnosis

History Taking
Elements that help with diagnosis
1. Tempo2. Symptoms3. Circumstances

History Taking - Tempo
● Acute or chronic (>3 days)?● FIRST onset of dizziness
○ Sudden or slowly developing?○ Provoked or spontaneous?○ Prior illness?
● Average duration of spells

History Taking - Symptoms
● What does dizzy mean?○ Disequilibrium ○ Lightheadedness ○ Rocking/swaying ○ Motion sickness ○ Nausea/vomiting ○ Oscillopsia ○ Floating/swimming/rocking/spinning ○ Vertigo

History Taking - Circumstance
Under what circumstance does the patient’s dizziness occur?
● With certain movements?● Spontaneously?● Exacerbated by head/visual movement?

History Taking - Other Considerations
● Often a psychological component to vestibular disorders● What medications is the patient taking?

Screening TestsTo rule out non-vestibular causes of vertigo

HINTS1
Head Impulse, Nystagmus, Test of Skew
Indicative of stroke:
INFARCT
Impulse Normal, Fast-phase Alternating, Refixation on Cover Test
HINTS plus Hearing

Head Impulse Test
Video: https://www.youtube.com/watch?v=fiqAkhYNPRk

Direction-Changing Nystagmus
Video: https://www.youtube.com/watch?v=0rHNappbYtE

Skew Deviation
Video: https://www.youtube.com/watch?v=-J170K7VAdA

Vertebral Artery Screening
● VBI often presents with vertigo, nausea, and vomiting○ Other symptoms are important in history
● Clinical tests - poor sensitivity○ Vertebral artery compression test (VAT)
■ Performed in supine with full cervical rotation/extension● What might be wrong with this?
○ Modified VAT (mVAT)■ Patient is in sitting
● Then rotates head to one side and flexes forward at hips thus extending the cervical spine

Vestibular Assessment

Oculomotor/Vestibular Examination

Oculomotor/Vestibulo-Ocular Examination
● Convergence● Smooth Pursuit
○ Combine with test for gaze-evoked nystagmus for efficiency
● Saccades● Spontaneous Nystagmus● Gaze-Evoked Nystagmus● Skew Deviation● VOR Cancellation

VOR Testing
● Head Impulse Test● Head-Shaking Nystagmus● Dynamic Visual Acuity● VOR I/II

Outcome MeasuresWhat measures have been validated in the vestibular disorder population?

Functional Gait Assessment (FGA)
● Modification of DGI to improve reliability and decrease ceiling effect● 10 items scored 0-3 for total possible score of 30● May be performed with or without assistive devices● Equipment
○ Stop watch○ 20ft x 12in walking path○ 9in obstacle (2 shoe boxes)○ Steps
● Cut-off scores2
○ </= 22/30 predicts falls (older adult data)■ Sensitivity 85%, Specificity 86%

Timed Up-and-Go (TUG)
● 3m (10ft) course, with patient seated in chair to start, and turn in middle● Timing begins on “go” and ends when patient sits
○ One practice trial should be given
● In vestibular population, both right and left turns should be tested● Cut-off scores3
○ >11.1s■ Sensitivity 80%, Specificity 56%

BPPV Diagnosis and Treatment

BPPV
● The only vestibular diagnosis that you can fix with one treatment○ Therefore it is a great skill for any physical therapist to have
● Remember○ Characterized by episodic vertigo precipitated by position changes that last for 30s - 2min and
is fatiguing even if the offending head position is maintained○ Characteristic nystagmus patterns
● Diagnosis can be difficult without the use of Frenzel/infrared goggles○ Why?

BPPV Mechanism
● Canalithiasis○ Debris dislodged from the otoconia becomes freely floating in the endolymph of an SCC
○ Head movement causes movement of the otoconia which in turn causes movement of the endolymph, thus deflecting the cupula
■ Delay in onset of vertigo/nystagmus up to 40 seconds■ Vertigo generally rises in intensity to a peak, and then improves rapidly and disappears
● Cupulolithiasis○ Debris dislodged from the otoconia becomes adhered to the cupula
■ Causes sudden onset vertigo/nystagmus that is non-fatiguing○ Relatively uncommon
● Treatments for canalithiasis and cupulolithiasis are different

Types of BPPV - Posterior Canal
MOST COMMON - 76% of cases
● Diagnostic Test○ Dix - Hallpike
● Observed Nystagmus and Canal Involvement (Left Dix-Hallpike Test) ○ Left posterior canal - upbeating and left torsional○ Left anterior canal - downbeating and left torsional○ Right anterior canal - downbeating and right torsional
● Treatment○ Canalith Repositioning Treatment/Epley Maneuver (CRT)○ Liberatory/Semont Maneuver○ Brandt-Daroff exercises

Posterior Canal BPPV Nystagmus - Video
Video: https://www.youtube.com/watch?v=jrp8iPfvP4Y

Types of BPPV - Anterior Canal
13% of cases
● Diagnostic Test○ Dix - Hallpike
● Observed Nystagmus and Canal Involvement (Left Dix-Hallpike Test) ○ Left posterior canal - upbeating and left torsional○ Left anterior canal - downbeating and left torsional○ Right anterior canal - downbeating and right torsional
● Treatment○ Deep Head-Hanging Maneuver4
○ Canalith Repositioning Treatment/Epley Maneuver (CRT)○ Liberatory/Semont Maneuver○ Brandt-Daroff exercises

Anterior Canal BPPV Nystagmus - Video
Video: https://www.youtube.com/watch?v=qW-tBDU9RRc

Types of BPPV - Horizontal Canal
5% of cases
● Diagnostic Test○ Roll Test
● Observed Nystagmus and Canal Involvement○ Geotropic (towards floor)
■ Canalithiasis○ Apogeotropic (away from floor)
■ Cupulolithiasis○ Which side is involved?
■ More intense nystagmus/increased symptoms and duration on pathological side● Treatment
○ Bar-B-Que Roll (fast or slow), Appiani/Casani Maneuvers○ Forced prolonged positioning

Horizontal Canal BPPV Nystagmus - Video
Video: https://www.youtube.com/watch?v=MtmkD5rDU0o

BPPV Treatment
Lab Portion

Referring to Outpatient Vestibular Therapy
● When should you refer a patient to outpatient vestibular physical therapy?○ BPPV○ Other vestibular disorders
● What is outpatient vestibular physical therapy like?○ Habituation, adaptation, gaze stabilization, balance training
● How long does it take patients to recover?

Questions?

References1) Newman-Toker DE, Curthoys IS, Halmagyi GM. Diagnosing stroke in acute vertigo: the HINTS family
of eye movement tests and the future of the “eye ECG.” Semin Neurol 2015;35(5):506-521. 2) Wrisley DM, Kumar NA. Functional gait assessment: concurrent, discriminative, and predictive
validity in community-dwelling older adults. Phys Ther 2010;90(5):761-773.3) Whitney SL, Marchetti GF. The sensitivity and specificity of the timed up & go and the dynamic gait
index for self-reported falls in persons with vestibular disorders. J Vestib Res 2004;14: 397-409.4) Yacovino DA, Hain TC, Gualtieri F. New therapeutic maneuver for anterior canal benign paroxysmal
positional vertigo. J Neurol 2009:256(11);1851-1855.
All other slides adapted from:
Herdman SJ. Vestibular Rehabilitation, 3ed. Philadelphia: FA Davis; 2007.